
Abstract
Listeria monocytogenes is a facultative, intracellular foodborne pathogen that causes listeriosis and is prevalent worldwide. However, our knowledge of this bacterium and the listeriosis it causes is still extremely limited until now. Therefore, this retrospective study of patients in mainland China over 10 years (2008–2017) was performed to better understand the demographic trends and clinical features of listeriosis in China. Both electronic and manual retrieval systems were used to collect the relevant literature on listeriosis in mainland China. A total of 759 cases were reported from 22 provinces. Among the clinical cases, septicemia was the most common presentation (49%), followed by central nervous system infection (25%). The overall case fatality rate was 18%, with a higher rate among neonatal patients (73%). In recent years, listeriosis has been reported annually and even peaked in 2014. The median age of nonperinatal cases was 36 years (range, 0–102), with a predominance of male cases (52%). Sporadic cases were frequent from March to May. Efforts to prevent and control the spread of listeriosis are required through further research and collaborative efforts to improve the capacities of clinical diagnosis and treatment.
Introduction
L isteria monocytogenes is a nonspore-forming, facultative intracellular pathogen that causes sporadic and epidemic listeriosis (Radoshevich and Cossart, 2018). L. monocytogenes is a typical cold-tolerant bacterium that is resistant to its external environment and capable of multiplying slowly at low temperatures (ranging from −0.4°C to 45°C) (ICMSF, 1996) and reproducing at refrigeration temperatures. L. monocytogenes can also adjust to high salinity (10% NaCl) and can survive at pH 4.5–9 (Chawla et al., 1996).
Because of its unique biological features, L. monocytogenes is ubiquitous in nature and can cause listeriosis in animals through consumption of silage, thus causing human listeriosis by contaminated animal food. It can also contaminate farms, food-processing systems, and marketed products, such as dairy products and vegetables (Derra et al., 2013), causing sporadic or epidemic human listeriosis. The clinical symptoms of listeriosis include central nervous system (CNS) infection, septicemia, gastroenteritis, stillbirth, and abortion (Aguilar-Bultet et al., 2018). Older people, newborns, pregnant women, and immunocompromised patients are particularly susceptible to L. monocytogenes infection (Wang and Shen, 2015).
Listeriosis outbreaks occur frequently around the world. For example, in 2018, listeriosis in South Africa resulted in 1034 cases of illness and 204 deaths (Salama et al., 2018); in 2014, an outbreak in Denmark resulted in 37 deaths (Jensen et al., 2016); and in 2008, a listeriosis outbreak in Canada was associated with 23 cases of deaths (Thomas et al., 2015). In developed countries, such as European countries and the United States, acute foodborne clinical infections occur frequently, although the mortality rates are usually low. Although cases of listeriosis are not as common as other foodborne illnesses, the high case fatality–mortality rate makes it one of the most deadly foodborne diseases (Rebagliati et al., 2009). To effectively prevent and control the incidence of listeriosis, increased monitoring and control measures are essential.
According to epidemiological studies conducted by the U.S. Centers for Disease Control and Prevention, the incidence of listeriosis is estimated to be 0.3 per 100,000 persons in the United States, with a mortality rate of 21% (Tack et al., 2019). Therefore, many European countries and the United States have listed listeriosis as a notifiable disease and established monitoring systems (Feng et al., 2010b). Since 2000, China has made strong efforts to control listeriosis and improve the surveillance system for this disease. However, because of the relatively late start of this program, there is a paucity of data on the epidemiology of human listeriosis in China.
A recent report (Fan et al., 2019) investigated listeriosis in mainland China from 2011 to 2017 and found that there were 562 cases, with mortality rates of 32.68% in the perinatal period and 23.78% in the nonperinatal period. Feng et al. (2013) of the Chinese CDC retrieved the data on 147 clinical cases of listeriosis reported between 1964 and 2010. A review by Lian et al. (2014) identified a total of 84 clinical case reports, published between 2002 and 2012, using similar search methods. To investigate the prevalence of listeriosis in depth, we collected and reviewed cases of listeriosis that were reported in mainland China from 2008 to 2017 to analyze the clinical manifestations and epidemiological features of this disease in China in the past decade and to provide a theoretical basis for its effective prevention and control.
Materials and Methods
Sources of materials
Between January 2008 and December 2017, we searched for reports of listeriosis using the following key words: L. monocytogenes, Listeria monocytogenes, Listeria ivonovii, listeriosis, listeriosis infection, listeriosis case, and Listeria epidemiology. Computer and manual retrieval systems were used to search full texts in the literature. Data on listeriosis reported between 2008 and 2017 were collected from five primary academic electronic databases in mainland China: China KnowledgeNet (CNKI); Wipper Journal Resource Integration Service Platform; Wanfang (Wanfang Data full-text database); Web of Science; and the National Center for Biotechnology Information (NCBI) database. We identified and deleted duplicate cases from the clinical case reports based on basic patient data, age, and treatment results.
