
Abstract
In this study, the prevalence and antimicrobial resistance of enterotoxigenic Escherichia coli (ETEC) and enteropathogenic Escherichia coli (EPEC) were investigated. Altogether 100 stool samples were collected from diarrheal patients attending the Sheikh Hasina Medical College and Hospital, Tangail, Bangladesh, during the period from March 1 to May 30, 2018. In vivo pathogenic potential of ETEC and EPEC using a Caenorhabditis elegans infection model was investigated. Among 100 diarrheal patients, 31% were positive for both ETEC and EPEC strains, 23% were lt positive for ETEC strains, and 8% were bfpA positive for EPEC strains. It was detected that 82.60%, 65.21%, 73.91%, 78.26%, 47.82%, 60.86%, and 47.82% of ETEC strains were resistant to amoxicillin–clavulanic acid (AMC), tetracycline (TE), nalidixic acid (NA), azithromycin, ciprofloxacin, ampicillin (AMP), and erythromycin (E), respectively. Whereas it was detected that 87.5% strains were resistant to AMC, AMP, and E, 75% were resistant to TE and NA, respectively. Both strains developed multidrug resistance to commonly prescribed antibiotics. EPEC showed higher pathogenicity than ETEC as 67.75% and 60% of C. elegans died after 18 h postinfection with EPEC and ETEC, respectively. The high rate of antimicrobial resistance of EPEC and ETEC highlights the necessity for the prudent use of antimicrobials in Bangladesh.
Introduction
Diarrhea is one of the most common health problems, especially in developing countries such as Bangladesh. Around 2 billion diarrheal diseases occur each year worldwide and are responsible for killing around 1.9 million children aged below 5 years. The occurrence rate of diarrheal disease is higher in the developing country due to unimproved sanitation, inadequate hygiene, and poor drinking water access, as well as poorer overall health and nutritional status (United Nations Report of the Secretary-General, 2017). Diarrhea is characterized by an abnormally frequent flow of loose or watery stools that lead to dehydration. The major causative agents of diarrhea are Escherichia coli, Vibrio cholerae, Campylobacter spp., Shigella spp., Clostridium difficile, rotavirus, and norovirus or parasites, for example, Giardia and Entamoeba histolytica. Among these, E. coli is the most common and frequently observed causative agent of diarrhea ([GBD] Diarrhoeal Diseases Collaborators, 2017).
There are two types of E. coli strains, pathogenic and nonpathogenic. There are five major groups of pathogenic E. coli strains, which are (i) enterotoxigenic E. coli (ETEC) that causes infantile and traveler's diarrhea; (ii) enteropathogenic E. coli (EPEC) that causes infant diarrhea; (iii) enteroaggregative E. coli that is associated with watery diarrhea, but it can be accompanied with blood or mucus and cause persistent diarrhea; (iv) enteroinvasive E. coli that causes dysentery; and (v) enterohemorrhagic E. coli that causes hemorrhagic colitis and the hemolytic–uremic syndrome (Jafari et al., 2012). These different clinical manifestations are related to the presence of virulence genes in plasmids and in defined groups of genes, called pathogenic islands, present in the chromosomes of these bacteria. The proteins coded by these genes allow the bacteria to interact with the cells in the intestinal mucosa and disrupt normal functions with the consequent expression of clinical symptoms (Gilligan et al., 1999).
E. coli is the cause of diarrhea not only in developing countries but also in developed countries. Diarrheagenic E. coli (DEC) has been reported to be responsible for 34% of diarrheal episodes in Bangladesh (ICDDR, B, 2002). Normally, in the hospital, diarrheal patients use a different type of random antibiotic (nonspecific). The emergence of antibiotic-resistant bacteria limits the clinical use of antibiotics, and there is an increasing concern that the existing antibiotics will become ineffective against pathogens and more expensive (Sommer et al., 2017). Several findings suggest that inappropriate selection and abuse of antibiotics may lead to resistance in various bacteria and make the treatment of bacterial infections more difficult (Kolár et al., 2001). Globally, antibiotic resistance in E. coli has been reported. E. coli infection treatment has gradually become more intricate by the emergence of resistance to most first-line antibiotics (Sabaté et al., 2008).
Inappropriate antibiotic use and limited laboratory facilities for testing antibiotic susceptibility have led to increased resistance for bacteria and reduced therapeutic efficacy in developing countries (Roma et al., 2000). Hence, this study aimed to determine the prevalence, antimicrobial resistance pattern, and pathogenicity of two most important pathogenic E. coli strains (ETEC and EPEC) isolated from diarrheal patients attending the Sheikh Hasina Medical College and Hospital, Tangail, Bangladesh.
