
Abstract
Burden of disease metrics are increasingly established to prioritize food safety interventions. We estimated the burden of disease caused by seven foodborne pathogens in Denmark in 2017: Campylobacter, Salmonella, Shiga toxin–producing Escherichia coli, norovirus, Yersinia enterocolitica, Listeria monocytogenes, and Toxoplasma gondii. We used public health surveillance data and scientific literature to estimate incidence, mortality, and total disability-adjusted life year (DALY) of each, and linked results with estimates of the proportion of disease burden that is attributable to foods. Our estimates showed that Campylobacter caused the highest burden of disease, leading to a total burden of 1709 DALYs (95% uncertainty interval [UI] 1665–1755), more than threefold higher than the second highest ranked pathogen (Salmonella: 492 DALYs; 95% UI 481–504). Campylobacter still led the ranking when excluding DALYs attributable to nonfoodborne routes of exposure. The total estimated incidence was highest for norovirus, but this agent ranked sixth when focusing on foodborne burden. Salmonella ranked second in terms of foodborne burden of disease, followed by Listeria and Yersinia. Foodborne congenital toxoplasmosis was estimated to cause the loss of ∼100 years of healthy life, a burden that was borne by a low number of cases in the population. The ranking of foodborne pathogens varied substantially when based on reported cases, estimated incidence, and burden of disease estimates. Our results reinforce the need to continue food safety efforts throughout the food chain in Denmark, with a particular focus on reducing the incidence of Campylobacter infections.
Introduction
Foodborne diseases (FBDs) have been recognized as an important health concern in Denmark for decades. High incidence of human cases and/or large impact outbreaks at different points in time have motivated the implementation of comprehensive pathogen-specific control plans, for example, focused on Salmonella spp. (Wegener et al., 2003), Listeria spp. (EC, 2005), and Campylobacter spp. (Rosenquist et al., 2009; Fødevarestyrelsen, 2018). These action plans have had varied degrees of success. For example, although Salmonella control programs have resulted in a substantial decrease in the reported incidence of salmonellosis, Campylobacter action plans have had limited effect (Wegener, 2010).
Notifications of cases to public health surveillance suggest changes in the relative importance of diseases and effectiveness of intervention strategies over time, but the overall impact of FBD in Denmark is largely unknown. It is widely recognized that reported cases represent only the “tip of the iceberg,” and that for many pathogens the true incidence of disease in the population is unknown (Mead, 1999; Majowicz et al., 2010; Scallan et al., 2011; Kirk et al., 2014). Only a fraction of all cases caused by contaminated foods are captured by public health surveillance systems. For a case to be identified, the ill person must seek medical care; the doctor must request a fecal sample; the causative pathogen must be identified at a laboratory; and the results must be reported to public health officials. Any dropouts in this process lead to underdiagnosis and underreporting, which varies between causative agents depending on the severity of symptoms and the awareness about the pathogen (Haagsma et al., 2012). In addition, FBDs have a wide variety of manifestations with different severity, duration, and sequelae, and comparisons based solely on incidence do not provide a complete picture of their relative public health impact (Havelaar et al., 2012). Health metrics that incorporate these parameters such as the disability-adjusted life year (DALY) are increasingly accepted as a way to translate and compare the health impact of FBDs and facilitate evidence-based risk ranking (Havelaar et al., 2015; Cassini et al., 2016).
The objective of this study was to estimate the incidence and foodborne burden of disease (in DALYs) of seven pathogens in Denmark, a country with a free public health care system and nationwide data on notifiable FBDs available.
Materials and Methods
We estimated the burden of disease caused by five enteric pathogens (four bacteria: Salmonella, Campylobacter, Yersinia enterocolitica, and Shiga toxin–producing Escherichia coli [STEC] and one virus: norovirus) and two invasive pathogens, the bacteria Listeria monocytogenes and the parasite Toxoplasma gondii. Pathogens were selected on the basis of their public health relevance, reflected either by reported incidence, number of outbreaks, or severity of symptoms. Among these seven agents, only the enteric bacterial infections were notifiable in Denmark.