Definition and classification of cases
The patients in the clinical case reports were divided into two groups according to their clinical symptoms: (i) perinatal period: pregnant women and newborns (<28 days old); and (ii) nonperinatal period: all cases other then perinatal cases. In the perinatal period, a perinatal case was only classified as maternal when the mother had an abortion or stillbirth attributed to listeriosis. The cases were also classified into three groups according to the site of infection: (i) CNS infection, where Listeria was isolated from either blood or CNS specimens and confirmed by a doctor as a CNS infection; (ii) septicemia, where Listeria was cultured from the blood, but no CNS involvement was diagnosed by a doctor; and (iii) focal infection, where Listeria was detected in neither a CNS specimen nor blood (Feng et al., 2013).
Statistical methods
We included the relevant statistics for the patient demographic data (e.g., sex and age) and clinical courses (e.g., underlying disease, time of onset, symptoms, therapy, duration of hospitalization, and outcome) obtained from the clinical literature (Wang et al., 2013). All statistical analyses were performed with SPSS 16.0. The t-test was used to assess significant differences between two independent samples, while count data were analyzed by the chi-square test. A p-value <0.05 was defined as statistically significant.
Results and Analysis
Survey of clinical case reports
The database search yielded 3780 articles, as shown in Figure 1. Among these, 1880 were selected by index, title, authors, journal, and abstract. We subsequently identified and deleted 1648 duplicate articles after reading the titles and abstracts. Fifty-eight articles were excluded as they were not relevant to humans or without description of listeriosis cases in mainland China. Thus, a total of 174 articles were identified for further case study from January 2008 to December 2017. A total of 759 cases of listeriosis that occurred between 2008 and 2017 were reviewed for their details. These involved 245 nonperinatal patients (32%) and 514 pregnancy-related patients (68%). Among the 622 cases in which the sex of the patient was known, there were a bit more female cases than male cases (321 vs. 301). However, in 138 cases, the patient's sex was not provided. The patients most frequently suffered septicemia (49%) or meningitis (25%). In the nonperinatal period, a total of 116 (15%) patients suffered immune deficiency. Many of these patients had several diseases associated with immune deficiency, including hematological malignancies (39 cases), systemic lupus erythematosus (12 cases), and human immunodeficiency virus infection (1 case).
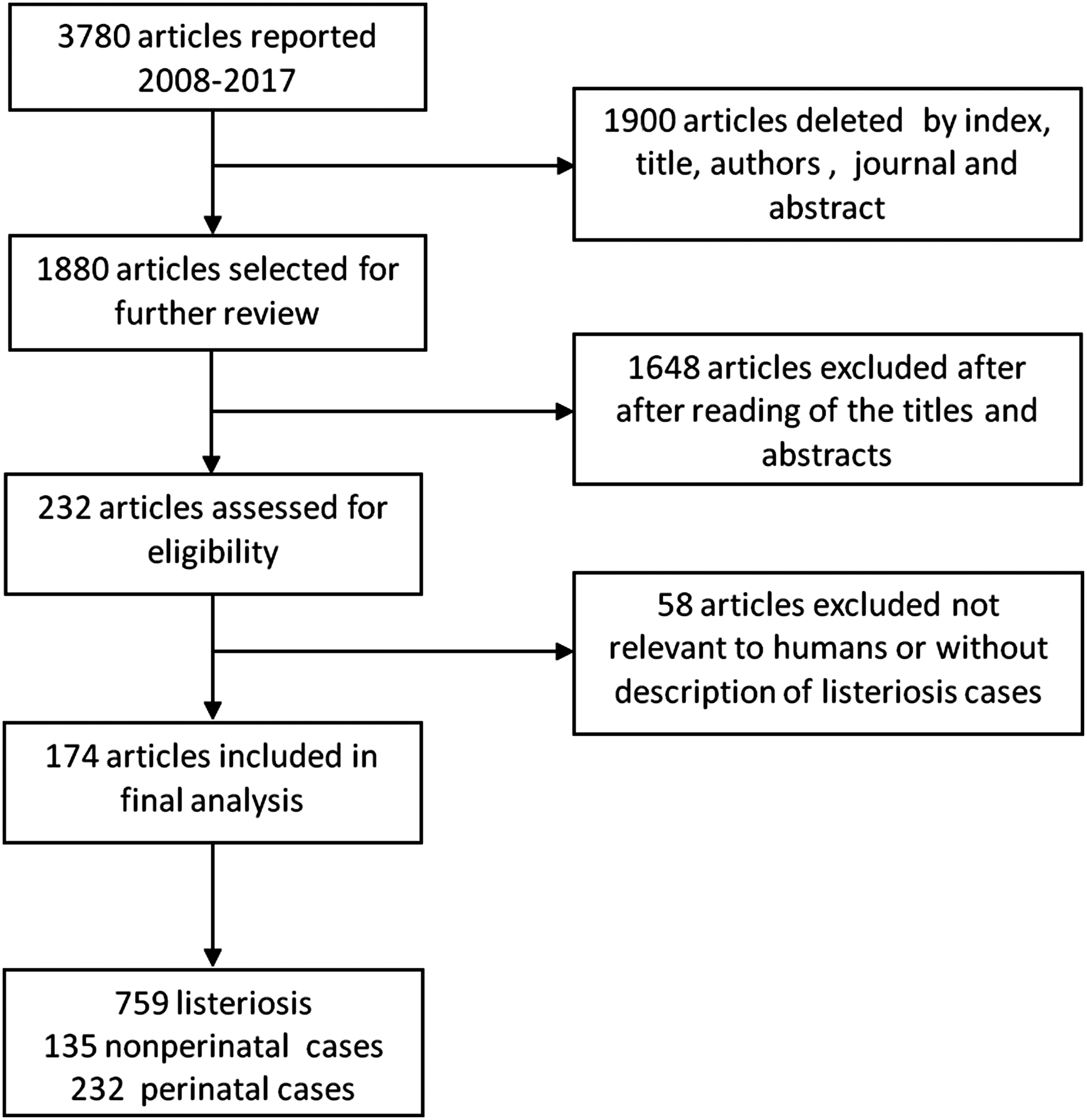
Flowchart of the search strategy.
