
Abstract
Consumers often engage in unsafe food handling behaviors at home. Previous studies have investigated the ability of behavior-change theories to explain and predict these behaviors. The purpose of this review was to determine which theories are most consistently associated with consumers' safe food handling behaviors across the published literature. A standardized systematic review methodology was used, consisting of the following steps: comprehensive search strategy; relevance screening of identified references; confirmation of relevance and characterization of relevant articles; risk-of-bias assessment; data extraction; and descriptive analysis of study results. A total of 20 relevant studies were identified; they were mostly conducted in Australia (40%) and the United States (35%) and used a cross-sectional design (65%). Most studies targeted young adults (65%), and none focused on high-risk consumer groups. The outcomes of 70% of studies received high overall risk-of-bias ratings, largely due to a lack of control for confounding variables. The most commonly applied theory was the Theory of Planned Behavior (45% of studies), which, along with other investigated theories of behavior change, was frequently associated with consumer safe food handling behavioral intentions and behaviors. However, overall, there was wide variation in the specific constructs found to be significantly associated and in the percentage of variance explained in each outcome across studies. The results suggest that multiple theories of behavior change can help to explain consumer safe food handling behaviors and could be adopted to guide the development of future behavior-change interventions. In these contexts, theories should be appropriately selected and adapted to meet the needs of the specific target population and context of interest.
Introduction
F
Most sporadic cases of foodborne illness are estimated to occur in people's home (Redmond and Griffith, 2003), and in Europe, most reported outbreaks of foodborne illness are associated with private homes (EFSA and ECDC, 2016). However, consumers frequently underestimate their risk of acquiring foodborne illness at home compared to other settings, such as restaurants (Redmond and Griffith, 2003; Kennedy et al., 2011; Nesbitt et al., 2014). In addition, previous studies have found that various other psychosocial factors, such as perceived risks, lack of knowledge, imbedded habits, and limited self-confidence in how to perform safe food handling, can contribute to consumers' use of unsafe food handling behaviors at home (Byrd-Bredbenner et al., 2008; Fischer and Frewer, 2008; Abbot et al., 2009; Mullan et al., 2015).
Theories of behavior change can be used to identify and explain which combinations of different psychosocial factors are associated with consumer behaviors such as safe food handling (Mullan, 2010; Davis et al., 2015; Prestwich et al., 2015). Theories of behavior change provide a systematic view of the relationships between various psychosocial variables to explain and predict specific human behaviors (Glanz et al., 2015). By identifying the important psychosocial constructs that influence behavior, theories of behavior change provide a framework for developing more targeted, and potentially more effective, behavior-change interventions (Prestwich et al., 2015).
A previous scoping review of food safety education interventions for consumers found that only 27% of studies reported on an intervention that was based on a theory of behavior change (Sivaramalingam et al., 2015), indicating that increased adoption of theory-based approaches is warranted in this field. The characteristics and outcomes of studies that investigated the ability of behavior-change theories to explain consumers' safe food handling practices at home have not been previously synthesized using a formally structured and transparent approach.
We conducted a systematic review to identify, assess, and synthesize these studies. The review purpose was to determine which theories, and psychosocial constructs within each theory, are most consistently associated with consumers' safe food handling behaviors, and under what conditions. The results can help to inform the development of targeted, theory-based interventions to improve consumer safe food handling at home.
Materials and Methods
Review question and eligibility criteria
This systematic review was conducted according to a prespecified protocol and followed standardized methodology (Higgins and Green, 2011; Young et al., 2014). It is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guidelines (Moher et al., 2009). The review question was: “What is the relationship between behavior-change theories and safe food handling behaviors among adult consumers (aged ≥18 years old) who prepare and consume food at home?”
The research question was a subset of a larger systematic review that evaluated the association between various psychosocial factors and consumers' safe food handling behaviors. Data on the other components of the review are reported in a separate publication (Young et al., 2017). Outcomes of interest in this review included behavioral intentions and behaviors (self-reported or observed). Journal articles and gray literature sources (e.g., dissertations and conference proceedings) published in English, French, Spanish, or Italian were eligible for inclusion.