Materials and Methods
Specimen collection and cultural identification
One hundred stool samples were collected aseptically in a clean, leakproof wide-mouth container from diarrheal patients attending the Sheikh Hasina Medical College and Hospital from March 1 to May 30, 2018. The sample size represented almost 10% of the population visiting the hospital during this time period. We were trying to collect similar proportions of male and female samples. The aims of the research and benefits of participation were clearly explained to the participants before data collection. Participation of the patient was on a voluntary basis and it was their right to withdraw from the study at any time in the course of the study.
Stool samples were directly inoculated into tryptic soy broth with 0.3% yeast extract and incubated at 37°C for 18–20 h. After overnight incubation, enriched stool samples were streaked on MacConkey agar plates, and the enriched stool samples were stored in a −20°C refrigerator after addition of 15% glycerol for future use. The ability to ferment lactose gives an option to use MacConkey agar to discriminate E. coli from other nonlactose-fermenting coliforms. Medium-sized, round pink colonies on MacConkey agar are picked as E. coli suspect colonies (Lupindu, 2017). After overnight incubation on the MacConkey agar plate, a single, lactose-fermenting, E. coli cell colony was picked for further characterization.
Polymerase chain reaction assay for detection of EPEC and ETEC strains
The template DNA was made from the lactose-fermenting colony that was picked up from the MacConkey agar plate. The single colony was dissolved in 20 μL of sterile water and boiled for 5 min to make the DNA template for polymerase chain reaction (PCR). For molecular detection of EPEC and ETEC, the PCR was carried out in a 25-μL reaction volume with 12.5 μL of 2 × Go Taq® G2 Green Master Mix (Promega), forward and reverse primers at 50 μM final concentration, 50 ng DNA template, and nuclease-free water in a microcentrifuge tube.
The primers used for detection of virulence genes of lt of ETEC are 5′-CACACGGAGCTCCTCAGTC-3′ (F) and 5′-CCCCCAGCCTAGCTTAGTTT-3′ (R) with the gene product size of 508 bp. For detection of virulence genes of bfpA of EPEC, primers used are 5′-GGAAGTCAAATTCATGGGGGTAT-3′ (F) and 5′-GGAATCAGACGCAGACTGGTAGT-3′ (R) with the gene product size of 300 bp. The following thermocycler conditions were used for the PCR: 96°C for 4 min, followed by 35 cycles at 95°C for 20 s, 65°C for 20 s for the ETEC strain (or at 59°C for 20 s for the EPEC strain), and 72°C for 1 min.
Biochemical characterization
The biochemical reactions of all of the positive colonies from molecular detection were performed using standard methods described in the manual for laboratory investigation of acute enteric infections (WHO, 1987). For biochemical characterization of E. coli, the following biochemical tests were performed: Kligler's iron agar (KIA) test, motility indole urea (MIU) test, and Simmons citrate agar test.
Antimicrobial susceptibility testing
Bacterial susceptibility test to antimicrobial agents was performed using the Kirby–Bauer method (Bauer et al., 1966) on Mueller-Hinton agar by the Clinical and Laboratory Standards Institute (CLSI) with commercial antimicrobial discs (Oxoid, Basingstoke, United Kingdom). The antibiotic discs used in this study were ampicillin (AMP; 10 μg), amoxicillin–clavulanic acid (AMC; 10 μg), nalidixic acid (NA; 30 μg), erythromycin (E; 30 μg), tetracycline (TE; 30 μg), ciprofloxacin (CIP; 5 μg), and azithromycin (AZM; 15 μg).
The detected E. coli isolates were inoculated in Mueller-Hinton broth and incubated at 37°C for 5 h. The broth was diluted in normal saline solution to a density of 0.5 McFarland turbidity standards. Cotton swabs were used for streaking the diluted broth onto Mueller-Hinton agar plates. After air drying, antibiotic discs were placed 30 mm apart and 10 mm away from the edge of the plate. Plates were inverted and incubated aerobically at 37°C for 16–18 h. The zone of inhibition and resistance was measured, recorded, and interpreted according to the recommendations of the CLSI (2017).