Clinical symptoms of listeriosis
Clinical symptoms of perinatal cases
The total 514 cases that occurred in the perinatal period comprised 116 pregnant women and 398 neonates. Among pregnant women, 103 patients had intrauterine infections (89%), in all of which only Listeria was isolated from the cervical secretions. This was followed by septicemia in 22% of cases (Fig. 2A). Fever was the most frequently reported symptom and was sometimes accompanied by abdominal pain, dry cough, nausea, vomiting, headache, dyspnea, and other symptoms.
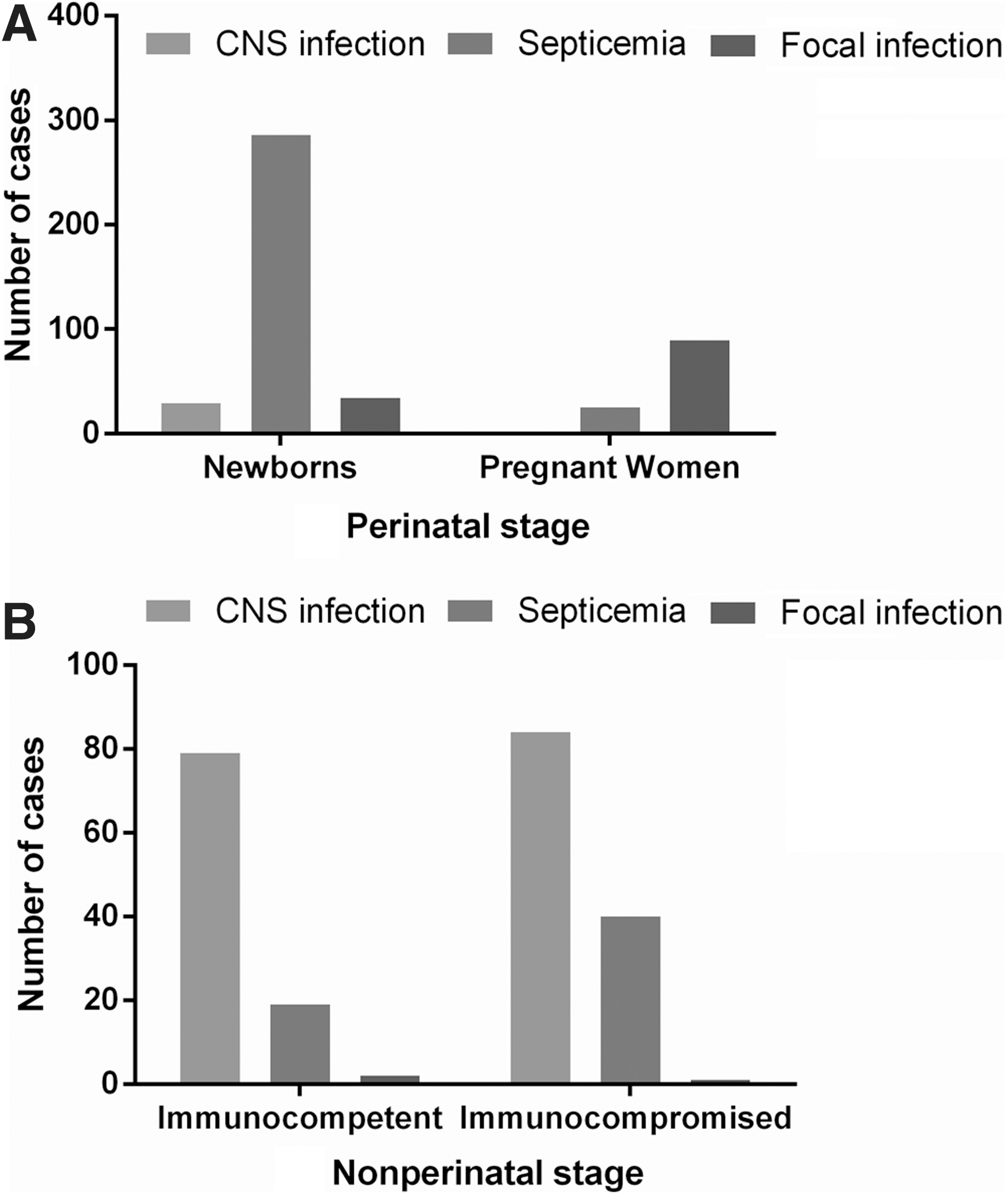
Types of human listeriosis infections in mainland China, 2008–2017.