Search strategy
A comprehensive and pretested search strategy was developed in consultation with a librarian. It consisted of combinations of keywords in different categories: topic (e.g., food safety); population (e.g., consumers and adults); exposure (e.g., theory); and outcome (e.g., behaviors and practices). The search was implemented in nine bibliographic databases on July 4, 2016: Scopus, PubMed, CAB Abstracts, Food Safety and Technology Abstracts, PsycINFO, Cumulative Index to Nursing and Allied Health Literature, Health and Safety Science Abstracts, Risk Abstracts, and ProQuest Dissertations and Theses.
A complimentary search for gray literature was conducted using a series of 10 simple searches in Google (e.g., “consumer safe food handling theory”), and the search was verified by reviewing the reference lists of five review articles and all relevant articles. Additional search details, including full algorithms, are available as Supplementary Data (Supplementary Data are available online at
Reference management, relevance screening, and article characterization
Identified references were uploaded to RefWorks (Thomson ResearchSoft, Philadelphia, PA), duplicates were removed, and references were then imported into the web-based systematic review software DistillerSR (Evidence Partners, Ottawa, Canada) to facilitate further review steps. References were screened for relevance to the review question using a structured form consisting of one yes/no question. Full articles of potentially relevant references were obtained and confirmed for relevance using an article characterization form. This form also captured key characteristics from each article, such as citation information; study design and data collection methods; and details on targeted consumer population, behavior-change theories, and outcomes investigated. Both forms were pretested before use on 50 references and 5 studies, respectively.
Risk-of-bias assessment and data extraction
Relevant studies were assessed for their risk of bias, and relevant data were extracted using two additional forms. The risk-of-bias tool was adapted from published instruments (Thomas et al., 2004; Viswanathan et al., 2013; Sterne et al., 2016). It consisted of seven individual criteria, and an overall risk-of-bias rating for each study. The criteria were evaluated at the “outcome level,” considering the main outcomes of interest in each study. Outcomes of interest in this review included multivariable linear regression and structural equation modeling (SEM) that evaluated the impacts of behavior-change theories on consumers' safe food handling behaviors. The regression models simultaneously evaluated the contribution of multiple psychosocial constructs comprising each theory, sometimes adjusted for additional sociodemographic or other confounding variables.
The data extraction form was used to extract details on each outcome of interest in each study, including modeling approach, theory and psychosocial variables assessed, confounding variables adjusted for, and key model findings (e.g., R 2, which refers to the proportion of variation accounted for by the model). Both forms were pretested on five articles before use to ensure consistent interpretation among reviewers. All review steps were conducted by two independent reviewers. Copies of all forms used in this review are available as Supplementary Data.
Statistical analysis
Extracted data were downloaded as Microsoft Excel spreadsheets for formatting and descriptive analysis (Excel 2013; Microsoft Corporation, Redmond, WA). Data were stratified separately across five different behavioral construct categories: (1) adequate cooking of foods; (2) avoiding the consumption of unsafe foods; (3) prevention of cross-contamination and practicing personal hygiene; (4) time–temperature control; and (5) overall or composite food handling scores. The construct categories were adapted from those previously reported in the literature (Medeiros et al., 2001; Bearth et al., 2014; Mullan et al., 2015, 2016). Within each of these categories, descriptive tables and graphs were generated to summarize the data and explore trends in the model outcomes across studies (Mays et al., 2005; Higgins and Green, 2011). Statistical meta-analysis was not deemed appropriate due to the wide variability in methods and approaches used across studies.
Results
Characteristics of relevant articles
A summary of the review process is shown in Figure 1. From 4055 references that were screened for relevance, 20 studies met the eligibility criteria for this review. The characteristics of these studies are noted in Table 1. Studies were mostly conducted in Australia (40%) and the United States (35%) and used a cross-sectional design (65%). While 90% of studies were informed by formative research, only 35% reported pretesting of their data collection instruments (Table 1). The most commonly applied theory of behavior change (45% of studies) was the Theory of Planned Behavior (TPB)/Theory of Reasoned Action (TRA) (Table 1).