Caenorhabditis elegans survival assay
Caenorhabditis elegans survival assays were performed as previously described (Tan et al., 1999) with minor modifications. ETEC and EPEC isolates and E. coli OP50 were grown overnight in 1 mL of brain-heart infusion (BHI) broth and LB broth, respectively, at 37°C. Ten milliliters of the overnight culture was spread over a small area on 3.5-cm nematode growth medium (NGM, NaCl [50 mM], peptone [0.25%], agar [1.7%], CaCl2 [1 mM], cholesterol [5 μg/mL], KH2PO4 (25 mM), and MgSO4 [1 mM]) plates and incubated at 37°C for 24 h. Plates were then allowed to equilibrate to room temperature for 12–24 h before use. Twenty age-matched Glp worms (glp-4; sek-1) (gift from Peter R. Boag, Monash University, Australia) were transferred to NGM plates seeded with individual EPEC and ETEC isolates and incubated at 25°C. The number of live and dead worms was scored at 18-h intervals. As a negative control, EPEC/ETEC was replaced with E. coli OP50. Three independent experiments were performed for each isolate.
Results
Prevalence of EPEC and ETEC is determined by PCR
A total of 100 stool samples of diarrheal patients were examined to detect the presence of ETEC and EPEC strains of the E. coli pathotype by PCR; the lt gene for ETEC and bfpA gene for EPEC were screened. Among these 100 samples, 31 (95% confidence interval: 23–41) were positive for ETEC or EPEC (Fig. 1). Of these, 23 (95% confidence interval: 16–32) and 8 (95% confidence interval: 4–15) were positive for ETEC and EPEC, respectively. The prevalence rates of ETEC and EPEC were 23% and 8%, respectively.
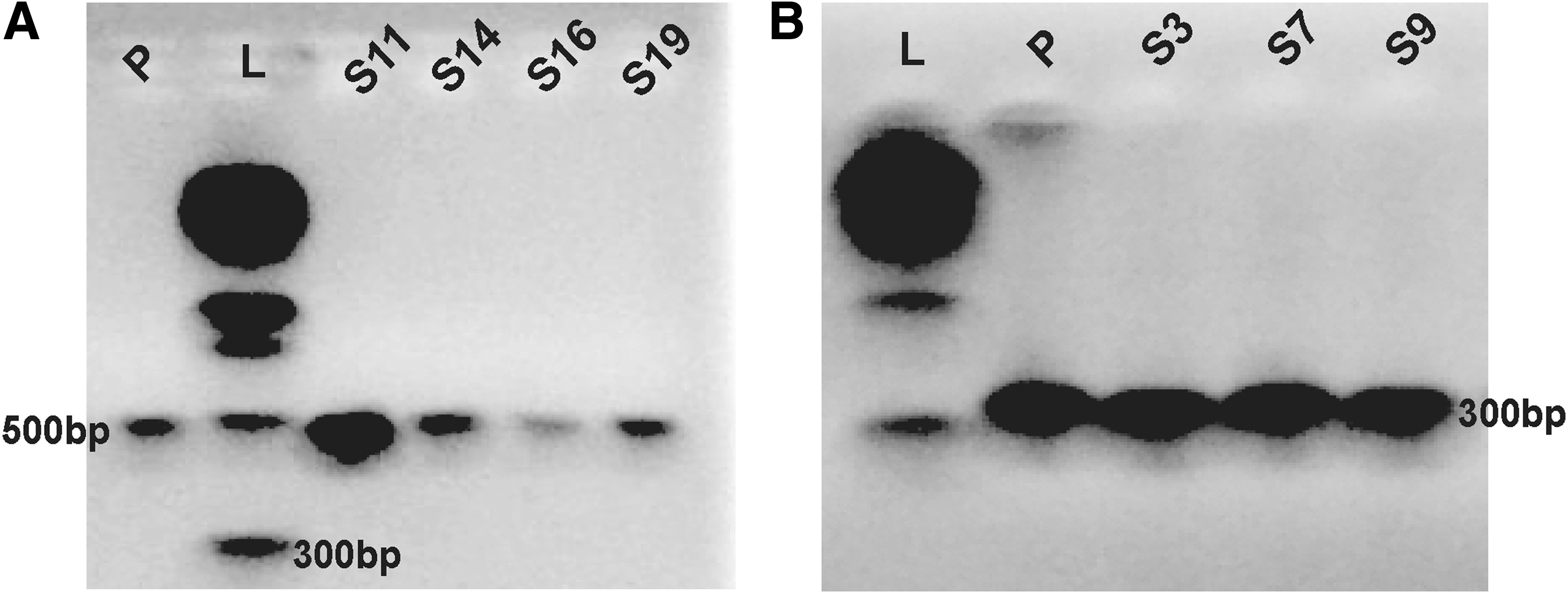
Representative picture of gel electrophoresis of the PCR product to detect ETEC and EPEC.
