
Abstract
Background:
Salmonella is a leading cause of foodborne enterocolitis worldwide. Antimicrobial use in food animals is the driving force for antimicrobial resistance among Salmonella particularly in high-income countries. Nontyphoidal Salmonella (NTS) infections that are multidrug resistant (MDR) (nonsusceptible to ≥1 agent in ≥3 antimicrobial categories) may result in more severe health outcomes, although these effects have not been systematically examined. We conducted a systematic review and meta-analysis to examine impacts of MDR NTS on disease outcomes in high-income settings.
Methods:
We systematically reviewed the literature from scientific databases, including PubMed, Scopus, and grey literature sources, using preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines. We included peer-reviewed publications of case-control and cohort studies, outbreak investigations, and published theses, imposing no language restriction. We included publications from January 1, 1990 through September 15, 2016 from high-income countries as classified by the World Bank, and extracted data on duration of illness, hospitalization, morbidity and mortality of MDR, and pan-susceptible NTS infections.
Results:
After removing duplicates, the initial search revealed 4258 articles. After further screening, 16 eligible studies were identified for the systematic review, but, only 9 of these were included in the meta-analysis. NTS serotypes differed among the reported studies, but serotypes Typhimurium, Enteritidis, Newport, and Heidelberg were the most often reported MDR pathogens. Salmonella infections that were MDR were associated with excess bloodstream infections (odds ratio [OR] 1.73; 95% confidence interval [CI] 1.32–2.27), more frequent hospitalizations (OR 2.51; 95% CI 1.38–4.58), and higher mortality (OR 3.54; 95% CI 1.10–11.40) when compared with pan-susceptible isolates.
Conclusions:
Our study suggests that MDR NTS infections have more serious health outcomes compared with pan-susceptible strains. With the emergence of MDR Salmonella strains in high-income countries, it is crucial to reduce the use of antimicrobials in animals and humans, and intervene to prevent foodborne infections.
Introduction
N
Use of antimicrobials creates a selection pressure for emergence and dissemination of antimicrobial resistance, which has been documented in NTS infections worldwide (Su et al., 2004; Majtan et al., 2010; Sparham et al., 2017). In low-income countries, where intensive animal feeding operations are uncommon, this increase has been attributed mostly to the use of antimicrobials in humans. In high-income countries, where little person-to-person Salmonella infection occurs, several studies provide evidence for a direct link between antimicrobial use in animals and the emergence of antimicrobial-resistant Salmonella infections in humans (Holmberg et al., 1984; Fey et al., 2000; Bertrand et al., 2006; Dutil et al., 2010).
With rising concerns about antimicrobial resistance globally, scientific research has largely consisted of studies documenting trends in resistance phenotypes and describing occurrence of resistance genes in relation to Salmonella serotypes. Several studies have shown that patients with Salmonella infections of certain antimicrobial resistance patterns have more severe outcomes than those which are pan-susceptible (Crump et al., 2011; Barlow, 2012; Krueger et al., 2014; Angelo et al., 2016); however, other studies have not demonstrated such association (Devasia et al., 2005). No systematic review or meta-analysis has been conducted to examine the relationship between resistance and disease outcome for salmonellosis.
We systematically reviewed the literature regarding health outcomes from infection with multidrug-resistant (MDR) and pan-susceptible Salmonella. We restricted the study to high-income settings only due to: greater availability of data, differences in healthcare delivery, underlying resources, and treatment options (Chinnock et al., 2005).
Materials and Methods
This systematic review and meta-analysis was performed using preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines (Moher et al., 2009). The review protocol is available in PROSPERO under the registration number CRD42017055712.