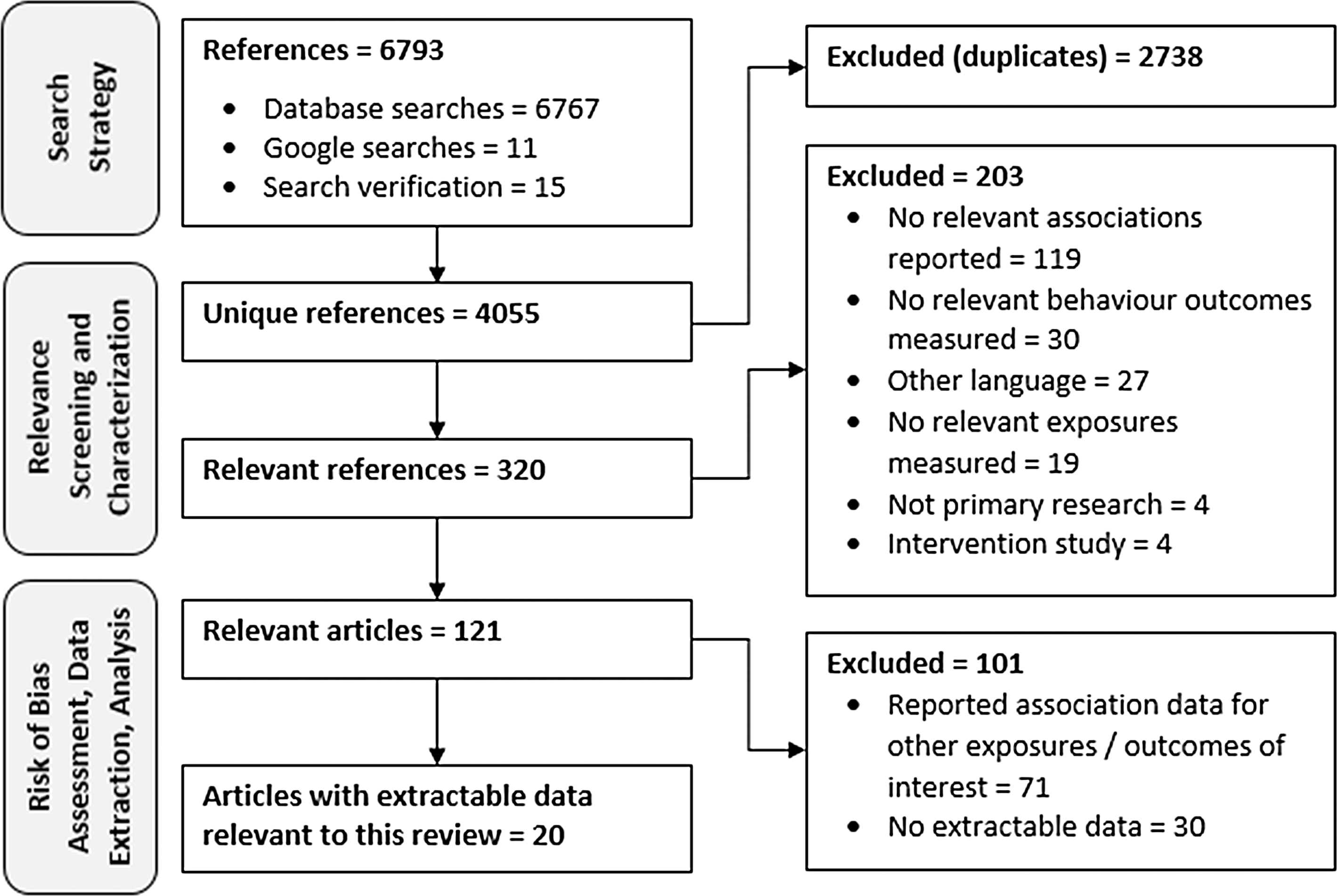
Systematic review flowchart.
All percentages were calculated out of the total number of relevant articles (n = 20).
Extracted data for these studies related to baseline measurements, before any interventions were applied.
Multiple selections were possible for these questions, so percentages may not add to 100%.
Only includes constructs that were evaluated in one or more modeling outcomes.
HAPA, Health Action Process Approach; HBM, Health Belief Model; PMT, Protection Motivation Theory; SEM; structural equation modeling; TPB, Theory of Planned Behavior; TRA, Theory of Reasoned Action.
Most studies focused on young adults (65%), evaluated overall or composite safe food handling scores (60%), and assessed one or more behavioral outcomes, including self-reported behavior (75%) and behavioral intentions (65%). More authors evaluated the impact of behavior-change theories using multivariable linear regression (65%) compared to SEM (35%) (Table 1).