Biochemical characteristics of the identified diarrheagenic E. coli
Of 100 samples, 31 were detected as pathogenic E. coli strains, which were ETEC and EPEC, by PCR. It was found that all the 31 strains fermented mannitol and utilized sucrose and lactose in KIA. They were also motile and indole positive, but urease negative in MIU agar. They showed a negative result for the citrate utilization test. The representative biochemical results of one of the positive samples are shown in Supplementary Figure S1.
Antibiotic resistance patterns of the isolated EPEC and ETEC
The antibiogram results showed that most of the ETEC and EPEC strains were multidrug resistant (resistance to more than one drug) (Supplementary Table S1). Of 31 isolates, 83.87% were resistant to AMC, 67.74% to TE and AMP, 74.19% to NA, 67.74% to AZM, 38.70% to CIP, and 58.06% to E (Table 1).
Antibiotic Resistance of Bacterial Isolates (n = 31) to Individual Drugs
AMC, amoxicillin–clavulanic acid; TE, tetracycline; NA, nalidixic acid; AZM, azithromycin; CIP, ciprofloxacin; AM, ampicillin; E, erythromycin.
In the present study, 82.60% of detected ETEC were resistant to AMC, 65.21% to TE, 73.91% to NA, 78.26% to AZM, and 47.82% to E and CIP (Table 2). Only 30.43% of detected ETEC were shown to be sensitive to tetracycline. On the other hand, 87.5% of detected EPEC were resistant to AMC, 75% to TE and NA, and 87.5% to AMP and E and showed no sensitivity to those antibiotics. Only 50% of detected EPEC showed sensitivity to AZM. Detected EPEC strains were shown to have a lower resistance rate to CIP and AZM (Table 3).
Antibiogram Profile of Enterotoxigenic Escherichia coli Isolates (n = 23) to Individual Drugs
AMC, amoxicillin–clavulanic acid; TE, tetracycline; NA, nalidixic acid; AZM, azithromycin; CIP, ciprofloxacin; AM, ampicillin; E, erythromycin.
Antibiogram Profile of Enteropathogenic Escherichia coli Isolates (n = 8) to Individual Drugs
AMC, amoxicillin–clavulanic acid; TE, tetracycline; NA, nalidixic acid; AZM, azithromycin; CIP, ciprofloxacin; AM, ampicillin E, erythromycin.
Pathogenic potential of identified ETEC and EPEC
Pathogenicity of ETEC and EPEC was studied by solid agar infection assay. There was a significant statistical difference (p < 0.05) in the survival of C. elegans when challenged with ETEC and EPEC in comparison with E. coli OP50 control. After 18 h postinfection with ETEC and EPEC, the percentage of live infected C. elegans was 40% and 32.25%, respectively, which are comparatively close to a positive control (reference strains of ETEC and EPEC). This result indicates that infected C. elegans were killed due to their infection of ETEC and EPEC strains (Fig. 2). All the detailed results are presented in Supplementary Table S2. There was no significant statistical difference (p < 0.05) between the killing rate of C. elegans when challenged with EPEC and ETEC. However, the killing rate of C. elegans by EPEC is higher than ETEC as 68% and 60% of the C. elegans were killed when challenged with EPEC and ETEC, respectively.