Search methodology
A systematic search was undertaken of (1) scientific databases, (2) grey literature, (3) public request for information, and (4) reference list search of eligible articles identified in (1) and (2). We searched six electronic scientific databases (PubMed, Scopus, Web of Science, Cochrane library, Lilacs, and Open Access Theses and Dissertations) and grey literature sources, including European Food and Safety Authority (EFSA), Food and Agriculture Organization of The United Nations (FAO), U.S. Food and Drug Administration (FDA), WHO library and website, Health Canada, and the U.S. Centers for Disease Control and Prevention (CDC) for articles published from January 1, 1990 through September 15, 2016. We complemented our search with a backward citation search of the studies included in the meta-analysis. The process of study selection for inclusion in the systematic review and meta-analysis is presented in Figure 1. Search terms were identified by (1) combining Medical Subject Headings (MeSH) for relevant and appropriate terms, and (2) key terminology from primary studies. We consulted a librarian to develop a search strategy for each database (Appendix 1 in the Supplementary Data; Supplementary Data are available online at
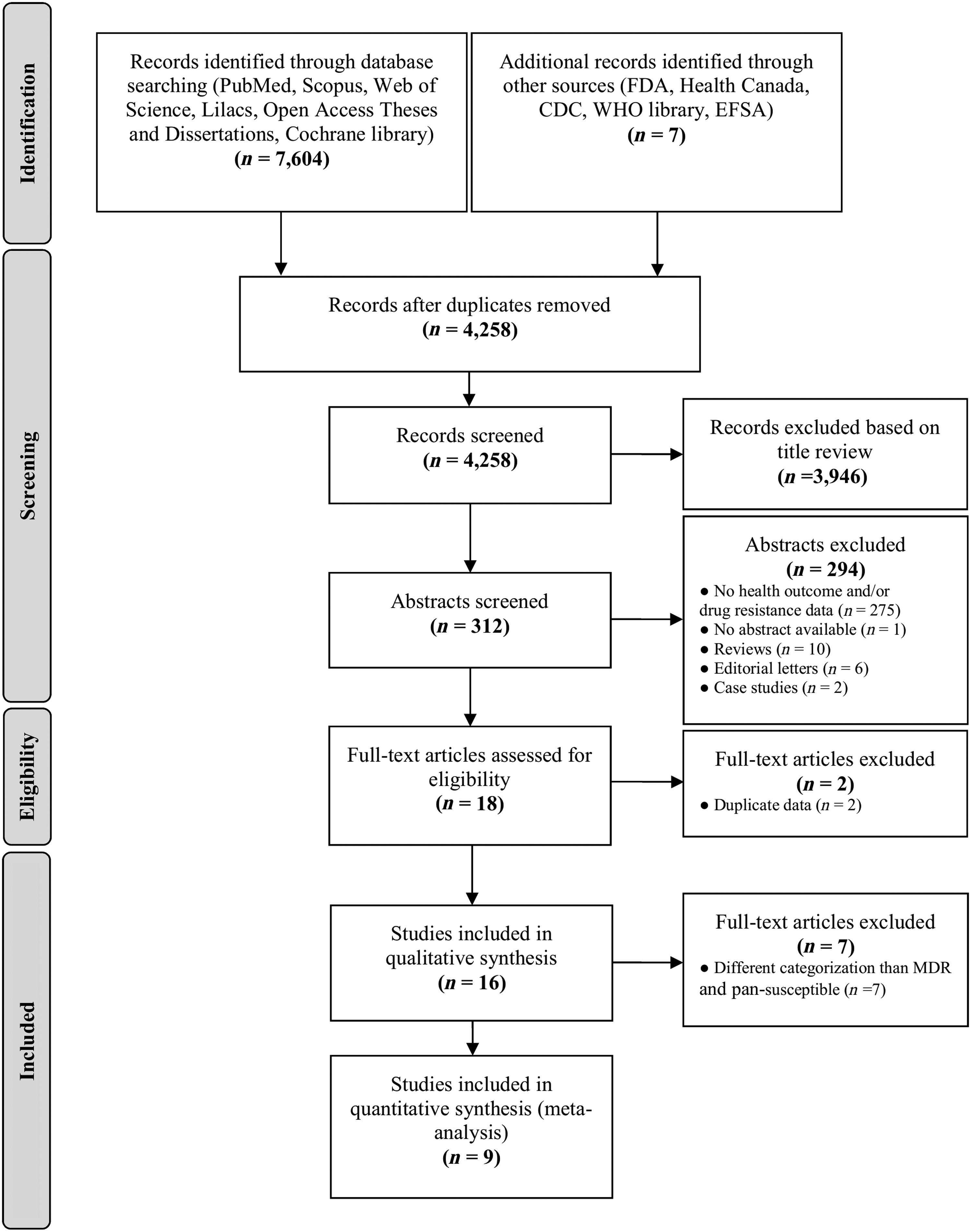
Flow diagram of studies included in the systematic review and meta-analysis examining the health outcomes of MDR and pan-susceptible NTS in high-income countries. CDC, Centers for Disease Control and Prevention; FDA, Food and Drug Administration; EFSA, European Food and Safety Authority; MDR, multidrug resistant; NTS, nontyphoidal Salmonella; WHO, World Health Organization.
