
Abstract
Background:
Rates of Campylobacter infection in Arizona have historically been higher than the national average, with the highest rates in Hispanic populations. The purpose of this retrospective case–case analysis was to determine how risk factors and disease presentation differ by ethnicity (Hispanic vs. Non-Hispanic) in cases of campylobacteriosis from 2012 to 2015 in Maricopa County, Arizona.
Methods:
Basic demographics and seasonality, including standardized morbidity ratios (SMRs), were analyzed to determine differences by ethnicity. To determine differences in risk factors, adjusted univariate and multivariable logistic regression was conducted.
Results:
There were significant differences by ethnicity by age (1–14 years and >60 years), location of residence (urban vs. suburban), and testing methodology. Most months in the seasonality analysis showed higher than expected values of Hispanic cases based on population distributions (SMR Range: 0.91–1.78, annual mean: 1.23). Differences in disease presentation showed that Hispanics (adjusted for age and location of residence) were more likely to experience vomiting (OR = 1.41) and fever (OR = 1.08), as well as seek care through an urgent care or emergency department (OR = 1.50), than non-Hispanic cases. Hispanics had a higher odds of reporting consumption of tomatoes (OR = 1.45), salsa (OR = 2.35), cilantro (OR = 2.21), queso fresco (OR = 8.53), and sprouts (OR = 1.94) than non-Hispanic cases. Multivariable analyses found queso fresco (aOR = 6.58), cilantro (aOR = 3.93), and animal products (aOR = 0.38) all to be significant by ethnicity.
Conclusions:
Hispanics had a higher likelihood of consuming high risk foods, while non-Hispanics were more likely to have environmental exposures linked to Campylobacter infection. Focused questionnaires can reveal differences and contribute to improving public health action/education for specific populations.
Introduction
C
Differences in ethnicity among Campylobacter cases have been reviewed in European countries where higher rates were reported among people of non-European decent (Gillespie 2003a; Manaseki et al., 2004; Gillespie et al., 2008). Arizona, where the population of Hispanics is 30% (US Census Bureau, 2016) and the rates of campylobacteriosis are routinely higher than the national average (14.1 compared to 13.3 per 100,000 in 2014), was well suited to examine risk factor differences in cases by ethnicity (ADHS, 2015; CDC, 2016b). A 2010 statewide case–control study found that cases were six times more likely to be Hispanic compared to NH. Surprisingly, while the odds of travel, particularly to Mexico, was strongly associated with disease onset, it did not account for the differences in ethnicity (OR = 7.27 for Hispanic nontravelers and OR = 5.87 for Hispanic travelers) (Pogreba-Brown, 2016). Very few studies have been conducted to identify the specific causes of these differences. Some theories are related to cultural differences in kitchen practices, such as washing raw poultry (Henley et al., 2012).
While national rates have been declining since 2011, rates in Arizona increased over the same period. Maricopa County, Arizona, a mix of urban, suburban, and rural areas, has over four million residents with disease rates similar to those seen statewide. Due to the increasing popularity and emergence of culture-independent diagnostic tests (CIDTs) as a method for the detection of Campylobacter in stool, reporting requirements and case definitions were changed in 2015 to include illnesses with positive CIDTs as probable cases (CDC, 2015). This change has led to marked increases in the reported rates of disease (the statewide rate increased from 14.1 to 20.4 per 100,000 from 2014 to 2015).
The goal of this case–case analysis was to compare Hispanic Campylobacter cases to NH Campylobacter cases to determine whether disease outcomes and common risk factors differ by ethnicity. The objectives of this work were to determine (1) differences in disease presentation and healthcare utilization between these two groups and (2) which high risk exposures were more commonly reported by ethnic group.
