
Abstract
Urinary tract infections (UTIs) are common and may occur in foodborne Salmonella outbreaks. Using data from PulseNet, the U.S. national molecular subtyping network for foodborne disease surveillance, we analyzed the 9781 Salmonella isolates associated with the 110 outbreaks from 2004 to 2013 that included at least one urine isolate. Within each outbreak, we calculated standardized isolation dates, using these dates in a linear mixed model to estimate the difference in incubation period for infections yielding stool versus urine isolates. We estimate that the incubation period for Salmonella UTIs is on average 10.6 (95% confidence interval 6.0–15.2) days longer than for gastrointestinal illness, suggesting that outbreak investigators should interview UTI patients about a longer time period before illness onset to identify sources of infection.
Introduction
Urinary tract infections (UTIs) are among the most common infections, estimated to lead to >10.5 million ambulatory health care visits in the United States (Foxman, 2002; Mazzulli, 2002; Russo and Johnson, 2003; Schappert and Rechtsteiner, 2011). Most community-acquired UTIs are caused by Escherichia coli (Stamm, 2002). Several studies have linked E. coli UTIs to foodborne transmission (Manges et al., 2007; Vincent et al., 2010; Manges and Johnson, 2013; Norstrom et al., 2013); however, since E. coli is a normal part of the human intestinal flora, determining whether UTIs are foodborne is usually difficult. Salmonella, a less common cause of UTIs, does not belong to normal human intestinal flora. Investigation of urine isolates recovered during foodborne Salmonella outbreaks (Sivapalasingam et al., 2004) can shed light on foodborne UTIs.
We used information from 10 years of U.S. Salmonella outbreak investigations to describe the epidemiology and estimate the incubation period of foodborne UTIs. We also describe clinical features of UTIs during a 2012 Salmonella serotype Cubana outbreak that included a high proportion of UTIs.
Materials and Methods
PulseNet analysis of outbreak-associated Salmonella UTIs
We used data from 2004 through 2013 from PulseNet, the U.S. national molecular subtyping network for foodborne disease surveillance and the primary tool for identification of multistate Salmonella outbreaks (Mazzulli, 2002). During the study period, state health departments performed pulsed-field gel electrophoresis (PFGE) on all Salmonella isolates and submitted the results to PulseNet. The PulseNet database includes information on isolate source (stool, urine, blood, or other) and date and patient demographic characteristics (gender, age, and state). When a cluster was identified, state and local public health officials interviewed patients about foods and other exposures 0–7 days before illness onset to identify common exposures; for multistate outbreaks, Centers for Disease Control and Prevention (CDC) typically coordinated. CDC's database of outbreaks in which it was involved was queried to identify outbreaks (defined as clusters of two or more isolates with the same PFGE pattern reported within 60 days) with confirmed (defined by ≥2 of 3 lines of evidence: epidemiologic, laboratory, and product traceback) or suspected food vehicles.
We analyzed data on urine and stool isolates from all outbreaks in which at least one urine and one stool isolate were reported and the outbreak duration (time from first to last isolation date) was <1 year. We used chi-square tests to compare patients with urine versus stool isolates by age and gender, categorizing age as ≤45 and >45 years. We estimated incubation periods by assuming that, in the context of an outbreak, the timing of exposure for patients with urine isolates would not be systematically different from patients with stool isolates. Therefore, observed differences in mean isolation dates should reflect differences in incubation period. Within each outbreak, we calculated the mean isolation date for stool isolates, then subtracted the isolation date of each stool and urine isolate in the outbreak from this date to standardize isolation dates across outbreaks. We used a linear mixed model with random and fixed effects for source site (urine vs. stool) to estimate both the mean difference in timing of urine and stool isolates and outbreak-specific estimates of this difference. Model assumptions were checked using residual plots.