Study selection
Study titles were screened independently by two authors (A.P. and S.V.), and potentially relevant studies were imported into EndNote X7. After removing duplicates, relevant titles were screened. Studies published in languages other than English, including French and Spanish, were reviewed by the researcher fluent in those languages (A.P.). After relevant abstracts were screened, full-text articles of all potentially relevant studies were located and independently assessed for eligibility against the review protocol by the same two authors (A.P. and S.V.). Any discrepancies during the selection were discussed with a third author (M.D.K.).
The systematic review was restricted to human studies reporting health outcomes from MDR and pan-susceptible NTS isolates in high-income countries. The list of exclusion and inclusion criteria for each stage of the review process is described in Appendix 2 in the Supplementary Data. To identify high-income countries, we used the World Bank classification, where high-income economies are those with a gross national income per capita of $12,476 (U.S. dollars) or more in 2015 (World Bank, 2016). As recommended by the European Center for Disease Prevention and Control (ECDC) and the CDC, multidrug resistance was defined as nonsusceptibility to at least one agent in ≥3 antimicrobial categories (Magiorakos et al., 2012). Pan-susceptible isolates were considered as those susceptible to the agents in the following categories: penicillins, phenicols, aminoglycosides, sulfonamides, tetracyclines, and quinolones. We applied no language restrictions.
Data extraction
Data from the included studies were independently extracted by one author (A.P.) and checked by another author (S.V.) using a predefined tool (Appendix 3 in the Supplementary Data). Data extracted from eligible articles included location, data source, study period, study type, Salmonella serotype, sample size, antimicrobial pattern, and health outcomes, including (1) bloodstream infection, (2) hospitalization, (3) length of hospital stay, (4) mortality, (5) intravenous fluids, (6) fever, and (7) other outcome (Appendix 4 in the Supplementary Data). Additionally, for studies included in the meta-analysis, we extracted data on age and comorbidities, including immunosuppressive conditions (Appendix 5 in the Supplementary Data). Studies excluded from the meta-analysis are presented in Appendix 6 in the Supplementary Data.
For all health outcomes, except for length of hospital stay, we extracted information on adjusted odds ratios (ORs) and 95% confidence intervals (95% CI) comparing MDR and pan-susceptible NTS infections. Where a study did not report adjusted OR with 95% CI, we calculated crude values using formula OR = (a × d)/(b × c). Concerning length of hospital stay, authors were contacted to provide additional information on the mean and standard deviation of the length of stay, if these values were not reported in the studies. Where multiple different groupings of antimicrobial resistance or patient populations were reported in the same study, data were extracted for each group separately. Because many of the included studies did not report on bloodstream infections but did report on sample origin (blood, cerebrospinal fluid [CSF], feces, urine, or other) a specific data extraction was performed. Invasive infections were defined as isolation of Salmonella from blood, CSF, or other normally sterile site. This could have resulted in biased results, and we tested this by performing a subgroup analysis. In addition, this outcome was addressed in quality assessment and the quality effect (QE) model (discussed later).