Materials and Methods
Campylobacter infections are required to be reported electronically to public health agencies within 5 days of laboratory confirmation (Arizona Administrative Code, 2013). The Maricopa County Department of Public Health (MCDPH) utilizes the University of Arizona's Student Aid for Field Epidemiology Response Team to conduct surveillance for all cases of Campylobacter. The Campylobacter questionnaire addresses demographics, symptomatology, travel history, food consumption (with an emphasis on high-risk foods), and a variety of water and animal exposures in the week before illness onset.
From 2012 to 2015, cases reported through public health surveillance were interviewed by phone for those cases that were (1) culture confirmed (years 2012–2015), (2) positive through nonculture based methods (probable) (2015 only), (3) had a valid contact number reported, and (4) spoke English or Spanish. Cases were contacted a minimum of three times during evenings, weekdays, and weekends before being lost to follow-up. While data on cases that were not interviewed were limited to age and gender, a comparison between interviewed and noninterviewed cases was conducted to determine if any basic differences existed between these two groups and determine the potential impact of selection bias (SAS Software 9.4). No additional analyses of risk factors were done on noninterviewed cases, and these cases were not used in any regression models.
For all interviewed cases, frequencies of demographics, symptoms, and healthcare utilization were calculated for the total sample and stratified by ethnicity. Information on cases that chose not to answer the ethnicity question were included to report other demographic information on all interviewed cases, but were excluded from further risk factor analyses. A sensitivity analysis was also conducted to check for the effects of specific outliers in the data for number of days with diarrhea (two patients with 330 and 365 days, respectively) and number of days hospitalized (three patients with 359, 361, and 726 days, respectively).
Cases were graphed by ethnicity and month to determine any seasonal differences. An indirect adjustment was calculated based on the reported Hispanic population within the county (30%) (US Census Bureau, 2016). A standardized morbidity ratio (SMR) was calculated to determine the proportion of cases above the expected values given the distribution of the population (as determined by values greater than SMR = 1.0).
As part of the model building process, variables were divided into three classes, demographics, disease presentation, and exposures. Demographic variables (class 1) that were significant at the p = 0.20 level using Chi-squared were included as possible confounders in subsequent models. Adjusted models were created for each factor in both class 2 (symptoms, duration, and healthcare utilization) and class 3 (exposure) variables. Both class 2 and class 3 models were adjusted for age and suburban residence, both known risk factors, and the only class 1 variables that remained significant in subsequent models. Univariate analyses used to check these variables resulted in a greater than 10% change to the measure of association. A final multivariable model was built based on significant class 2 and 3 variables. Using backward elimination, variables were included in the model if they were significant at the p = 0.05 level using the likelihood ratio test and Wald statistic. An interaction term between laboratory confirmation method (CIDT vs. culture) and age showed that the testing method was an effect modifier. Gender was also tested as an effect modifier. Individual adjusted models for exposures were stratified by testing method (STATA software 13.0). Odds ratios above 1.0 represent an increased association for Hispanics compared to NHs.
Results
From 2012 to 2015, a total of 2848 cases were reported to MCDPH with 1987 cases eligible for interview. A total of 1213 interviews were successfully completed (overall response rate 61.0%) (SAS software 9.4). The level of missing data for all variables ranged from 0% to 35% with an average of 5%; some of this was due to additions to the questionnaire following some large outbreaks. Analyses of noninterviewed cases found that 54% were male and the median age was 25 years. These values were not significantly different from the demographics of interviewed cases. Reported case rates for all campylobacteriosis cases were similar for Maricopa County and the state of Arizona as a whole. The sharp increase in 2015 data accounted for the inclusion of probable CIDT cases that had not previously been included in surveillance reporting (Table 1).
U.S. Census Population Estimate for Maricopa County, Arizona. Accessed 22 September 2016.
Total includes all races and those of unknown race/ethnicity.