A summary of the risk of bias for the relevant studies is shown in Table 2. The outcomes of many studies (65%) were rated at high risk of bias overall, largely due to a lack of control for confounding variables (Table 2). Other criteria frequently rated as unclear risk of bias included representativeness and comparability of groups of participants in the study and use of valid and reliable measurement instruments (Table 2). A summary of the characteristics and risk-of-bias ratings for each individual study is available as Supplementary Data.
Behavior-change modeling results
A summary of eight studies that evaluated the impact of behavior-change theories on consumers' adequate cooking, avoidance of the consumption of unsafe foods, cross-contamination and hygiene, and time–temperature control behaviors is shown in Tables 3 –6, respectively, and Figure 2. Three of these studies evaluated the impact of the TPB on one or more safe food handling outcomes (Tables 3 –6 and Fig. 2), all finding a significant effect on behavioral intentions (R 2 = 0.37–0.76), while the theory explained a lower proportion of the variance in self-reported behaviors (R 2 = 0.03–0.43). Within and across behavior outcomes, there was no consistency in which specific components of the TPB were significant predictors of consumers' behavior.
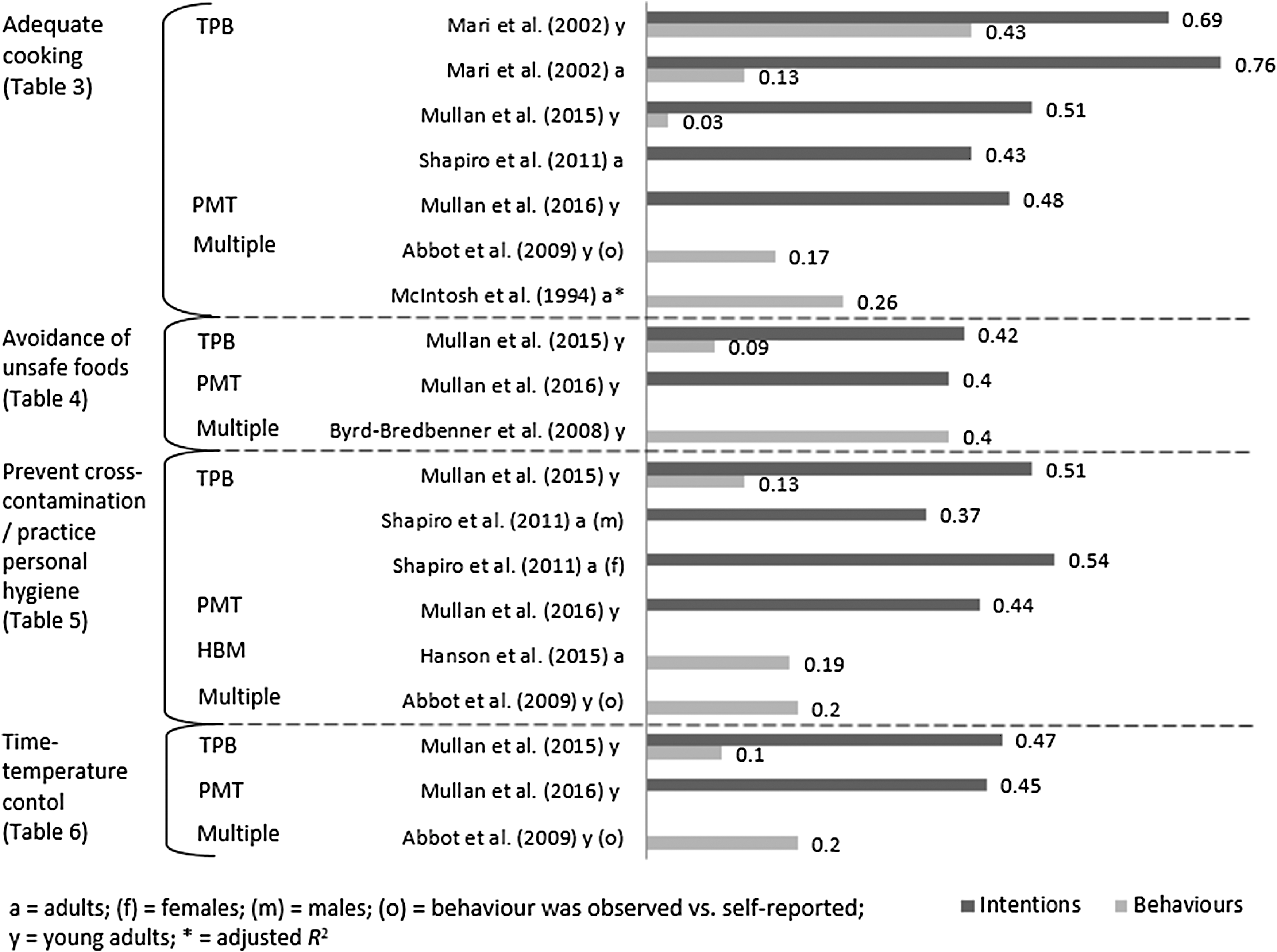
Coefficient of determination (R 2) of the best-fitting model from eight studies that measured specific safe food handling behavioral constructs, stratified by study outcome and theory evaluated. See Tables 3 –6 for additional details of each study and definitions of each theory. HBM, Health Belief Model; PMT, Protection Motivation Theory; TPB, Theory of Planned Behavior.