Due to the very limited number of studies reporting on health outcomes from MDR Salmonella, we also assessed studies with antimicrobial resistance patterns other than MDR in one group and pan-susceptible in the comparison group. These studies reported on quinolone resistance (Helms et al., 2004; Broughton et al., 2010), ciprofloxacin resistance (Hsu et al., 2005; Wang et al., 2006), resistance to a median of three antimicrobial agents (Lee et al., 1994), and studies where the control group was not pan-susceptible (Helms et al., 2003; Martin et al., 2004). However, due to small number of studies in each category and very different antimicrobial patterns in both groups, these studies were excluded from the quantitative synthesis (Appendix 6 in the Supplementary Data).
Quality assessment
The quality of each study included in the meta-analysis was assessed using the Newcastle–Ottawa quality assessment scale (Wells et al., 2009). The scale was modified so that it would allow for analysis of all study types with the same criteria. Modifications were also made based on the risk of bias and the type of health outcome measured. The modified scale considered seven safeguards against bias, which were combined into a univariate quality score (Qi) as outlined in Appendix 7 in the Supplementary Data. Quality assessment was performed independently by AP and SV, with disagreements resolved through discussion and consensus by MDK.
Statistical analyses
All statistical analyses described below were performed comparing MDR and pan-susceptible NTS infections. Where a study reported on several multidrug resistance patterns, the pattern “resistant to ≥3 categories” was given a priority in the meta-analysis. Where study reported on the same outcome in different patient populations, the population sample with different serotypes was given a priority. The outcome measure used for statistical analysis was the OR. For comparison purposes, we pooled data using three meta-analytical models: the inverse variance heterogeneity model (IVhet) (Doi et al., 2015a), the random effect model (RE) (DerSimonian and Laird, 1986), and the QE model (Doi et al., 2015b). The reported results are based on the IVhet, with the RE and QE outputs reported in the Supplementary Data for comparison purposes. Statistical heterogeneity was assessed using Higgin's I 2 with values of 25%, 50%, and 75% considered as low, moderate, and high, respectively (Higgins et al., 2003). To check for possible publication bias, we used Doi plots as they are more sensitive than funnel plots (Furuya-Kanamori et al., 2018), which are difficult to interpret when there are less than 10 studies. A quantitative measure of Doi plot asymmetry was done using the Luis Furuya-Kanamori (LFK) index (Furuya-Kanamori et al., 2018).
We performed sensitivity analyses for all health outcomes and one subgroup analysis for bloodstream infection. Sensitivity analysis was performed by excluding each study in turn and subsequently comparing the pooled OR with original result outcomes. The subgroup analysis was conducted by dividing studies based on whether the study directly reported the outcome as “bloodstream infection” or it was considered as bloodstream infection due to the blood origin of the isolate.
Statistical analyses were performed for all health outcome categories, except for the length of hospital stay, where missing data on the mean and standard deviation allowed only for a descriptive summary of study results. All analyses were conducted using MetaXL version 5.3 (EpiGear Int Pty Ltd.; Sunrise Beach, QLD, Australia;
Results
The initial search identified 7611 publications. After excluding duplicates, 4258 articles remained. After screening the publications by title and abstract, 16 studies were included in the final review, and 9 of these were included in the meta-analysis (Fig. 1).
All publications included in the meta-analysis are summarized in Table 1. All studies were from the United States of America, conducted between 1984 and 2013, and together covered more than 55 years of research with 77,981 participants. The most common MDR pattern was R-type ACSSuT and most common Salmonella serotypes were Typhimurium, Enteritidis, and Newport. Six studies included information on bloodstream infection, seven on hospitalization, four on median length of hospital stay, and three on mortality. Quality scores of included studies ranged from 5 to 9 (out of 9) and are summarized in Appendix 7 in the Supplementary Data.