The enteric bacteria and norovirus cause mild-to-severe gastroenteritis, and may lead to severe sequelae or death. T. gondii infections can be prenatal (leading to congenital toxoplasmosis [CT]) or postnatal (referred to as acquired toxoplasmosis). Owing to lack of data on the latter, we only included the congenital form. CT may lead to fetal death, neonatal death, or neurological lifelong symptoms in young children. Infection with L. monocytogenes can cause mild disease in otherwise healthy people, manifesting with usually mild and self-limiting gastroenteritis. However, in high-risk groups such as the elderly, immunocompromised or fetus and neonates (in utero infection), infection can be invasive and lead to severe clinical disease, manifesting as sepsis, meningitis or encephalitis, spontaneous abortion, and death (Jensen et al., 2016). We included only the invasive form of listeriosis.
To estimate the FBD burden for all pathogens in 2017, we (1) estimated the incidence and mortality of each, (2) estimated the disease burden of all health outcomes of each pathogen in terms of DALYs, and (3) linked these estimates with estimates on the proportion of the total burden that is attributable to foods. Detailed methodology of each step is presented hereunder and in Appendices A1–A4.
Incidence and mortality
We applied different approaches to each pathogen to estimate the total incidence of disease and mortality dependent on available data.
Enteric bacterial infections
In Denmark, human Salmonella, Campylobacter, STEC, and pathogenic Y. enterocolitica infections are notifiable through the laboratory surveillance system. Physicians send specimens from suspected cases to one of the clinical microbiology laboratories, the laboratories report positive results to the National Public Health Institute (Statens Serum Institut [SSI]) within 1 week, and results are recorded in the Register of Enteric Infections maintained by SSI (
To adjust for underdiagnosis and underreporting of enteric bacterial infections, we reconstructed the surveillance pyramid as described by Haagsma et al. (2012). The model consists of a set of nonpathogen-specific and pathogen-specific parameters defined by probability distributions (Appendix Tables A1.1 and A1.2). These parameters were informed by data collected through a population-based telephone survey conducted in 2009 (Müller et al., 2012), by evidence from National Health Registries, or by literature review. Estimated multipliers were applied to surveillance data from 2017 (available at
Norovirus infection
There is no reporting system for norovirus infections or for gastroenteritis outbreaks in Denmark, except for suspected foodborne outbreaks. Because reported outbreak-related cases only represent a small fraction of total cases, these data were insufficient to describe the epidemiology and public health impact of the disease. To estimate the total incidence of norovirus infections in Denmark, we adapted a previously described approach (Pires et al., 2015). In brief, we collected the total national diarrhea incidence and mortality envelopes as published by the Global Burden of Disease Study (available at
Congenital toxoplasmosis
The incidence of CT was estimated on the basis of a cohort study. The Danish National Neonatal Screening Programme for Congenital Toxoplasmosis (DNNSP) was conducted from January 1, 1999, to July 31, 2007 (Schmidt, 2005; Schmidt et al., 2006) and included >98% of all newborns in Denmark. We assumed that the incidence of CT in newborns observed during the DNNSP was applicable to 2017. The screening method applied in the cohort was expected to identify 70–80% of newborns with CT. We combined the observed average annual incidence of CT per 10,000 live born children with the number of live born children in Denmark in 2017 (Statistics Denmark, available at
Invasive listeriosis
Because invasive listeriosis is a severe illness, all cases in the population were assumed diagnosed and notified to the public health surveillance system. Age and gender-specific incidence of listeriosis in 2017 was collected from the National Listeria Surveillance database (available at
Health outcomes and mortality
All included infections can lead to more than one symptom and/or sequelae. The possible health outcomes of each infection were identified through literature review, and were described in an outcome tree. All outcome trees and probabilities of exhibiting each outcome after infection are presented in Appendix A4. All enteric infections cause diarrhea and/or vomiting, which define the incident case; in other words, all cases caused by each enteric pathogen will manifest this outcome. The sequelae varied between pathogens with only some similarity. Specifically, salmonellosis, campylobacteriosis, and yersiniosis may all lead to the sequelae reactive arthritis (ReA) and irritable bowel syndrome (IBS). Guillian–Barré syndrome is a potential sequelae of campylobacteriosis, and STEC infections can lead to hemolytic uremic syndrome and end-stage renal disease. No possible sequelae were considered for norovirus infections. All enteric infections may cause death.