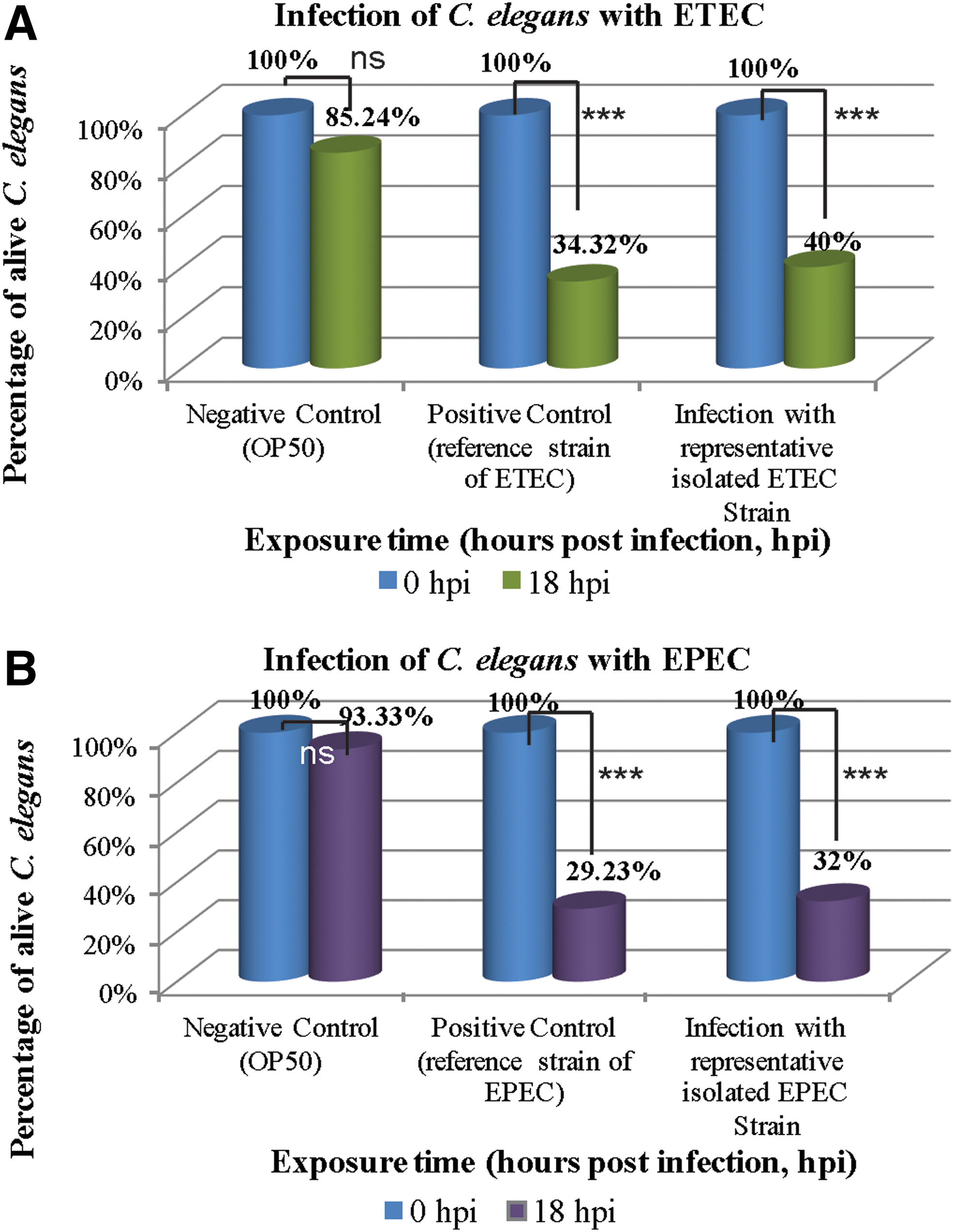
Infection of Caenorhabditis elegans with ETEC and EPEC.
Discussion
Diarrheagenic ETEC (23%) was the most prevalent strain in the study population. In 2002, it was reported that DEC was responsible for 34% of diarrheal diseases in Bangladesh (ICDDR, B, 2002). DEC was associated with 30% of diarrheal diseases in Bangladesh (Albert et al., 1999). ETEC and EPEC were commonly identified throughout the years (Azmuda et al., 2019). Previously, it was found that ETEC is the cause of 90% of infant diarrhea cases in Bangladesh (Qadri et al., 2005). It was also reported that ETEC was the most prevalent pathotype, followed by EPEC, in surface waters in Bangladesh (Akter et al., 2013). All the above study findings were quite similar to present study findings where the prevalence of ETEC was 23%, followed by EPEC (8%). In Bangladesh, a high prevalence of diarrheal diseases especially in children <5 years of age was reported due to the fecal contamination of surface water (Chowdhury et al., 2015).
Similar studies with acute diarrhea were performed in different parts of the world. In Japan, different types of DEC were the most frequently identified enteropathogens (Toma et al., 2003). In Iran and Finland, it has been reported that ETEC was associated with 10% and 11% of diarrheal diseases, respectively (Arif et al., 2010; Antikainen et al., 2013). Moreover, in Thailand and Vietnam, ETEC was associated with 5.8% and 4% of diarrheal diseases, respectively (Nguyen et al., 2005; Hien et al., 2008), which are much lower than our present study findings (23%). This might be due to important regional differences in the prevalence of different categories of DEC (Albert et al., 1995). Therefore, our findings revealed that the prevalence of ETEC is much higher in Bangladesh compared with other countries. However, this study has potential limitations regarding the prevalence of EPEC. EPEC isolates are classified as typical (eaeA+ bfpA+) or atypical (eaeA+ bfpA−). After detecting the gene bfpA, we actually detected only the typical EPEC. Therefore, there is a possibility to miss some atypical EPEC strains.