ACSSuT: resistant to at least ampicillin, chloramphenicol, streptomycin, sulfonamide, and tetracycline.
MDR-AmpC: resistant to amoxicillin/clavulanate, ampicillin, cefoxitin, ceftiofur, cephalothin, chloramphenicol, streptomycin, sulfamethoxazole, tetracycline, and had decreased susceptibility to ceftriaxone.
MDR-AmpC: resistant to amoxicillin/clavulanate, ampicillin, cefoxitin, ceftiofur, cephalothin, streptomycin, sulfamethoxazole, but not chloramphenicol or tetracycline.
AC/KSSuT: resistant to at least ampicillin, chloramphenicol, kanamycin, streptomycin, sulfamethoxazole, and tetracycline.
CDC, Centers for Disease Control and Prevention; CI, confidence interval; MDR, multidrug resistant; NTS, nontyphoidal Salmonella; OR, odds ratio.
None of the studies reported data on comorbidities, except for the study of Krueger et al. (2014) who excluded patients with coinfection with another enteric bacterium from their analysis. Two studies reported data on underlying immunosuppressive conditions (Gupta et al., 2003; Devasia et al., 2005), but only the study of Devasia et al. (2005) compared immunosuppressed MDR-AmpC and pan-susceptible Salmonella Newport infection, and found no statistically significant difference in all three health outcomes. Furthermore, immunosuppression did not seem to convey a statistically significant increased risk for the MDR-AmpC Salmonella Newport infection (relative risk (RR), 1.5; 95% CI, 0.9–2.7). Data on age (median, age ≤5 years, age ≥65 years) and potential immunosuppressive conditions are summarized in Appendix 5 in the Supplementary Data.