Statewide rates for Arizona, Arizona Department of Health Services. Accessed 22 September 2016.
http://www.azdhs.gov/preparedness/epidemiology-disease-control/index.php#data-stats-archive
Demographics and symptoms of interviewed cases stratified by ethnicity are reported in Tables 2 and 3, respectively. Hispanics had higher case counts in children and adolescents (mean age = 20.5), whereas the majority of cases among NHs were seen among adults (mean age = 41.8). Significant differences by ethnicity were found in three age categories (1–4, 5–15, and ≥60 years old). Differences in ethnicity were also found for confirmation method and residence where Hispanic cases predominately lived in urban areas, and the majority of NH cases lived in suburban areas. Results of the sensitivity analysis found no differences when patients with outlying values for number of days with diarrhea and number of days hospitalized were excluded from the analyses. All patient data were retained for the regression models.
The Other category represents 34 Mexican American, 27 Hispanic/Latino, 26 of mixed race, 14 with various nationalities, and 48 cases with missing information on their specific race. All 27 cases who indicated Hispanic/Latino for their race also indicated that they were Hispanic for their ethnicity.
Location of residence descriptions: Urban (city), Suburban (residential area), Town (urban area that is larger than a village and smaller than a city), Rural (a countryside area rather than the town), and Farm (an area of land and its buildings used for growing crops and rearing animals).
Bold variables indicate a statistically significant difference at the 95% confidence level between Hispanic and non-Hispanic cases.
Adjusted for age and suburban location of residence.
Bold variables indicate a statistically significant difference at the 95% confidence level.
Generally, case counts of campylobacteriosis peak in the summer months. While the highest total case counts were seen in the summer months, following a brief drop in September, counts increased again through the fall and into December (Fig. 1). The SMR showed statistically significant peaks in April, May, and August for Hispanic populations in the county. Overall, the SMR ranged from 0.91 to 1.78 with a mean of 1.23 with most months showing observed rates among Hispanics to be above expected values based on population distributions (SMR >1.0).