Outcome was observed behavior.
Outcome was self-reported behavior.
While the PBC variable was significant, the overall model was not significant.
PBC, perceived behavioral control; PMT, Protection Motivation Theory; R 2, coefficient of determination; R 2 adj, adjusted coefficient of determination (i.e., adjusted for the number of variables in the model); TPB, Theory of Planned Behavior.
Both studies measured self-reported behavior.
PBC, perceived behavioral control; PMT, Protection Motivation Theory; R 2, coefficient of determination; TPB, Theory of Planned Behavior.
Outcome was observed behavior.
Outcome was self-reported behavior.
HBM, Health Belief Model; PBC, perceived behavioral control; PMT, Protection Motivation Theory; R 2, coefficient of determination; TPB, Theory of Planned Behavior.
Outcome was observed behavior.
Outcome was self-reported behavior.
PBC, perceived behavioral control; PMT, Protection Motivation Theory; R 2, coefficient of determination; TPB, Theory of Planned Behavior.
Three studies evaluated the effect of author-specified theories consisting of multiple psychosocial constructs on one or more safe food handling outcomes (Tables 3 –6 and Fig. 2), finding that various psychosocial and sociodemographic variables were associated with the different self-reported and observed behaviors (R 2 = 0.17–0.40). One study found that the Protection Motivation Theory (PMT) significantly explained consumers' intentions to practice each safe food handling behavior construct (R 2 = 0.40–0.48), with self-efficacy the only variable that was consistently significant across each outcome (Tables 3 –6 and Fig. 2).
One study evaluated the effect of the Health Belief Model (HBM) on consumers' cross-contamination and hygiene practices (Table 5 and Fig. 2), finding that perceived severity and gender were both significant predictors (R 2 = 0.19). Seven of the eight studies evaluated the impact of confounding variables, finding that one or more confounding variables were also associated with behavioral intentions or behaviors for 10 of 14 (71%) reported outcomes (Tables 3 –6).
Thirteen studies investigated the impact of behavior-change theories on consumers' overall or composite safe food handling behavior scores (Table 7 and Fig. 3). Six TPB/TRA-based studies and two Health Action Process Approach (HAPA)-based studies measured consumers' overall behavioral intentions (Fig. 3), all finding significant effects across studies (R 2 = 0.26–0.69). Each study that measured a habit or past behavior construct found that it was a significant contributor to the model, while all five TPB-based studies found that perceived behavioral control was also significant; the effect of other constructs was inconsistent across studies (Table 7). None of the studies that measured behavioral intentions evaluated the impact of confounding variables.

Coefficient of determination (R 2) of the best-fitting model from 13 studies that measured overall safe food handling behavioral intentions and behaviors, stratified by theory evaluated. See Table 7 for additional details of each study and definitions of each theory. HAPA, Health Action Process Approach; HBM, Health Belief Model; TPB, Theory of Planned Behavior; TRA, Theory of Reasoned Action.
Outcome was observed behavior.
Outcome was self-reported behavior.
Study measured both self-reported and observed behavior outcomes.