The odds of bloodstream infection were significantly higher for an NTS infection by an MDR versus pan-susceptible strain (Fig. 2; OR, 1.73; 95% CI, 1.32–2.27). Similarly, MDR infections were associated with increased odds of being hospitalized (OR, 2.51; 95% CI, 1.38–4.58). A statistically significant association was also found for mortality (OR, 3.54; 95% CI, 1.10–11.40), but the analysis was based only on three studies. Concerning length of hospital stay, considering only information on median days, MDR NTS infections were associated with approximately one extra day of hospitalization.
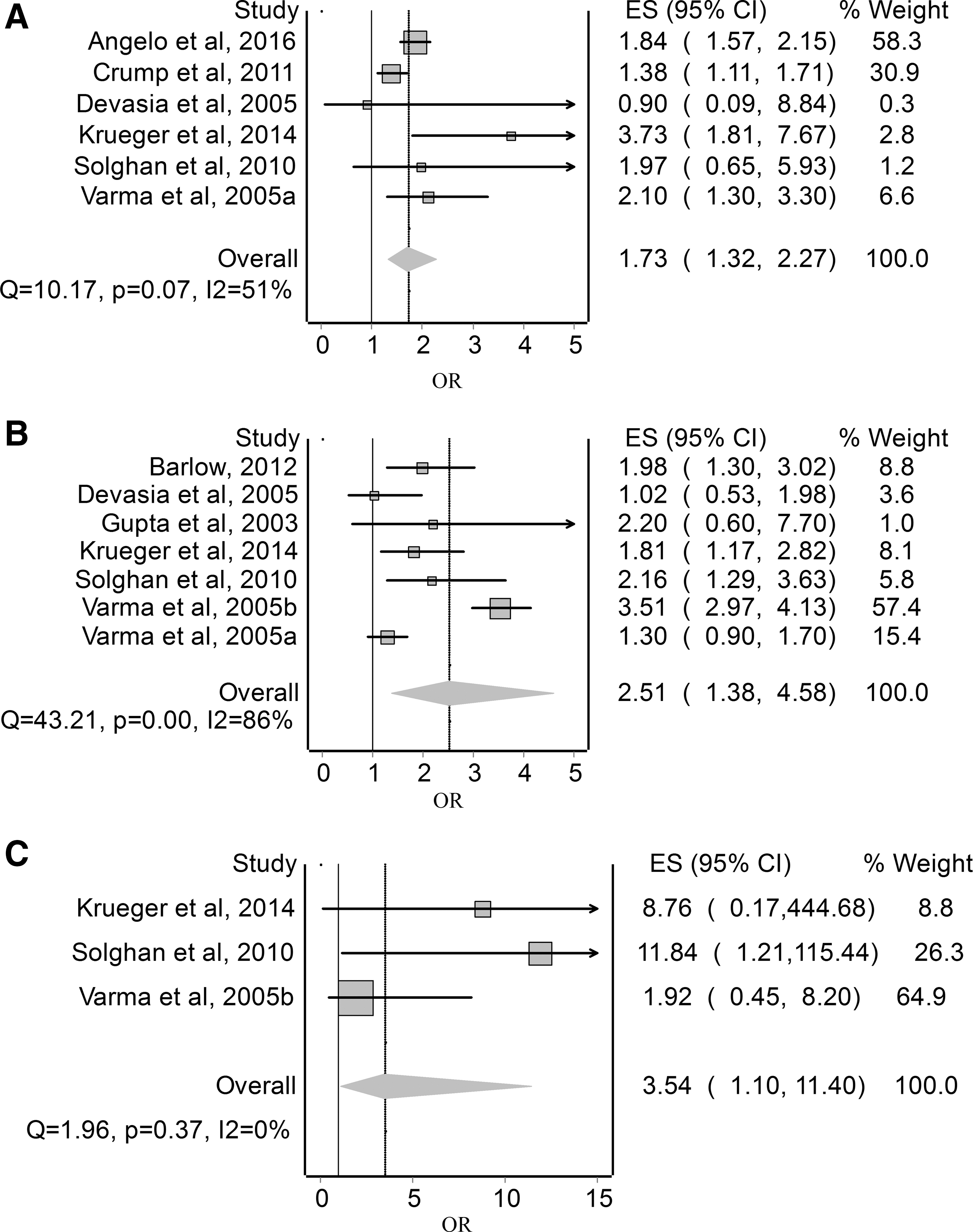
Forest plots for the OR of
The I2 index confirmed heterogeneity across studies comparing MDR and pan-susceptible NTS included in the analysis of bloodstream infections (I2 = 51%) and hospitalization (I2 = 80%), but not for the mortality analysis (I2 = 0%). On visual inspection and quantitative measure of Doi plots, we detected no asymmetry in the bloodstream infection analysis (LFK index: 0.39), but in the hospitalization and mortality analysis we detected major asymmetry (LFK index: −2.47, 3.37, respectively) suggesting possible publication bias (Appendix 8 in the Supplementary Data). Due to limited numbers of studies in each health outcome category, sensitivity analyses were performed by excluding one study at a time (Appendix 9 in the Supplementary Data).
In the subgroup analysis, the first group consisted of two studies reporting bloodstream infection and second group consisted of the four remaining studies reporting the source of the isolate. The pooled effect size of the first group (OR, 2.49; 95% CI, 1.43–4.33) was not statistically different from the second group (OR, 1.67; 95% CI, 1.34–2.08). Results for the subgroup analysis using the IVhet model are presented in Figure 3, remaining models are presented in Appendix 10 in the Supplementary Data.