The invasive infections CT and listeriosis have different manifestations. CT comprises a variety of health outcomes, and children may be symptomatic at birth, affected later in life, or remain apparently asymptomatic. Health outcomes of CT were defined as by Havelaar et al. (2007b): fetal loss, sequelae manifesting in the first year of life (chorioretinitis, intracranial calcification, hydrocephalus, central nervous system (CNS) abnormalities, and neonatal death), and sequelae appearing after the first year of life (chorioretinitis). Nonspecific symptoms after CT (e.g., anemia, jaundice, pneumonitis, and diarrhea) were not included. CT was only considered possible for infants of previously seronegative mothers who became infected during pregnancy; the possibility of periconceptional transmission or vertical transmission in mothers deemed seropositive before conception was excluded. Detailed information on the classifications has been published previously (Nissen et al., 2017).
For listeriosis, we followed the model defined by the European Centre for Disease Control and Prevention (ECDC, 2015), which accounted for the probability that acquired invasive symptomatic cases present with meningitis and for the probability of death after infections. For perinatal cases, the disease burden for health outcomes of early- and late-onset listeriosis is combined into one category.
Disability-adjusted life years
DALYs are the sum of years lived with disability (YLD), and the years of life lost (YLL) due to premature death caused by a disease (Devleesschauwer et al., 2014). For each disease, we combined the estimated incidence of each health outcome with disability weights previously collected (Salomon et al., 2015) with duration of disease and life expectancy statistics as published by Denmark Statistics (available at
Input Parameters for the Calculation of Disability-Adjusted Life Years of Seven Foodborne Pathogens
CT, congenital toxoplasmosis; GP, general practitioner; STEC, Shiga toxin–producing Escherichia coli.
Proportion attributed to foodborne transmission
To estimate the burden of disease that was due to consumption of contaminated foods, we applied the attributable foodborne proportions to the total disease burden, previously estimated by Hald et al. (2016). This study conducted a global expert elicitation, with expert panels representing different world regions and groups of hazards, to estimate attribution proportions for foodborne, environmental, direct contact, or person-to-person transmission. Because estimates were not produced at a national level, we applied estimates for the subregion that includes Denmark (WHO subregion EUR-A), which corresponds to European countries with very low child and adult mortality (
Results
Incidence of disease
In 2017, 4231 cases of campylobacteriosis, 1065 cases of salmonellosis, 354 cases of yersiniosis, 338 cases of STEC infections, and 58 cases of listeriosis were reported to the Danish public health surveillance system. No cases of CT were notified, and 298 outbreak-associated norovirus infections were registered. When correcting for underreporting and underdiagnosis, we estimated that 185,060 cases of norovirus (95% uncertainty interval [UI] 156,506–212,627), 58,141 cases of campylobacteriosis (95% UI 49,617–71,781), 10,386 cases of salmonellosis (95% UI 8792–12,153), 5019 cases of yersiniosis (95% UI 4312–5839), 10,565 cases of STEC (95% UI 7209–14,562), and 10 cases of CT (95% UI 8–12) occurred in Denmark in 2017 (Table 2). The incidence of norovirus infection was significantly higher in children <5 years of age (21,657 cases per 100,000 population) than in older age groups (between 1500 and 3200 in age groups between 5 and 69 years, and 5200 in >70 years of age) (see detailed results in Appendix Table A2.B). Among bacterial infections, age and gender differences were larger for Campylobacter, with higher incidences in middle aged men, and STEC, with children <5 years more affected (results not shown). The total estimated multiplier to correct for underreporting was lower for Salmonella spp. (7.7; 95% UI 3.7–18.1), and highest for STEC (19.7; 95% confidence interval [CI] 6.0–105.2), whereas for Campylobacter and Y. enterocolitica, the estimations were similar [11.0 (95% CI 6.0–23.8) and 10.9 (95% CI 6.0–23.3), respectively].