HAPA, Health Action Process Approach; HBM, Health Belief Model; PBC, perceived behavioral control; R 2, Coefficient of determination; TPB, Theory of Planned Behavior; TRA, Theory of Reasoned Action.
Eleven studies measured overall self-reported or observed behavior outcomes (Table 7 and Fig. 3). Three of these studies evaluated the TPB, finding that it significantly explained consumers' overall self-reported and observed behaviors (R 2 = 0.32–0.42), while one study found that the TRA significantly explained consumers' self-reported behaviors but not their observed behaviors (Table 7 and Fig. 3). Studies evaluating the HAPA (n = 2) and multiple psychosocial constructs (n = 3) all found significant effects across studies (R 2 = 0.17–0.80), while two HBM-based studies showed conflicting results (Table 7 and Fig. 3).
All five studies that evaluated a habit or past behavior construct and both studies that evaluated knowledge found that these variables were significant predictors of consumers' overall safe food handling behavior in the best-fitting model, while other theory-based constructs had inconsistent effects across studies (Table 7). Two of the three studies that evaluated confounding variables found that multiple sociodemographic factors were associated with consumers' overall safe food handling behavior (Table 7).
Discussion
This review used a structured and transparent approach to synthesize studies that evaluated the ability of various behavior-change theories to explain consumers' safe food handling behaviors at home. Most studies were conducted in Australia and the United States, with all of the Australian studies coming from the same research group, indicating a lack of globally representative research in this area from different groups of investigators.
In addition, most studies focused on young adults (e.g., university and college students) and none targeted population groups at higher risk of foodborne illness and its severe consequences, such as the elderly, immunocompromised, and pregnant women (Lund and O'Brien, 2011). Previous research suggests that high-risk groups of consumers have unique barriers and facilitators toward safe food handling (Athearn et al., 2004; Cates et al., 2006; Medeiros et al., 2008; Chen et al., 2010; Dickinson et al., 2014), and behavior-change models developed for general populations of young adults and adults may not be applicable to these groups of consumers. Future research is needed to explore behavior-change theories among high-risk groups of consumers to facilitate development of appropriate and targeted theory-based interventions for these populations.
While many studies reported using formative research (e.g., previous research and surveys) to develop their data collection instruments, only 35% reported pretesting their questionnaires. Pretesting is important in theory-based studies to ensure that questions are clear, understandable, valid, and reliable (Glanz et al., 2015). A lack of reporting of these criteria contributed to unclear risk of bias ratings for several studies (Table 2).
The majority of study outcomes, however, received a high risk of bias rating due to a lack of control for confounding variables, which could have an influence on the observed relationships in those studies. Sociodemographic variables such as gender, age, ethnicity, education level, and income level are known to be associated with consumer safe food handling behaviors (Patil et al., 2005; Fein et al., 2011; Nesbitt et al., 2014) and should be evaluated for their potential influence on the relationship between behavior-change theory variables and consumer safe food handling behaviors.
This is further supported by several studies captured in this review that found that various sociodemographic variables were significant contributors to different models (Schafer et al., 1993; McIntosh et al., 1994; Byrd-Bredbenner et al., 2008; Fischer and Frewer, 2008; Abbot et al., 2009; Shapiro et al., 2011; Hanson et al., 2015; Mullan et al., 2016). While many studies controlled for the effects of age by sampling a young adult population with a very narrow age range, these were still rated as high risk of bias if other confounders deemed to be potentially important in the particular setting (e.g., gender) were not evaluated.
A recent scoping review identified 82 different theories that could have applications in behavior-change research for health-related behaviors (Davis et al., 2015). However, in this review only four different labeled theories of behavior change were identified among studies investigating consumer safe food handling behaviors (Table 1). The most commonly investigated theory was the TPB, including its precursor the TRA.
The TRA suggests that an individuals' behavior is mediated by their intention to perform that behavior, and their intention is influenced by their attitude toward the behavior and their subjective norm (i.e., perception of social pressure to perform the behavior) (Ajzen, 1991). The TPB is an extension of the TRA that includes a construct called perceived behavioral control as an additional determinant of behavioral intention and behavior (Ajzen, 1991). Perceived behavioral control refers to the extent that an individual feels in control of and is confident to perform the behavior (Ajzen, 1991).