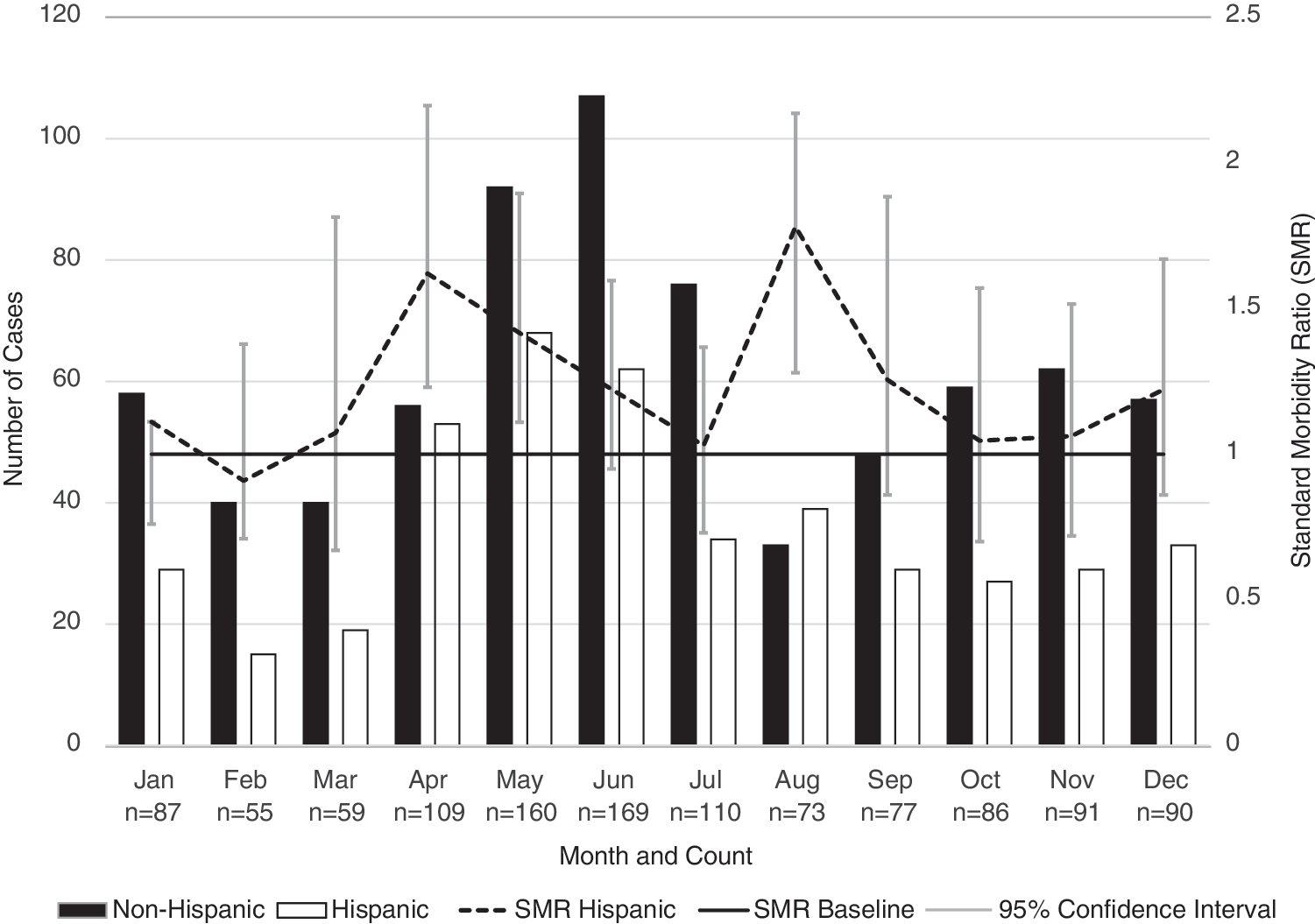
Frequency of Campylobacter Cases by Month from 2012 to 2015 with Standardized Morbidity Ratio (SMR) of Hispanic cases with 95% Confidence intervals.
Among class 1 variables, age and residing in a suburban area were statistically associated with cases (p < 0.001) and, therefore, were controlled as potential confounders in further models. All disease presentation (class 2) models showed that Hispanics reported vomiting as a symptom 41% more often than NH (OR = 1.41) and fever slightly more often (OR = 1.08). Regarding healthcare utilization, Hispanics presented at an Emergency Department or Urgent Care 50% more often (OR = 1.50) and conversely, NH were 42% more likely to see a primary care physician (OR = 0.58). All significant class 2 variables reported in Table 3 were added to the multivariable model. None remained in the model following backward elimination.
Of the 40 exposure variables tested using logistic regression (adjusted for age and suburban residence), 6 were reported more frequently by Hispanic cases than non-Hispanic cases (Table 4). Hispanics were over twice as likely to report eating cilantro (OR = 2.14) and over eight times as likely to report consuming queso fresco (OR = 8.29) than NH. Other exposures with a higher odds in Hispanics were salsa (OR = 2.35), tomatoes (OR = 1.45), sprouts (OR = 1.94), as well as eating from a cafeteria (OR = 1.87). For other exposures, NH were 46% more likely to report contact with animal products (food, pet treats, feces, manure, and hides) (OR = 0.54) and had a 31% higher odds of having contact with a river, lake, or stream (OR = 0.69) compared to Hispanics. Poultry, a commonly reported risk factor for campylobacteriosis, showed no differences in consumption patterns by Hispanics or NH. There were no statistically significant differences by ethnicity on reported occupation or travel.
Adjusted for age and suburban location of residence.
Bold variables indicate a statistically significant difference at the 95% confidence level.
For the final multivariable model (Table 5), Hispanics were significantly more likely to consume cilantro (OR = 3.93) and queso fresco (OR = 6.58) and significantly less likely to have exposure to animal products (OR = 0.38) than NH.