Reported and Estimated Total Cases and Deaths, Years of Life Lived With Disability, Years of Life Lost, and Disability-Adjusted Life Years Caused by Seven Pathogens in Denmark, 2017
DALY, disability-adjusted life year; STEC, Shiga toxin–producing Escherichia coli.
Disability-adjusted life years
Campylobacter caused the highest burden of disease (1709 DALYs), followed by Salmonella (492 DALYs) and norovirus (485 DALYs) (Table 2). Listeriosis caused 196 DALYs, the majority (95%) caused by YLL due to mortality (186 YLL). Despite the low number of cases, CT was responsible for the loss of 165 years of healthy life.
The contribution of health outcomes to the total disease burden varied between pathogens. Diarrhea was responsible for between 30% and 52% of total DALYs attributed to cases of infection by diarrheal agents; this contribution was lowest for Campylobacter and highest for STEC (Fig. 1). IBS was responsible for 26%, 19%, and 32% of total DALYs for Campylobacter, Salmonella, and Yersinia, respectively. Mortality (YLL) was responsible for 30–40% of DALYs for enteric pathogens, but explained a much higher proportion of the total disease burden of invasive infections: 70% of CT and 92% of listeriosis.
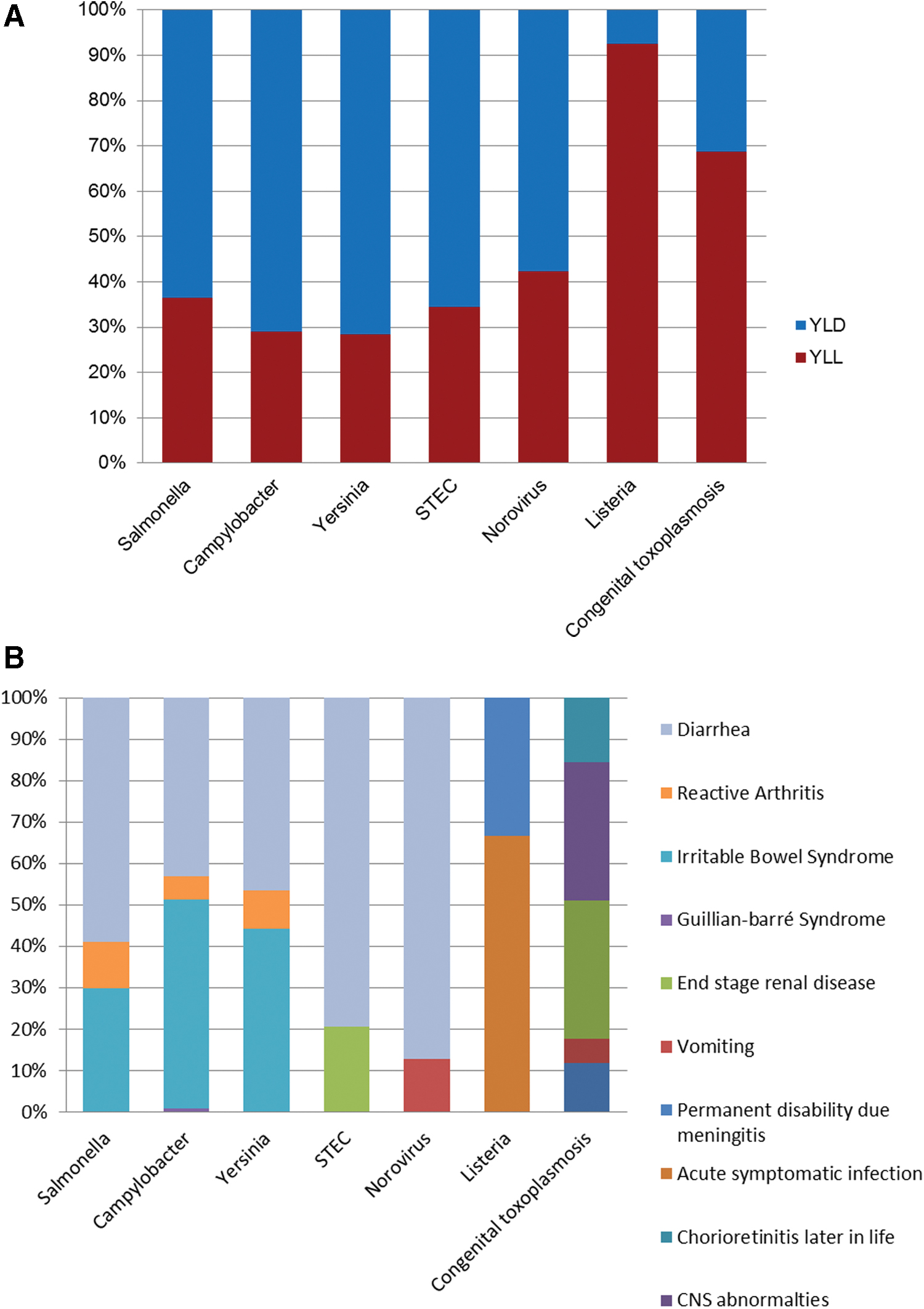
Figure 2 plots the burden of disease at population level (total DALYs) against the burden at individual level (DALYs per case, a measure for disease severity) for each pathogen. CT and listeriosis caused a high individual-level burden. Norovirus has a low individual-level burden, and a moderate population-level burden when compared with remaining hazards. Campylobacter caused the highest population burden, and a moderate individual-level disease burden. None of the seven infections caused both high individual and population-level burdens.