Clinical and laboratory information about their offspring was available for 116 pregnant patients. Of these, 64 newborns suffered Listeria infections (55%), 35 of whom died after abortion or stillbirth (30%), and 14 (12%) suffered fetal death. Only one (1%) pregnant woman recovered satisfactorily from the infection and gave birth to a healthy infant not infected with Listeria. The fetal outcome of only one patient was unreported. Of the 41 pregnant women who had contracted their Listeria infections from food, 18 (44%) were infected after consuming cold food, such as ice cream, cold drinks, chilled lo mei, frozen strawberries, and raw cucumbers; 17 (41%) were infected after consuming unsanitary food, such as barbecued food; and 6 (15%) were infected after consuming seafood, such as salmon sashimi.
As shown in Figure 2A, the main presentation of the neonatal infections was septicemia (72%), followed by CNS involvement with septicemia (12%), CNS infection (7%), and other lesions (9%), including bloodstream infection, neonatal pneumonia, and intracranial hemorrhage.
Clinical symptoms of nonperinatal cases
Information on symptoms of nonperinatal cases was recorded for 245 cases: 163 (67%) patients had CNS infections, 59 (24%) had septicemia, 3 (1%) had focal infections, and 20 (8%) had CNS infection and septicemia. It is noteworthy that the main presentation in both immunocompromised patients (67%) and immunocompetent patients (79%) was meningitis (Fig. 2B). These patients had a median age of 36 years (range 0–102 years); 69 patients (32%) were aged 204 days–20 years; 107 patients (49%) were aged 21–60 years; and 41 patients (19%) were >60 years old (Fig. 3). Of these, immunocompromised patients were older than immunocompetent patients (p < 0.05). Among the 219 patients whose sex was reported, 114 were male and 105 were female.
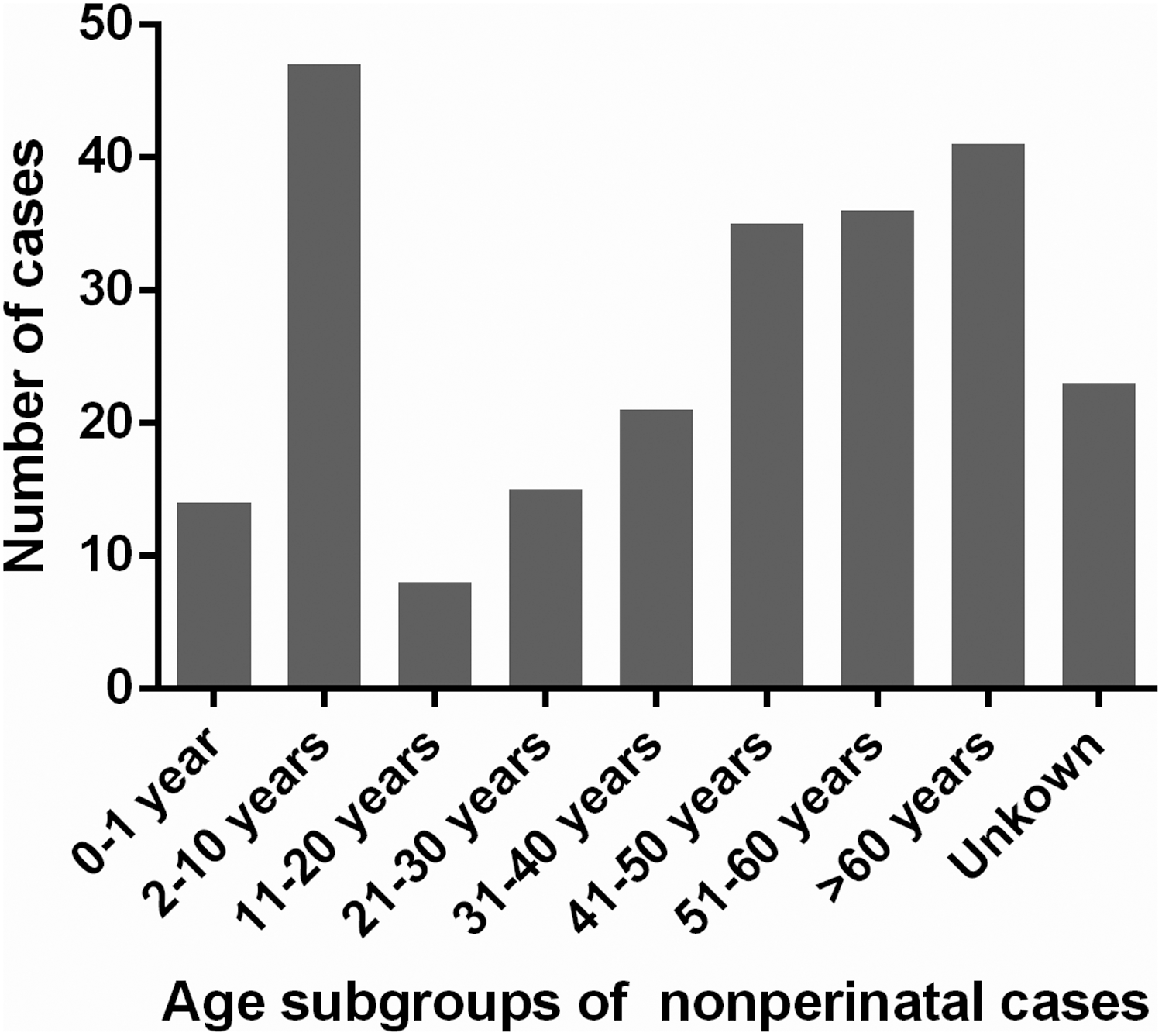
Age subgroups of nonperinatal cases. Distribution of human listeriosis by age group, 2008–2017. The youngest age group was 204 days–20 years. There were 23 cases of unknown age.