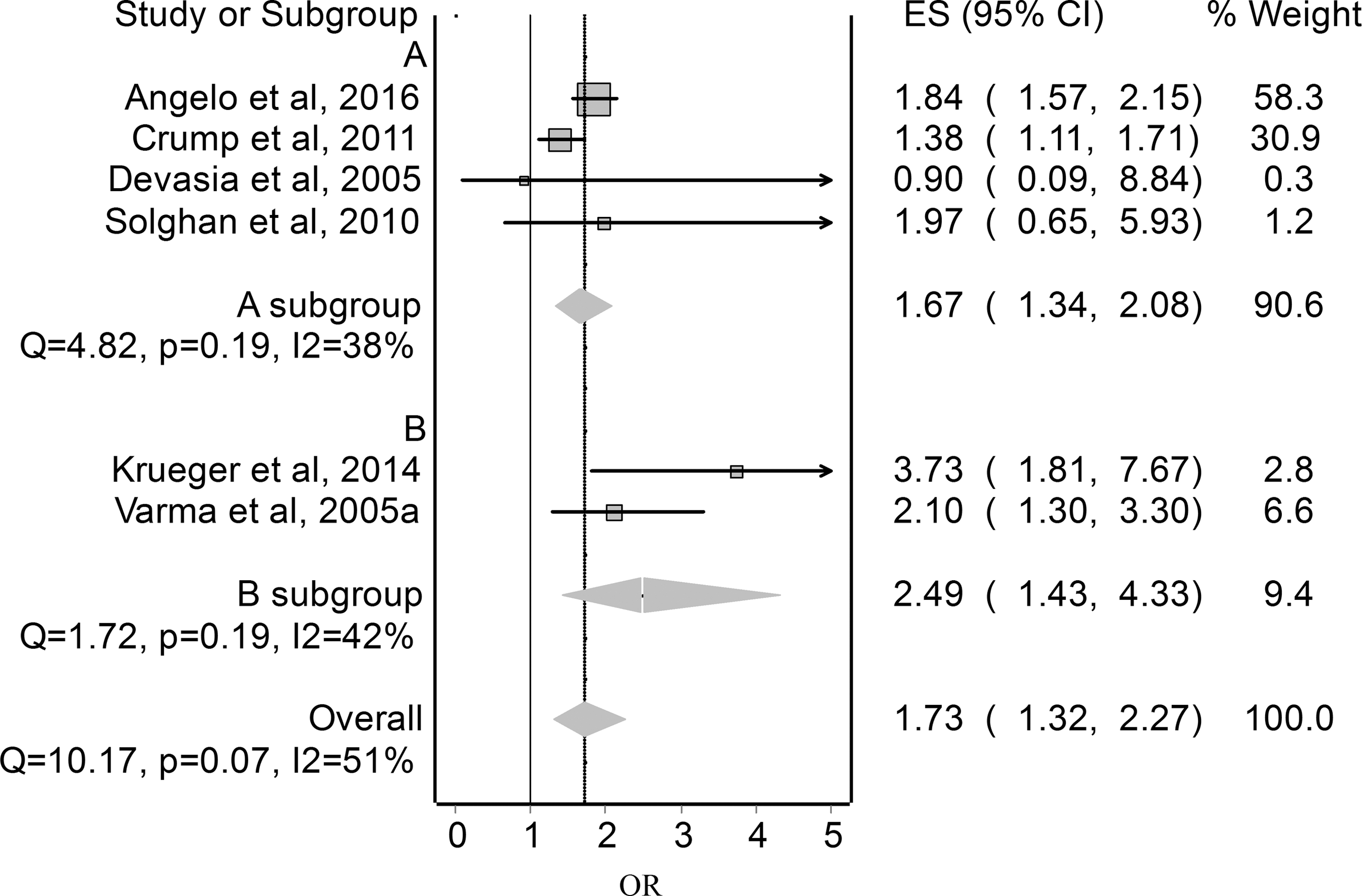
Forest plot for the OR of the subgroup analysis of bloodstream infection comparing MDR and pan-susceptible NTS, using the IVhet model. A subgroup: studies reporting “bloodstream infection,” B subgroup: studies reporting “blood isolate.” Horizontal lines represent 95% CIs for the study-specific effect size. The pooled OR is shown as a diamond. The middle of the diamond corresponds to the OR, and the width represents the 95% CI.