Clinical features of Salmonella UTIs in a foodborne outbreak
To examine whether outbreak-associated urine Salmonella isolates are associated with symptomatic UTIs (not an incidental “contaminant”), we surveyed patients with urine isolates reported in a 2012 Salmonella serotype Cubana outbreak associated with consumption of contaminated alfalfa sprouts. A CDC epidemiologist contacted these patients 1–6 months after the reported illness and used a standard questionnaire to ask about gastrointestinal and urologic symptoms in the 30 days before the Salmonella isolation date, medical care-seeking, diagnoses, and treatment. We report descriptive statistics for this outbreak.
Results
PulseNet analysis of outbreak-associated Salmonella UTIs
The PulseNet data set contained 110 Salmonella outbreaks meeting the inclusion criteria, with a median of 89 isolates (range: 3, 1040), duration of 118 days (range: 12, 361), and median percentage urine isolates at 4% (range: 1, 74). These 110 outbreaks included 9781 isolates with 8454 (86%) from stool, 566 (6%) from urine, and 761 (8%) from blood or other sources. Urine isolates had later mean isolation dates than stool isolates in 102 (91%) of the 110 outbreaks, with a mean difference of 10.6 days later (95% confidence interval: 6.0–15.2) (Fig. 1). Residual plots showed acceptable model fit. Urine isolates were more likely than stool isolates to be obtained from women (among isolates from patients for whom gender was reported, 88% [471/537] of urine isolates and 53% [4172/7848] of stool isolates were from women; p-value <0.0001) and from older persons (among isolates from patients for whom age was reported, 57% [307/542] of urine isolates and 32% [2532/7963] of stool isolates were obtained from persons ≥45 years; p-value <0.0001). Median age reported for stool isolates is 30 years (interquartile range [IQR]: 13, 50), and for urine is 50 years (IQR: 24, 69).
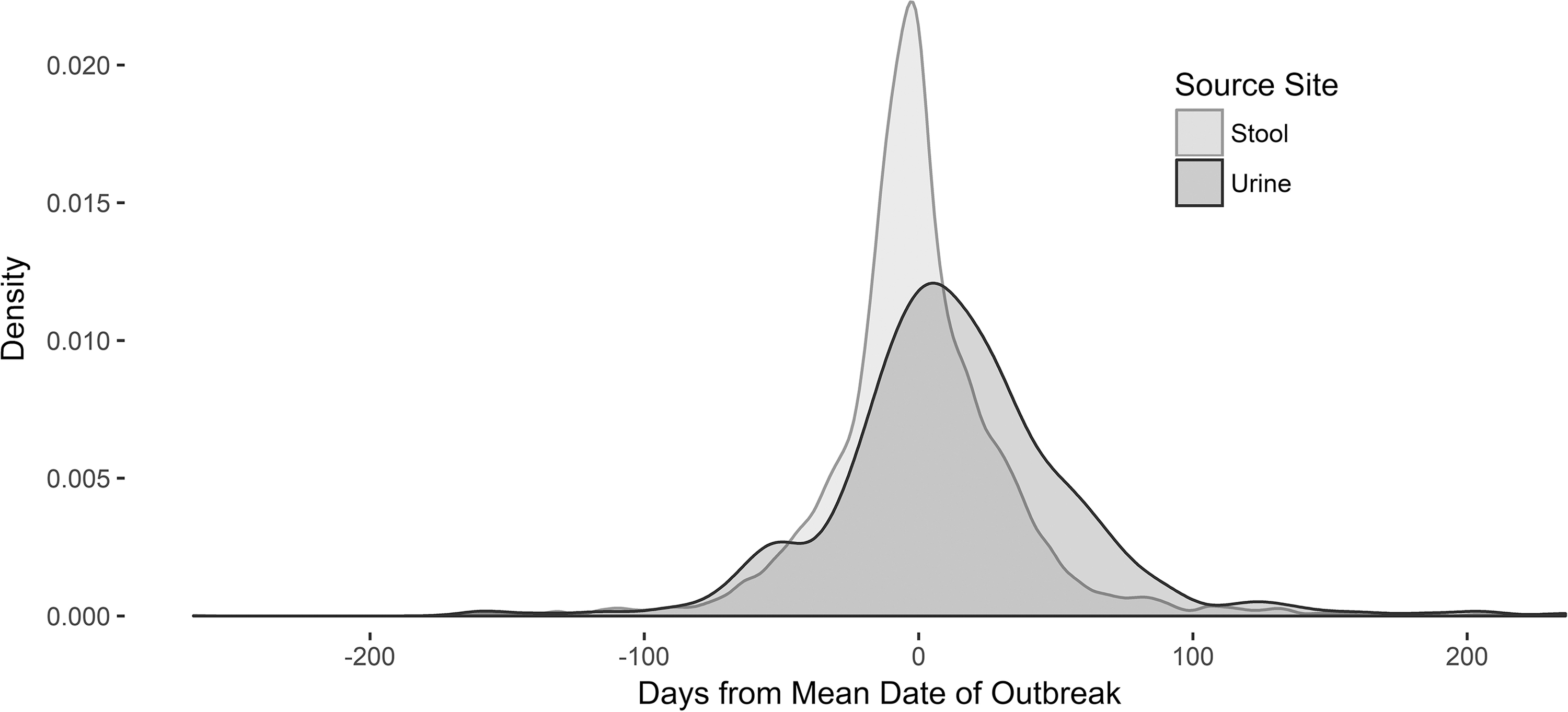
Timing of urine and stool isolates in 2004–2013 foodborne Salmonella outbreaks that included at least one urine and one stool isolate, with “0” representing the mean outbreak-specific stool isolation date, PulseNet.
Clinical features of Salmonella UTIs in a foodborne outbreak
Eleven patients in the Salmonella Cubana outbreak had urine isolates. Seven were reached for interview; six completed the questionnaire, and one reported on diagnosis and treatment only. All were women who were diagnosed with UTIs and treated with antibiotics; two reported kidney infection. Multiple signs and symptoms consistent with UTIs, most commonly urinary frequency (5/6), urgency (5/6), dysuria (4/6), and hematuria (4/5), were reported. Two of six patients reported diarrhea in the 30 days preceding UTI, but neither sought medical attention for diarrhea.