Outcomes
Data on the outcome were available in 725 cases, 423 were cured, 134 improved, and 128 died. The total case fatality rate was 18% (Table 1). Twenty-one patients (17%) died of CNS infections and 92 patients (72%) died of septicemia. As shown in Table 1, the highest mortality rate was among neonates (23%), followed by immunocompromised patients (20%) and immunocompetent patients (2%), and the lowest rate was among pregnant women (0%). Seventeen patients had sequelae after treatment.
Outcomes of Listeriosis in Humans
After the disease is treated, the symptoms disappear and the function is fully restored.
After the disease is treated, the symptoms and signs improved.
AAD, against advise discharge; If the patient is still not cured after treatment, patient or family member is required to be discharged.
Includes patients with autoimmune diseases. Blood/tumor (n = 29), systemic lupus erythematosus (n = 12), and AIDS (n = 1).
Hydrocephalus (n = 1), movement disorder (n = 6), epilepsy (n = 1), mental retardation (n = 1), moderate disability (n = 1), and intracranial hemorrhage and reduced limb activity (n = 1).
Among the 228 nonperinatal cases whose outcomes were reported, 35(27%) died: 15 deaths were attributed to CNS infections and 11 were caused by septicemia. Among these patients, the mortality rate in immunocompromised patients (21%) was higher than that in immunocompetent patients (10%). Of the 497 perinatal cases whose outcomes were reported, 93 (19%) died: 81 from septicemia and 6 from CNS infections.
Geographic distribution of cases
The cases of listeriosis included in this study were reported in 22 of the 31 mainland provinces of China. The five provinces with the largest total numbers of cases were Beijing (n = 259), Sichuan (n = 113), Zhejiang (n = 63), Liaoning (n = 39), and Shaanxi (n = 30) (Fig. 4).
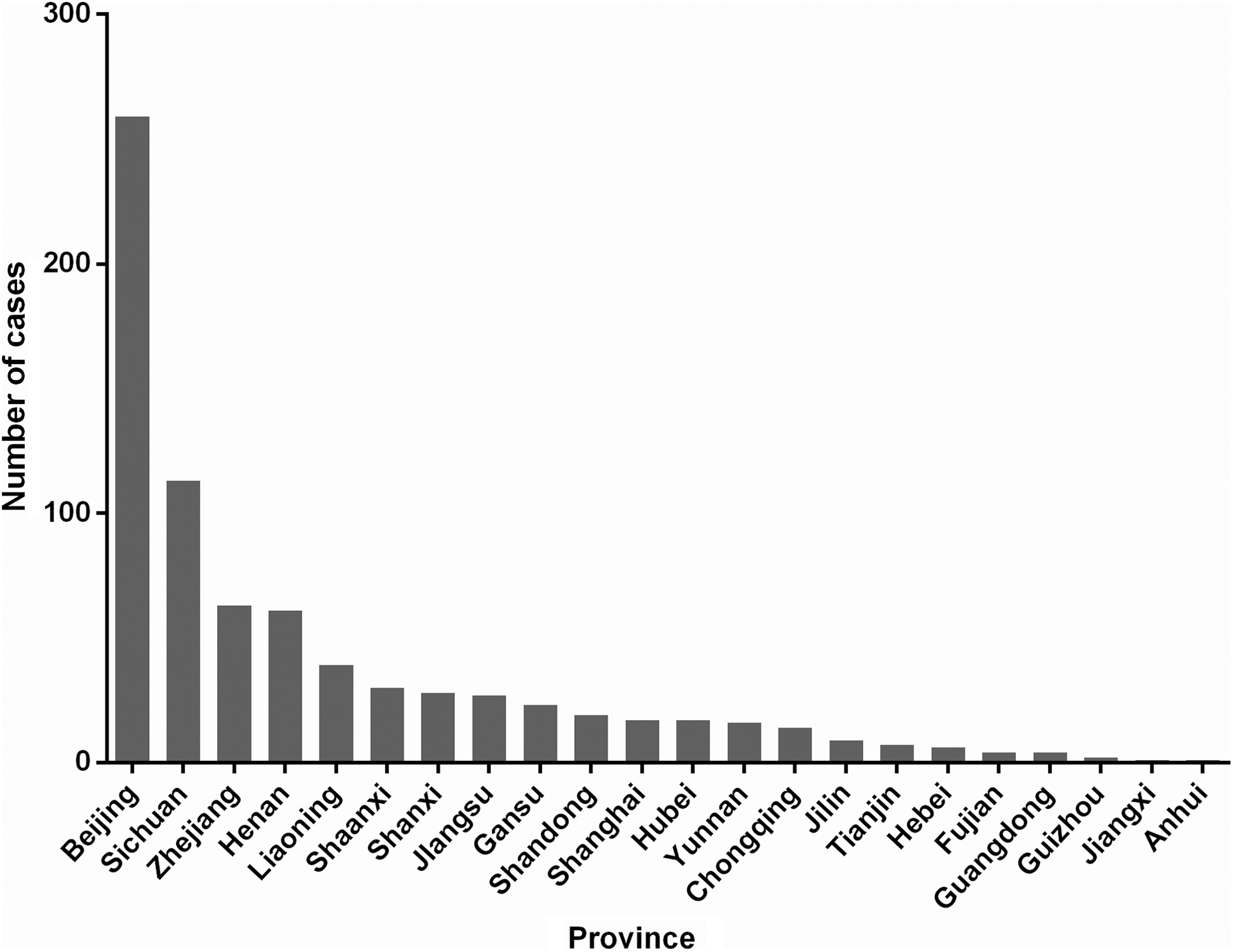
Distribution of listeriosis cases in different areas. Twenty-two provinces were involved in the survey. Beijing (n = 130) and Sichuan (n = 80) reported the greatest numbers of listeriosis patients.