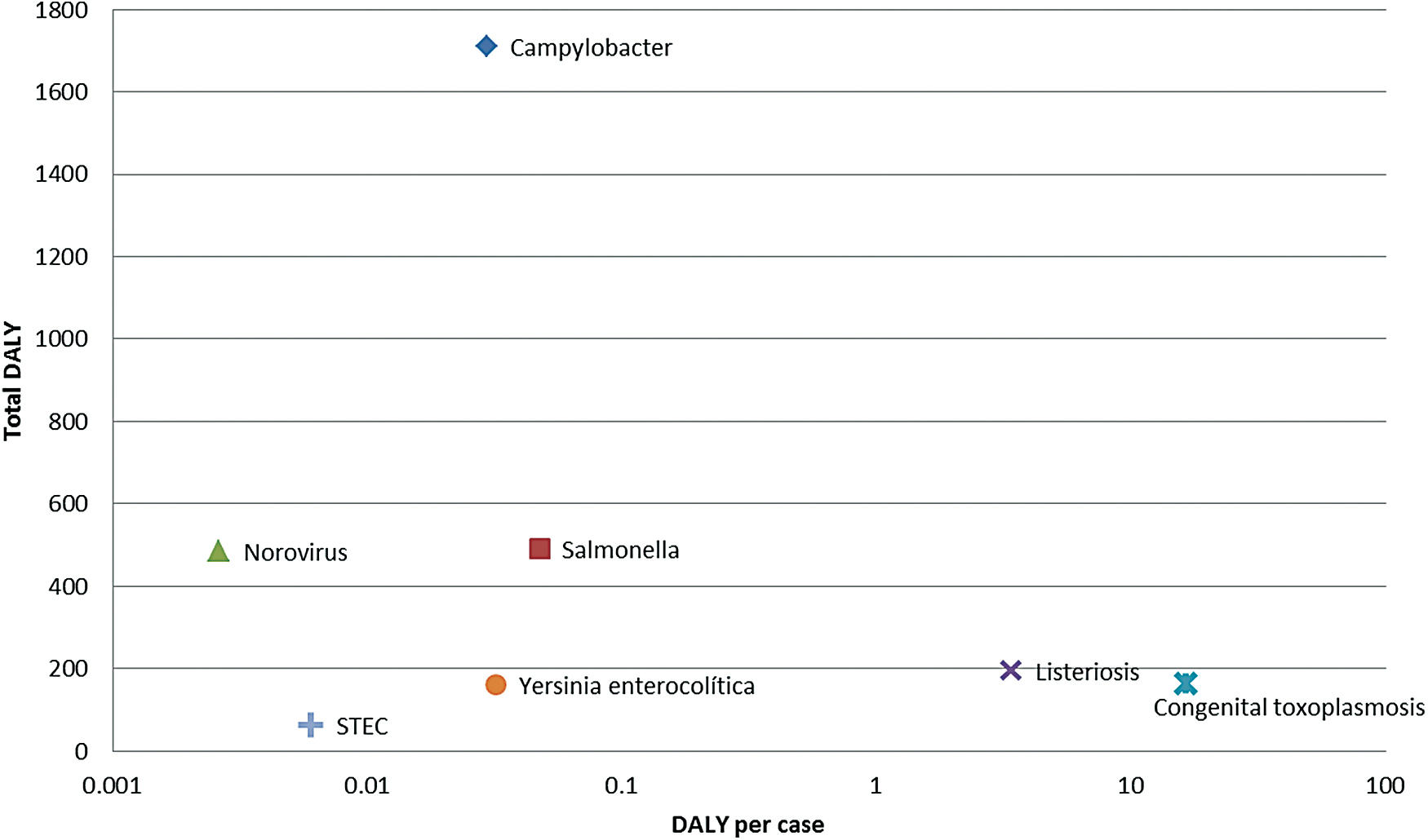
Plot of the burden of disease at the population level (total DALYs) and the burden of disease at individual level (DALYs per case) for seven infectious pathogens commonly transmitted through foods in 2017, Denmark. DALY, disability-adjusted life year. Color images are available online.
Foodborne DALYs
When multiplying total mean DALYs with the estimated foodborne attribution proportions for each, we found that Campylobacter caused the highest foodborne burden (1299 DALYs), followed by Salmonella (374 DALYs) and Listeria (196 DALYs) (Table 2). Two pathogens (Listeria and Yersinia) were assumed to be 100% foodborne. In contrast, with a foodborne attribution proportion of 18%, the foodborne burden of norovirus infections was 86 DALYs, which represented a marked decrease in the ranking of diseases (from third to sixth).
Discussion
We ranked seven pathogens commonly transmitted through foods in Denmark on the basis of their public health impact. Our estimates show that Campylobacter caused the highest FBD burden, leading to a total burden of 1709 DALYs, more than threefold higher than the second highest ranked pathogen (Salmonella). With an estimated 76% of all cases attributed to consumption of contaminated foods, Campylobacter still led the ranking when excluding DALYs that are due to other routes of exposure, such as environmental or person-to-person transmission. Focusing on the FBD burden, Salmonella ranked second, followed by Listeria and Yersinia. Foodborne CT was estimated to lead to the loss of ∼100 years of healthy life, a burden that was borne by a low number of cases in the population.
Campylobacter and Salmonella lead the ranking in both burden of disease and estimated incidence. All cases of campylobacteriosis and salmonellosis had diarrhea (the health outcome that defined an incident case), but because diarrhea is mostly mild and of short duration, it only explained ∼35% of the total burden for these infections. Sequelae such as IBS and ReA lead to a substantial fraction of healthy YLL, because they are long-lasting severe conditions. Even though norovirus had the highest estimated incidence, the disease burden that can be attributed to contaminated foods was low because severity and duration of disease are low, and because a small fraction of cases are caused by ingestion of contaminated foods (human-to-human transmission playing a major role; Hald et al., 2016). Some diseases with low incidence in the population, specifically listeriosis and CT, caused a substantial disease burden because health outcomes are very severe and/or mortality is high. Still, the interpretation of such burden estimates differs: the larger contribution of the DALYs of Listeria infections is due to the YLL, although most deaths occur in older age groups. In contrast, although 70% of the DALYs of CT are due to mortality, deaths occur in newborns or unborn babies (i.e., neonatal or fetal losses); this means that one single case will lead to a high number of years of life loss (equivalent to the life expectancy). In addition, the remaining 30% of the burden is explained by few cases living permanently with a disease with high disability (e.g., compromised vision or neurological disease).