Adjusting for all other variables in the model.
Bold variables indicate a statistically significant difference at the 95% confidence level.
During the initial analyses it was determined that there were significant differences between cases identified through culture and CIDT related to age (p < 0.05) and ethnicity (p < 0.05). CIDT cases were disproportionately Hispanic and younger. For all demographic variables, there was no other evidence of effect modification based on stratified analysis or interaction terms using a likelihood ratio test. For exposures, most of the stratified results did not differ from the combined dataset. Two exceptions were found for consumption of poultry and eggs, where the odds ratios differed dramatically by test type. For CIDT cases, the odds of consuming eggs was thrice higher for Hispanics than NH and four times higher for consuming poultry, whereas there was no association for cases identified through the culture test.
Discussion
This study detected a marked difference in exposures associated with campylobacteriosis among Hispanics compared to NH within the most populous county of the southwestern part of the United States. Surveillance data are often underutilized; however, using an enhanced survey within routine systems already in place, we were able to collect additional information not normally captured. This information can be used to develop targeted messaging or outreach to specific populations.
The main notable difference in cases by ethnicity was age. Hispanic cases were predominately under the age of 14, while NH cases were largely over 40 years of age. While higher rates among children under the age of five, and persons with Hispanic ethnicity are reported nationally (Friedman et al., 2004; CDC, 2014) and internationally (Skirrow, 1987; Green, 2006; European Centre for Disease Prevention and Control, 2011), the differences by age and ethnicity together have rarely been explored in the literature up to this point. Determining whether this is an artifact seen only in areas with a high Hispanic population or whether it is more widespread would help to target interventions for specific at-risk groups. The challenge may be due to ethnicity data itself. As we showed in Table 1 where the overall rate is much higher than each ethnicity rate, this demographic information is often missing in routine surveillance data. Our group made a concerted effort to determine the ethnicity for each case interviewed (only 42 cases were dropped from the original dataset due to missing ethnicity data), but it is often a question people choose not to answer.
To demonstrate the differences in seasonality by ethnicity we chose to use an SMR. A stable population of 30% Hispanic over the four years of data collection was used. This is a limitation given possible shifts in population over time, but according to census data, the population was estimated to have changed by less than one percent from 2010 to 2015 (U.S. Census Bureau, 2016), although the exact percentage is unknown. However, this representation made it very clear what times of the year Hispanics may be at higher risk of infection. While cases among NH seem to peak in the typical summer months (May-July), a trend noted in other studies (Blaser, 1997; Friedman et al., 2004; Nichols et al., 2012), cases among Hispanics seem to have an earlier and longer period of time in which infections were reported starting with a peak in April, high numbers of cases in the summer (but not higher in relation to NH), and followed with another peak in August. Our team speculated that the high number of cases in April may have been due to the holiday La Semana Santa (Holy Week) that precedes Easter. This typically includes a high influx of travelers at the Mexico/U.S. border and a tradition of cascarones, an egg which is hollowed out, filled with confetti, and cracked on someone's head as a surprise. Interestingly, case numbers among NH increase again in October through January, possibly due to a large influx of retired winter visitors to the county.
The odds of consumption of higher risk foods among Hispanics were higher than the odds in NH. The authors acknowledge that this is in some way simply a reflection of differences in dietary preferences by different cultural groups. However, it is important to take into account that all of these foods were part of the survey because they have at one time (or several times) been linked to foodborne pathogens. For example, while queso fresco was much more often consumed by Hispanics (CDC, 2016b), raw dairy has been a commonly reported risk factor for campylobacteriosis around the world (Eberhart-Phillips et al., 1997; Friedman et al., 2004; Domingues et al., 2012). There were also some unexpected results such as a higher odds ratio seen with consumption of sprouts by Hispanics. For NH, only handling animal products was significant in the individual risk factor or multivariable models. This highlights the potential importance of targeted intervention or education campaigns based on ethnicity. It is also clear that some common exposures like poultry consumption are evenly distributed across both ethnic groups.