Yearly and seasonal distributions of cases
Overall, the year of infection was recorded in the clinical case reports of 217 patients. As shown in Figure 5, the number of cases reported was highest in 2014 (33 cases), followed by 2013 (26 cases) and 2012 (20 cases). In 2011–2014, the number of cases showed a slow upward trend and then decreased each year.
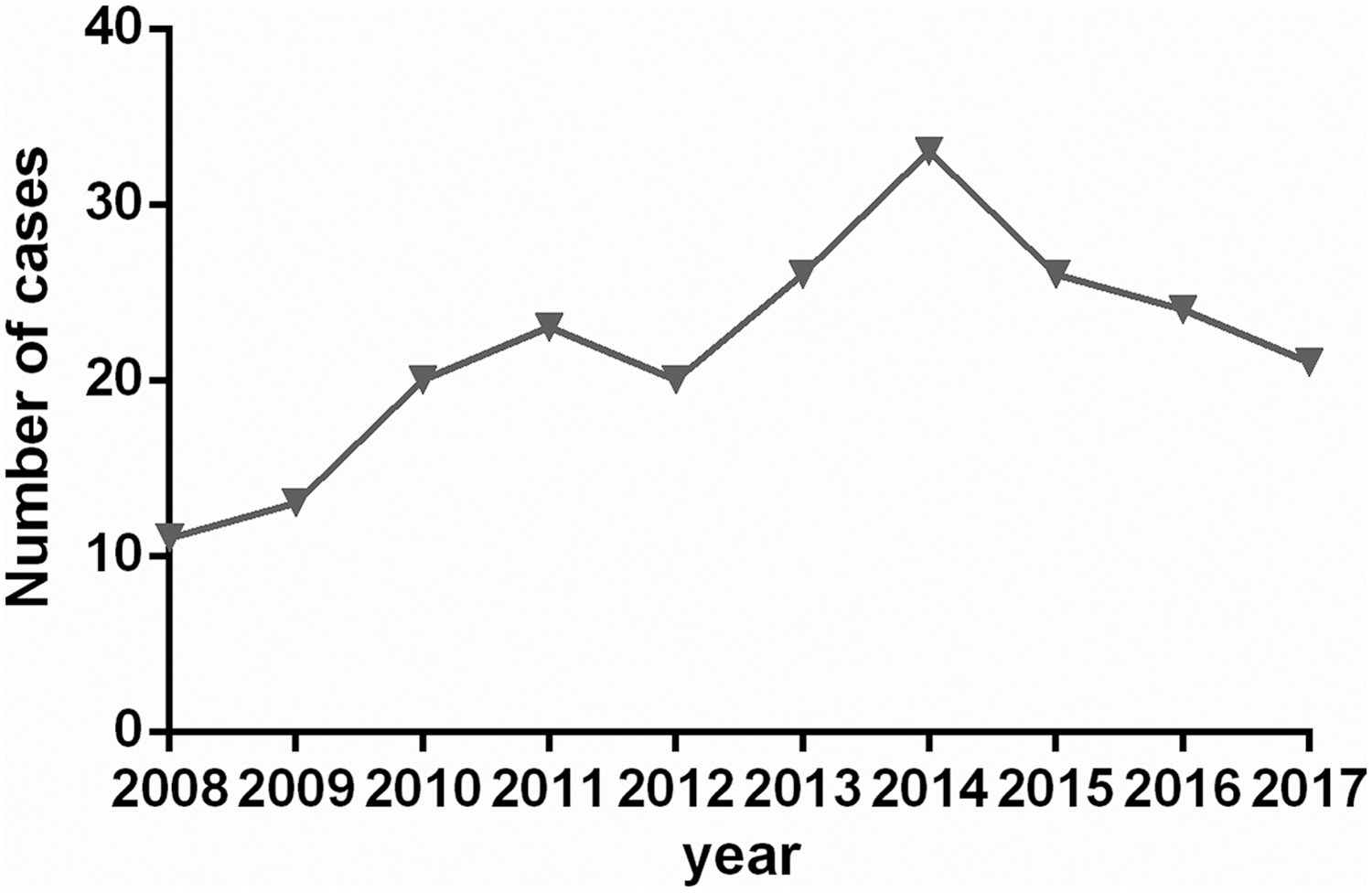
Distribution of listeriosis cases in humans from 2008 to 2017. Infection occurred from 2008 to 2017.