Nowadays, antibiotic resistance of bacteria is a very alarming issue worldwide as the multidrug-resistant bacteria have been observed with increasing frequency, and new antibiotic discovery is not as rapid as resistance development of bacteria. The Food and Drug Administration (2013) and many other international organizations have openly admitted that there is an antibiotic crisis. There are many dangerous species of Gram-positive and Gram-negative bacteria, including Staphylococcus aureus, Streptococcus pneumoniae, Clostridium difficile, E. coli, and Klebsiella pneumoniae, due to their most alarming resistance to antibiotics, namely methicillin, vancomycin, and penicillin (Richard and Yitzhak, 2014). E. coli is one of the Enterobacteriaceae family that is generally susceptible to most of the antibiotics, but recently, they have been found to be highly resistant to the most widely used antibiotics due to horizontal gene transfer (Livermore et al., 2008). Our present study reveals that the DEC (ETEC and EPEC) attain high resistance to most of the commonly used antibiotics. Only 30.43% of detected ETEC and 50% EPEC were shown to be sensitive to tetracycline and AZM, respectively. The ETEC and EPEC with resistance to all other commonly used antibiotics, including AMP, AMC, NA, E, and CIP, were observed. This is very alarming and worrying because humans are most commonly infected with these Gram-negative bacteria. Now, we need to be aware of the use of antibiotics and their misuse, especially in developing countries such as Bangladesh, to prevent the frequent increase of antibiotic resistance and allocate more funds to establish R&D to discover and develop new antibiotics. Otherwise, the day will not be far when we will enter an era similar to that before the discovery of penicillin and people will die just because of a simple bacterial infection.
C. elegans was used to observe the pathogenicity of ETEC and EPEC strains of DEC as it is an ideal model for host–pathogen interaction studies and screening of new drugs and antibiotics. EPEC showed more pathogenicity than ETEC as 68% and 60% of the C. elegans were killed when challenged with EPEC and ETEC, respectively. In the future, it is likely that C. elegans will be increasingly used to dissect the virulence of a pathogen, to untangle the molecular mechanisms of resistance and susceptibility to disease, and ultimately to find leads for antimicrobial drug discovery.
Conclusion
This study highlights the prevalence of ETEC and EPEC among diarrheal patients and their antibiotic resistance patterns. The most significant finding of this study is that ETEC is more prevalent among diarrheal patients. The ETEC and EPEC are resistant to most of the frequently used antibiotics, including combinational AMC. Therefore, the history of pre-exposed antibiotics should be considered during antibiotic therapies to prevent the development of antibiotic resistance. Further investigations are needed for the prevalence rates of other strains of DEC among diarrheal patients and understanding the molecular mechanisms of their multidrug resistance.
Ethical Approval for Participation
The study was approved by the ethics review committee of the Department of Biotechnology and Genetic Engineering (BGE) of Mawlana Bhashani Science and Technology University (MBSTU), Bangladesh. The committee consists of the Chairman, BGE, and the two senior-most Professors (Dr. AKM Mohiuddin and Dr. Md Imam Hossain). Permissions were obtained from the concerned bodies of the Hospital. All underage participants had their written informed consent provided by their parent or legal guardian. Information acquired in each course of the study was kept confidential.
Footnotes
Acknowledgments
The authors are grateful to the participants who agreed to provide their stool samples for this study. The authors would like to thank Md Shahin Mahmud for his criticism during the study and are also very grateful to Dr. Peter R Boag, Monash University, Australia, for his gift of the C. elegans strain.
Disclosure Statement
No competing financial interests exist.
Author Contributions
M.M.R., P.A., A.K., and N.S. designed and performed the experiments and analyzed the data. M.M.R. and P.A. wrote the manuscript with input from all authors. A.Z.S. and F.T.Z. contributed to the interpretation of the results and the final version of the manuscript. All authors provided critical feedback and helped shape the research, analysis, and manuscript. M.M.R. supervised the project.
Funding Information
The authors acknowledge the Research Cell, Mawlana Bhashani Science and Technology University, Santosh, Tangail-1902, Bangladesh, for funding this research.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.