Our estimates demonstrate a large and variable degree of underreporting of the different pathogens. Notably, the pathogen with the largest degree of underreporting and underdiagnosis (i.e., with the largest difference between reported and estimated total cases) was STEC, for which a multiplier of ∼19 was estimated (compared with 7 for Salmonella, 11 for Campylobacter, and 11 for Yersinia). The larger degree of underreporting is linked with the likelihood of samples being tested for these pathogens. Even though the symptoms of mild uncomplicated disease by all these three pathogens may be similar, physicians and laboratories are more likely to request testing for Salmonella and Campylobacter, while other infections often go undiagnosed in the population. For STEC, the likelihood of it being included in the panel of agents for laboratory analysis has been increasing in Denmark in recent years (Espenhain, 2013), which should be reflected in a corresponding decrease in underreporting. Because the data available to estimate underreporting of foodborne pathogens was somewhat dated (Müller et al., 2012), our underreporting factor for STEC is likely to be an overestimate.
The data used to correct the reported incidence for underascertainment, underreporting, and underdiagnosis were collected in a survey of a representative sample of the population that evaluated incidence and care-seeking behavior of cases of gastroenteritis in Denmark (Müller et al., 2012). Other studies conducted in different countries estimated multipliers to correct for underreporting and underdiagnosis of FBDs using different methodologies (Kubota et al., 2011; Scallan et al., 2011; Haagsma et al., 2012; Tam et al., 2012). Estimates vary substantially, which may reflect differences in health-seeking practices, public health care, and surveillance systems, in data availability and study methodologies. Using EU-wide data and data on disease risk in Swedish travelers, Havelaar et al. (2013) estimated lower underreporting correction factors for Campylobacter and Salmonella infections in Denmark (4.1 and 4.4, respectively). Our estimates were derived from a country-specific cross-sectional study designed to estimate national incidence of disease, and thus are more robust. Nevertheless, our surveillance pyramid model has a number of limitations, mostly linked to model assumptions and uncertainties in underlying data. We made a number of assumptions, including that the degree of underreporting was the same for all age groups; participants of the population survey that reported duration of symptoms >2 days had bacterial infections and thus their care-seeking behavior data could be used to estimate underreporting of the enteric pathogens included in this study; the likelihood of having a stool sample subjected to laboratory analysis was higher for hospitalized patients; the probability of a positive laboratory test being reported to national public health surveillance was the same for all cases, regardless of severity. All these may have led to under- or overestimation of underreporting of enteric pathogens. Other limitations of the approach have been discussed by Haagsma et al. (2012).
We identified health outcomes and sequelae of the seven pathogens through literature reviews. Other burdens of disease studies have included health outcomes that we have chosen not to include, for example, irritable bowel disease (IBD) as a sequelae of Salmonella and Campylobacter infections (Havelaar et al., 2012). Contesting previous evidence, Jess et al. (2011) showed that the estimated increased risk of IBD after infection with Salmonella or Campylobacter may be due to detection bias related to repeated stool testing in patients with unclear gastrointestinal symptoms rather than etiology, suggesting that risk estimates derived for this and other health outcomes may be overestimated (Jess et al., 2011). Other recent studies have also excluded IBD from their health outcome trees (Van Lier et al., 2016; de Noordhout et al., 2017).
As a composite health measure, DALY provides a comprehensive overview of the impact of diseases as it encompasses the relative disabilities and mortality, sustained both during the acute phase and related to the short- and long-term complications of diseases (Cassini et al., 2016). The recent World Health Organization's Global Burden of Foodborne Disease Project estimated DALYs for FBDs at global and regional level (WHO, 2015). This initiative was crucial for raising awareness on the importance of FBDs globally and showed substantial variation in the overall burden and most important diseases in different regions (Havelaar et al., 2015). It also showed that global and regional studies face substantial methodological and data challenges, particularly because they need to secure data harmonization, which often leads to a simplification of approaches and data. National burden of disease studies is crucial to address these limitations and inform disease-prevention strategies at country level (Lake et al., 2015).