The specific month of infection could be determined from the clinical case reports for only 131 patients. Infection occurred throughout the year, but was most often concentrated between March and May, so predominantly during spring and summer. However, the value of this inference is limited because few seasonal data were provided (Fig. 6).
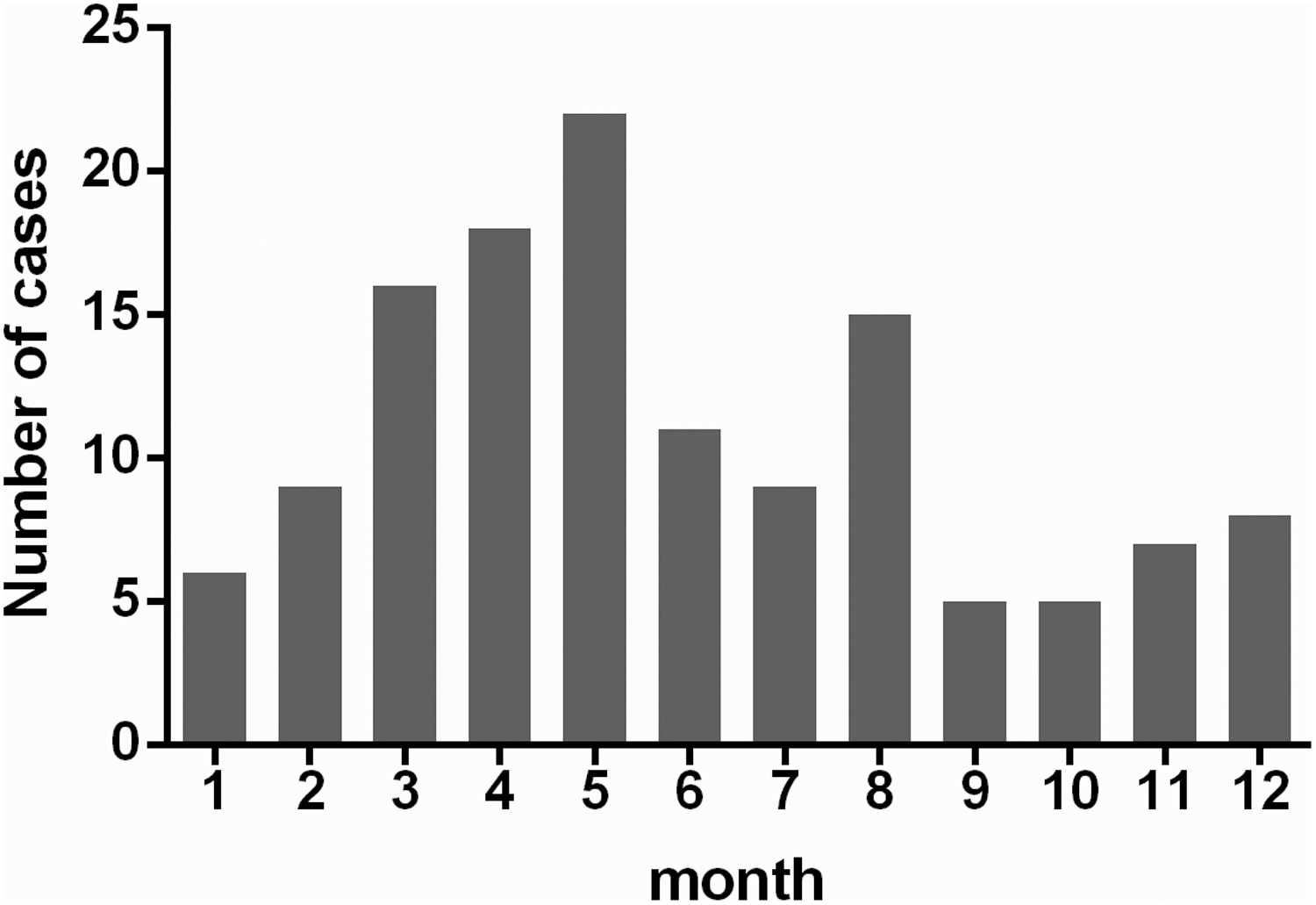
Distribution of listeriosis in different months from 2008 to 2017, including 57 patients with information on the specific date of illness onset.
Discussion
Listeriosis is a notifiable disease in many developed countries, but China has not added listeriosis to its list of notifiable diseases (Feng et al., 2010a; Feng et al., 2011). Thus, the current epidemiological data for listeriosis in China are limited and its transmission routes and key control points remain to be explored. Therefore, we retrospectively reviewed 174 articles (759 cases) published in mainland China between 2008 and 2017 to examine the epidemiology of human listeriosis in China over a period of 10 years, while those in the study by Fan et al. (2019) were reported between 2011 and 2017 (759 vs. 562).