Discussion
Our analysis of UTIs occurring in 110 multistate Salmonella foodborne outbreaks for 10 years supports two conclusions that expand understanding of foodborne UTIs. First, the incubation period for urinary infections is on average about 10 days longer than for gastrointestinal infections. This finding suggests that, during outbreak investigations, epidemiologists should query patients with urine isolates about food exposures for a longer period before illness onset than patients with stool isolates, perhaps 14 days rather than the standard 7. Second, our small survey of patients with urinary isolates in a Salmonella Cubana outbreak indicates that, at least during this outbreak, these patients had symptomatic UTIs not necessarily associated with diarrhea. These urinary isolates were not incidental findings, and consumption of contaminated food was clearly an antecedent to these illnesses.
Our data do not explain why the incubation period for Salmonella foodborne UTIs is longer than for diarrheal disease. However, our observations are consistent with the hypothesis proposed by others (Norstrom et al., 2013) that more time may typically be required for the pathogen to be ingested, excreted, transferred to the urinary tract, and amplified to levels causing symptoms. Later median onset dates would also be observed if patients with urine isolates typically consumed contaminated foods later during outbreaks than patients with stool isolates, but this seems implausible. A more important limitation of our study is that we have information on urinary symptoms for only a small number of patients in a single outbreak. It is possible that sometimes urine isolates could represent specimen contamination rather than UTIs. Also, our estimates do not account for variables such as Salmonella serotype and patient gender, age, and time to care-seeking that may affect observed incubation periods.
Conclusions
Our findings regarding the incubation period of Salmonella UTIs in foodborne outbreaks add to a growing body of literature on foodborne transmission of pathogens causing UTIs (Manges et al., 2007; Vincent et al., 2010; Manges and Johnson, 2013; Norstrom et al., 2013). The high burden of UTIs suggests that this is an important area for further investigation of burden, pathogenesis, and prevention.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.