One interesting subanalysis was the stratification of cases by laboratory method. Stratification may become increasingly important as more CIDT cases are included in surveillance data across the country. At this time, the cause of these differences is unclear, but this observation has been made in other jurisdictions as well (Long, 2015). In this study, CIDT was more common with children and often reported from two large hospitals in the Phoenix Metro area. The differences may be more of a result of the populations served by those hospitals, but it should be noted that they serve very different population demographics. One interesting result from the stratification was the results seen with poultry and eggs. Neither of these foods was statistically different by ethnicity, but when they were stratified by test type, the odds ratios were significantly higher for CIDT cases compared to culture confirmed cases. The authors theorize that this may have been due to a missed cluster of cases that happened to be served by the two hospitals that primarily use CIDT methods. We intend to continue investigating these differences to see if they hold true over time or if the observation was simply an anomaly in this dataset.
Regarding disease presentation, Hispanics were found to have a higher odds for vomiting and fever, even when adjusted by age and suburban residence. However, while statistically significant, this may not have any biologic importance and would need to be investigated in a larger study. Regarding healthcare utilization, Hispanics had a higher odds of visiting an urgent care or emergency department, while NH were much more likely to seek medical attention elsewhere (primary care physician). The number of adult Hispanic citizens that have a usual healthcare provider in the United States (76%) is consistently lower than the U.S. population (83%) with the main barrier being financial reasons, such as the high cost of medical care and no health insurance (Livingston, 2009). These healthcare inequalities must be addressed to improve the health of the Hispanic population in the United States. These results again may allow for targeted interventions such as education campaigns based on where patients are most likely to seek care.
The size of the population, as well as the high proportion of Hispanics, added to the strength of this study. There were limitations to our study, including possible differences between those who did not respond to our interview attempts compared to those who did, but in comparing the information we had on noninterviewed cases, there were no significant differences. Conducting a case–case analysis is a less resource intensive way to determine risk exposures across groups (e.g., across different ethnicities), and because people who go through the process of reporting a disease may be more alike to each other than non-ill controls, selection bias is reduced (McCarthy and Giesecke, 1999). In addition, case–case studies can reduce recall bias compared to traditional case–control methods (Pogreba-Brown et al., 2014). This study utilized routine Campylobacter cases to determine differences in disease presentation and potential risk factors between Hispanics and NH. While case–case methods are often utilized between two different diseases (for example, Campylobacter compared to Salmonella or outbreak cases verses routine cases), several studies have used this methodology to explore differences in risk factor profiles among cases of the same disease. These differences have included ethnicity and race (Jones et al., 2008; Peterson et al., 2011), severity of disease (Bai et al., 2004), urban verses rural (Levesque et al., 2013), seasonality (Ravel et al., 2010), time to diagnosis (Bonjour et al., 2008), and even the existence of undetected clusters (Gillespie et al., 2003b). Finally, using this method, logistic regression models can be built and expressed as odds ratios, allowing for the direction and magnitude of the association to be determined, rather than just discerning that a difference exists (as expressed by a χ2 value).
Conclusions
Differences in presentation of disease may be related to specific exposures, dose, genetics, or other unidentified factors. We recommend that further analysis by race and ethnicity be conducted on a broader scale, both over longer periods of time or a larger geography, to determine why these differences exist, and not just that they do. Finally, additional studies should be conducted to determine if and why differences in risk factor by detection method are seen more broadly.
Footnotes
Acknowledgments
The authors thank the student team interviewers who helped to collect these data and epidemiologists, particularly Nicole Fowle at Maricopa County Department of Public Health, for their assistance and support.
Disclaimers
The views expressed in the submitted article are the authors own and not an official position of the institution or funder.
Disclosure Statement
The authors declare no conflicts of interest.