Discussion
Our systematic review and meta-analysis found higher severity of health outcomes from MDR NTS infections in high-income countries when compared with pan-susceptible NTS infections. Patients with MDR NTS infections were more likely to have bloodstream infection, to be hospitalized, and to die when compared with patients with pan-susceptible NTS infections.
There are several possible mechanisms by which multidrug resistance could cause poorer health outcomes. The initial therapy might be ineffective, resistance may result in use of a less desirable drug, or associations between virulence and resistance genes of the pathogen may cause more severe infections and prolonged duration (Barza, 2002). Varma et al. (2005b) found an association between multidrug resistance and hospitalization with bloodstream infection, but not between multidrug resistance and hospitalization with enteric infection. This suggests that patients with MDR infections may have higher hospitalization rates because they are more likely to have an invasive infection.
In terms of host factors, children and older adults (ages ≤5 and ≥65 years) have been found to have a higher risk of invasive disease (Parry et al., 2013), and underlying immunosuppressing conditions have been associated with generally poorer health outcomes (Gordon, 2008). Solghan et al. (2010) reported that patients with R-type ACSSuT infections were significantly older (median age, 41 years) than pan-susceptible cases (median age, 25 years). Crump et al. (2011) reported that the median age of patients with NTS bacteremia was 36 years compared with 20 years for patients with NTS stool isolates, with bacteremia more common in males and patients who were ≥65 years of age. Gupta et al. (2003) evaluated previous antimicrobial use and found no statistically significant difference between MDR and pan-susceptible groups.
Comorbidities can be a marker of other potentially relevant risk factors for MDR infections and invasive disease. As patients with comorbidities are more likely to be exposed to antimicrobial treatments and to healthcare settings, they might have a higher risk of acquiring invasive disease due to the loss of the protective effect of the normal gut flora, allowing MDR NTS populations to expand and potentially to also invade. Since only few studies reported data on host factors that are known to increase susceptibility to invasive disease (Koningstein et al., 2010), our analysis may be missing important unmeasured confounders.
This is the first meta-analysis and systematic review examining health outcomes from MDR and pan-susceptible NTS infections. Although we used a comprehensive search strategy, we recovered a limited number of studies, all of which were from the United States of America. We were only able to include crude ORs estimated from RRs or proportions reported by some studies, meaning that we may have not adequately controlled for age, sex, and other important factors.
Due to the limited number of studies and heterogeneity in study designs and outcomes, the role of serotype on the final health outcome could not be evaluated. However, all studies in our meta-analysis that looked at the proportion of invasive serotypes (Varma et al., 2005b; Crump et al., 2011; Barlow, 2012) were in line with previous study results, which found serotype Dublin as most invasive of all isolates, and serotype Newport less invasive than serotype Typhimurium (Jones et al., 2008). The biggest limitation of the study relates to the mortality analysis. The pooled OR reached significance in all models, but the CIs were very wide due to the small number of deaths.
Conclusions
Overall, the results of this meta-analysis link MDR NTS infections with poorer health outcomes. Given the lack of data outside the United States of America and potential confounders, there is a need for more adequately designed studies in different geographical areas. Since the use of antimicrobials in animal production, particularly in intensive animal feeding operations, is one of the key mechanisms for antimicrobial resistance in high-income countries, our study also highlights the need to reduce the use of medically important antimicrobials in food-producing animals as recommended by WHO (WHO, 2015, 2017b), and intervene to improve the background of the likely human health consequences of MDR NTS infections.
Footnotes
Acknowledgments
This work was supported by the Department of Agriculture and Water Resources, Canberra, Australia (K.G., M.D.K., A.P., S.V.). The authors thank the financial support provided by the Endeavour Scholarship (A.P.) and acknowledge all authors who provided additional data upon request. M.D.K. and D.J.G. are both recipients of research fellowships provided by the National Health and Medical Research Council, Australia.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.