Norovirus was responsible for the highest disease incidence. Even if only one in every five cases is estimated to be due to foodborne transmission, norovirus is recognized as one of the most important causes of FBD worldwide.
Reducing the burden of FBD depends upon informed risk management decisions and effective intervention strategies that are focused on the most important food safety problems. By ranking FBDs at a national level by accounting for underreporting of cases, total incidence, mortality, and severity of diseases in the population, we provide evidence on the priority causative agents. To be able to define and prioritize interventions, the next step is to identify the most important sources and transmission routes (Pires et al., 2009). Foodborne hazards are transmitted through a variety of foods and exposure pathways. Although naturally all hazards classified as foodborne can be transmitted through consumption of foods, many can also be transmitted through other transmission routes (e.g., contaminated environment, such as water, or direct contact with animals; Hald et al., 2016). An integrated food safety approach to reduce the burden of FBDs requires identifying the most important causative agents, and the most important causative sources of each disease (Havelaar et al., 2007a). Source attribution estimates have been used to guide interventions to control salmonellosis in several countries, including Denmark (Wegener, 2010). Ongoing and future efforts focusing on other pathogens are likely to lead to similar effects.
Burden of disease is a valid and robust method to compare the relative health impacts of diseases. Combining with economic analysis allows for identification of the FBD with highest health and economic impact in society (Christensen and Dejgård, 2017). We showed that Campylobacter caused the highest public health impact among all FBDs in Denmark, even though it was surpassed by norovirus in terms of total estimated cases. Campylobacter has been the most reported FBD in Denmark in the past decades (Anonymous, 2018), and it is also the most reported FBD in Europe and globally. It has also been estimated to cause the highest economic impact among FBDs in Denmark when accounting for the cost of illness (i.e., considering direct and indirect health care costs, and costs due to absence of work (Christensen and Dejgård, 2017). These indicate that Campylobacter should be prioritized in mitigation efforts to reduce the FBD burden. However, such a prioritization should not be at the expense of extensive and effective control programs already in place for Salmonella and L. monocytogenes, which are paramount to maintain low prevalence in the food chain.
Broiler chickens have been recognized as the most important source of Campylobacter infections in Denmark, and a number of initiatives to reduce Campylobacter prevalence in broilers have been attempted (Rosenquist et al., 2009; Boysen et al., 2013). However, these interventions have not had the desired effect in terms of reduction of the public health burden of campylobacteriosis in the population. The lack of public health effect may be related to other factors counterbalancing the effect of the implemented interventions, particularly with the role of other sources of exposure. This highlights the need for identifying the relative contribution of all potential sources of a pathogen to prioritize food safety intervention strategies.
The calculations of benefits and setting priorities in control and prevention of human disease are complicated by the cross-sectoral nature of foodborne zoonosis management, with consequences appearing in public health but investments needed in prevention in the food producing sector (Wilson, 2013). As an example, controlling Salmonella in the pig sector includes high biosecurity in pig herds and sensible animal movement patterns between farms. These interventions will not only reduce the risk of foodborne salmonellosis, but will also have other benefits for the pig sector, the animal health sector, food safety, and food security, and may eventually be more economically beneficial for the food industry than, for example, controlling Campylobacter at poultry slaughter houses, if nondirect benefits are included.
Since return for public money is not only measured in rational scientific and economic criteria, but also includes more intangible and unmeasurable benefits, our analysis may not provide the full answer in prioritization prevention of FBDs (Brookes, 2015). However, our study has provided clear scientific evidence that Campylobacter results in the biggest FBD burden in Denmark today, and that efforts to prevent exposure to other pathogens through foods should be maintained or reinforced. Our burden of disease estimates can be updated periodically and provide a steppingstone from which policy analysis can be made to support decision-making.
Footnotes
Acknowledgments
We are thankful for the input of Flemming Scheutz, Aron Hall, and Brecht Devleesschauwer throughout the project. We also thank Sofie T. Thomsen for a critical read of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by the Danish Ministry of Environment and Food through the Metrix project.