In this retrospective study, we found that listeriosis was sporadic in mainland China during this period and presented predominantly as septicemia (49%), followed by CNS infection (25%). The total mortality rate was 18%, which is significantly lower than the international average rate of 30% (Lomonaco et al., 2015). The reason is possibly related to the different dominant clonal complexes (CCs) present in China and outside China. The major CCs that cause human listeriosis outbreaks abroad are CC1, CC6, CC2, and CC4 (Yin et al., 2015). Maury et al. (2016) found that CC1, CC6, CC4, and CC2 are the dominant CCs causing listeriosis in Western countries, whereas CC4, carrying virulence island 4 (LIPI4), has greatest pathogenicity and can cross the blood–brain barrier (Vázquez-Boland et al., 2001). According to the literature, the CCs detected in Chinese food are CC87, CC9, and CC8 (Wang et al., 2018). Because isolates of different CCs differ in their virulence and pathogenic tendencies, they also differ in their associated clinical symptoms and mortality rates. The sporadic features of listeriosis are closely related to the unique CCs (CC8, CC9, and CC87) in China (Huang et al., 2015).
Listeriosis is a foodborne disease that is often associated with L. monocytogenes-contaminated food. Although listeriosis occurs throughout the year in China, the clinical reports analyzed in this study show that the human disease is mainly concentrated in March–May, and peaks in May, unlike the results reported in the United Kingdom and Scotland (Campbell, 1990; McLauchlin 1990a, b). A similar seasonal variation observed in this study has been reported in other Chinese studies (Fan et al., 2019), which may be related to the pattern of Listeria infection in China. Interestingly, the incidence of listeriosis in ruminants is highest in March–April (Wesley et al., 2002), although human listeriosis arises from ingestion of contaminated food. This suggests that food safety must be guaranteed from the farm to the plate and that it is essential to strengthen the monitoring of animal product hygiene to control the spread of L. monocytogenes along the food chain and to reduce the risk of infecting consumers. Accordingly, the Codex Alimentarius Commission, the European Union, the United States, Japan, New Zealand, Australia, Canada, and other countries have set standard requirements for pathogenic bacteria in ready-to-eat food and raw food (Risk, 2004).
According to an infectious disease surveillance map produced by the European Centre for Disease Prevention and Control, the incidence of listeriosis was significantly controlled in countries such as Germany, Britain, and Denmark after implementation of the standards (Huang et al., 2015). In 2014, China issued the limitation of pathogenic bacteria in food (GB29921-2013) standard to establish a zero-tolerance policy for L. monocytogenes in ready-to-eat meat products to control food contamination and prevent foodborne diseases (Li et al., 2018). Frequently reported vehicles of infection include soft cheeses, refrigerated food, cooked meat products, raw vegetables, and seafood, etc. (Derra et al., 2013). It is worth noting that in this study, we found that cases of listeriosis were reported in mainland China every year and reached a peak infection rate in 2014. However, a zero-tolerance policy was established in the same year and subsequently implemented in various areas. The incidence rate then dropped significantly each year from 2015 to 2017. With the establishment and implementation of several policies to strengthen food hygiene and safety, the state will be able to prevent and control listeriosis, improve food safety, and ensure human health.
In this study, the top five provinces with the largest total number of cases were different from those in the study by Fan et al. (2019). The patients with listeriosis lived in various regions of mainland China, and an obvious correlation was observed between listeriosis in patients and their geographic distribution (Lee et al., 1992), which might be associated with the eating habits in different regions. Hospitals in Sichuan also reported many cases of listeriosis, and hot pots and barbecues are very popular in Sichuan. Hospitals in Beijing also reported many cases, whereas the contamination rate of food with Listeria in Beijing was not higher than in other provinces or cities (Li et al., 2018). This may indicate that Beijing has much better medical facilities and more effective diagnostic procedures. Because the symptoms of human listeriosis are easily confused with those of other pathogens, such as influenza and CNS infections (Lian et al., 2014), listeriosis is difficult to diagnose in a hospital with poor medical services. Therefore, listeriosis could be effectively diagnosed in regions with better medical services.
Listeria monocytogenes, Campylobacter, Salmonella, and Vibrio parahaemolyticus are the first four pathogens causing foodborne diseases (Realpe et al., 2016). They are foodborne zoonotic pathogens that are important public health issues both at home and abroad. Our findings show that most provinces in mainland China have reported cases of listeriosis annually, with an average case fatality rate of 18%, whereas the mortality rate is up to 73% among neonatal patients. Therefore, it is a serious threat to human health. Further epidemiological studies are required to determine the transmission routes and epidemic principles of listeriosis in China and to develop and implement targeted preventive measures to reduce the incidence of listeriosis. Because China is a large country, with a population of about 1.4 billion, it is imperative to improve our surveillance and control of listeriosis.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the National Key R&D Program of China (2017YFC1601201 and 2018YFD0500502), the National Natural Science Foundation of China (No. 31472193), Key Research and Development Program (Modern Agriculture) Project of Jiangsu Province (BE2017341), Jiangsu Agricultural Science and Technology Independent Innovation Funds [CX(16)1028], the Science and Technology Support Program of Jiangsu Province (BE2012367), and the Priority Academic Development Program of Jiangsu Higher Education Institutions.