Most TPB/TRA-based studies significantly explained consumer safe food handling behavioral intentions and behaviors to various degrees, but there was a lack of consistency in which specific constructs of the theory were significant contributors to the models (Mullan, 1997; Mullan and Wong, 2009, 2010; Fulham and Mullan, 2011; Shapiro et al., 2011; Mari et al., 2012; Milton and Mullan, 2012; Bai et al., 2014; Mullan et al., 2015).
Three studies evaluated the impact of the HBM to explain consumers' safe food handling behavior (Schafer et al., 1993; McArthur et al., 2006; Hanson et al., 2015). The HBM was one of the first theories of health behavior, originally developed in the 1950s (Glanz et al., 2015). It proposes that an individual's readiness to take a health-related action is influenced by their perceived risks (i.e., severity and susceptibility of illness), perceived barriers and benefits of engaging in the behavior, cues to action (i.e., external prompts and reminders), and self-efficacy (i.e., confidence in ability to take action) (Glanz et al., 2015).
Two of the HBM-based studies conducted with adult consumers found that at least one of the components of the theory was a significant predictor of their safe food handling behaviors (Schafer et al., 1993; Hanson et al., 2015), while the other study found that the theory did not successfully explain safe food handling behaviors among young adults (McArthur et al., 2006).
Two studies investigated the ability of the HAPA to explain consumers' safe food handling behaviors (Chow and Mullan, 2010; Mullan et al., 2010). The HAPA suggests that the adoption, initiation, and maintenance of health behaviors consist of two distinct phases: (1) preintentional motivation processes that lead to behavioral intention; and (2) postintentional decision processes that lead to the actual behavior (Schwarzer, 2008). The first (motivation) phase consists of risk perceptions, outcome expectancies (i.e., positives and negatives of implementing the behavior), and action self-efficacy (i.e., confidence in ability to implement the behavior) as predictors of behavioral intentions, while the second (volition) phase consists of behavioral planning (i.e., having goals and plans to implement the behavior), maintenance self-efficacy (i.e., confidence in maintaining a difficult behavior), and recovery self-efficacy (i.e., confidence in resuming a difficult behavior after a relapse) (Schwarzer, 2008).
Both studies found that the HAPA effectively explained consumers' overall safe food handling behavioral intentions and behaviors, but there was variability in which components of the theory were significant predictors (Chow and Mullan, 2010; Mullan et al., 2010).
One study evaluated the PMT (Mullan et al., 2016). The PMT is organized around two distinct processes: (1) the threat-appraisal process; and (2) the coping-appraisal process, both of which predict “protection motivation” (i.e., intention to perform the behavior) (Floyd et al., 2000). The threat-appraisal process consists of an evaluation of intrinsic and extrinsic rewards and perceived threat (severity and vulnerability), while the coping-appraisal process consists of an evaluation of self-efficacy, response efficacy (i.e., belief that the behavior will be effective), and response costs (e.g., monetary, time, and effort) (Floyd et al., 2000).
Mullan et al. (2016) found that the PMT effectively explained consumers' behavioral intentions across four different outcome constructs: adequate cooking; avoidance of the consumption of unsafe foods; cross-contamination and hygiene; and time–temperature control. Self-efficacy was the only construct that was consistently significant across each behavior outcome (Mullan et al., 2016).
Five studies evaluated the ability of author-developed models consisting of multiple psychosocial constructs to explain consumer safe food handling behaviors (McIntosh et al., 1994; Byrd-Bredbenner et al., 2008; Fischer and Frewer, 2008; Abbot et al., 2009; Lim et al., 2016). These studies found that a variety of different constructs were effective to explain different consumer behaviors, including knowledge, attitudes and risk perceptions, self-efficacy, locus of control, taste and health/safety preferences, and sources of food safety information (McIntosh et al., 1994; Byrd-Bredbenner et al., 2008; Fischer and Frewer, 2008; Abbot et al., 2009; Lim et al., 2016).
Although each of the identified theories of behavior change in this review was found to significantly explain consumers' safe food handling behaviors in different situations, the percentage of the variance in outcomes explained by each theory varied widely across studies. This observed heterogeneity in variance is likely influenced by the specific context of each study (e.g., consumer population, setting, and types of behaviors assessed) and other study-specific factors (e.g., how the theory and constructs were defined and measured, modeling approach used, and the impact of confounding or other potential biases).
Across all studies, whenever a measure of consumer habit or past behavior was evaluated as a predictor of behavioral intentions or behavior, it nearly always contributed significantly to the final model. Previous qualitative research has found that consumers' safe food handling behavior can be viewed as unconscious, repetitive, routine, and influenced by past actions and experiences (Young and Waddell, 2016), and a complementary systematic review and meta-analysis of the literature found a strong and consistent association between consumer habits and their safe food handling behaviors (Young et al., 2017).
Measures of self-confidence and control (e.g., self-efficacy, perceived behavioral control, and locus of control) were also frequently identified as significant predictors of consumer behavioral intentions and behaviors in this review. This construct was also found to have a strong and consistent association with consumer safe food handling behavior in a complementary systematic review and meta-analysis (Young et al., 2017). Thus, both constructs appear to be important to account for in future research in this area and when developing interventions for consumers.
Any of the theories identified in this review could be potentially adapted for use as a foundational or framework theory in the design or development of a behavior-change intervention for consumer safe food handling. However, whatever theory is selected should be appropriately modified, adapted, and refined to the specific setting by adding additional psychosocial constructs that are expected or known to be important variables in the target population. Such constructs can be identified by conducting formative research, such as qualitative focus groups or interviews with the target population, to understand consumers' underlying beliefs, experiences, barriers, and facilitators toward safe food handling (Glanz et al., 2015).
In addition, researchers could consider adapting and applying integrated behavior models that have collated relevant psychosocial constructs from multiple theories of behavior change. For example, the Theoretical Domains Framework (TDF) is one such model, designed to be applied across multidisciplinary behavior-change contexts, that includes 84 unique psychosocial constructs integrated across 14 theoretical domains (Cane et al., 2012). Another example is the Behavior Change Wheel (BCW), which models behavior change as a function of three essential components (capability, opportunity, and motivation) that are linked with nine intervention functions and seven policy categories that could enable those interventions to occur (Michie et al., 2011).
The TDF and the BCW can be used together to identify underlying psychosocial and other factors necessary to enable and facilitate behavior change (Cane et al., 2012). The BCW has been applied within the context of healthy eating and physical activity behaviors (Robinson et al., 2013; Webb et al., 2016) and could be applicable to the area of consumer safe food handling.
This review has some possible limitations. For example, although a comprehensive search strategy was implemented, it is possible that some relevant articles might not have been captured by the search algorithm or verification strategy. Articles in languages other than English, French, Spanish, and Italian were excluded, which could have underrepresented some geographic regions; however, the impact of this bias is likely minimal as all identified relevant articles were published in English.
The analysis focused on the overall impact of each behavior-change theory by considering the R 2 value (coefficient of determination) and the variables contributing significantly to the best-fitting model in each study. A statistical meta-analysis was not conducted on the reported regression model outcomes, as the data collection and analysis approaches (e.g., types of constructs measured, how constructs and outcomes were defined and measured, modeling approach, and number and type of variables included in the models) and other study characteristics differed considerably across studies. For these reasons, a descriptive tabulation and summary of the models were deemed more appropriate.
Conclusions
The TPB was identified as the most commonly investigated theory within the context of consumer safe food handling, and its constructs were generally associated with different safe food handling behavioral intentions and behaviors. Other theories and models were also found to be associated with consumers' behavioral intentions and behaviors across studies and settings, but the percentage of variance explained by each theory varied widely. Measures of consumer habit and self-confidence and control frequently contributed significantly to the various behavior-change models.
The results of this review suggest that multiple theories and psychosocial constructs can contribute to explaining consumer safe food handling behaviors, and these could help to guide the development of behavior-change interventions for consumers. Future studies and applications in this area should carefully review, select, and adapt an appropriate behavior-change theory to match the needs of the specific context and local situation, which might include adding psychosocial constructs determined to be important through formative research with the target population, as well as considering the adoption of integrated behavior theories and models.
Footnotes
Acknowledgments
The authors thank Cecile Farnum for assistance in developing the search strategy and Janet Harris and the Ryerson University Interlibrary Loan staff for assistance procuring relevant articles. This research was supported by funding from an SRC Seed Grant, Faculty of Community Services, Ryerson University. The National Microbiology Laboratory, Public Health Agency of Canada, is also acknowledged for providing in-kind support.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.