
Abstract
The objective of this systematic review and meta-analysis was to estimate the proportion of postinfectious reactive arthritis (ReA) after bacterial enteric infection from one of four selected pathogens. We collected studies from PubMed, Web of Science, and Embase, which assessed the proportion of postinfectious ReA published from January 1, 2000 to April 1, 2018. Papers were screened independently by title, abstract, and full text; papers in English, Spanish, and Portuguese utilizing a case–control (CC) or cohort study design, with a laboratory confirmed or probable acute bacterial enteric infection and subsequent ReA, were included. The proportion of ReA cases was pooled between and across pathogens. Factors that can induce study heterogeneity were explored using univariate meta-regression, including region, sample size, study design, and ReA case ascertainment. Twenty-four articles were included in the final review. The estimated percentage of cases across studies describing Campylobacter-associated ReA (n = 11) was 1.71 (95% confidence interval [CI] 0.49–5.84%); Salmonella (n = 17) was 3.9 (95% CI 1.6–9.1%); Shigella (n = 6) was 1.0 (95% CI 0.2–4.9%); and Yersinia (n = 7) was 3.4 (95% CI 0.8–13.7%). Combining all four pathogens, the estimated percentage of cases that developed ReA was 2.6 (95% CI 1.5–4.7%). Due to high heterogeneity reflected by high I 2 values, results should be interpreted with caution. However, the pooled proportion developing ReA from studies with sample sizes (N) <1000 were higher compared with N > 1000 (6% vs. 0.3%), retrospective cohort studies were lower (1.1%) compared with CC or prospective cohorts (6.8% and 5.9%, respectively), and those where ReA cases are identified through medical record review were lower (0.3%) than those identified by a specialist (3.9%) or self-report (12%). The estimated percentage of people who developed ReA after infection with Campylobacter, Salmonella, Shigella, or Yersinia is relatively low (2.6). In the United States, this estimate would result in 84,480 new cases of ReA annually.
Introduction
Joint pain after bacterial dysentery was one of the first recognized long-term outcomes of diarrheal diseases dating back to the Civil War and other early outbreaks in military populations (Bollet, 1991). Reactive arthritis (ReA) is an inflammatory arthritis that develops after infection of a body site other than the joint (Schmitt, 2017). This spondyloarthropathic disorder manifests through inflammation of the joints and tissues after a gastrointestinal or genitourinary infection (Carter and Hudson, 2009; Townes, 2010). The mechanisms by which a distal site infection induces sterile joint inflammation are poorly understood. ReA is clinically defined as any joint pain starting within 2 weeks of a known inciting infection with no other underlying cause (Kingsley and Sieper, 1996; Pope et al., 2007; Townes, 2010). Symptoms typically last 3–12 months and may be intermittent, with a small percentage of persons developing chronic disease.
Estimating the burden of ReA is difficult and further complicated by limitations in diagnosing the inciting infection, particularly for foodborne enteric infections, which are common, affecting one in six Americans annually. The vast majority of cases do not seek medical care, and even fewer have microbiological tests performed to identify the infecting pathogen (Scallan et al., 2011). For those diagnosed with a relevant pathogen, it is unclear if the postinfectious sequelae (PIS) risks are adequately or effectively communicated by the clinician (Austhof et al., 2020). As such, joint pain after acute gastrointestinal illness is unlikely to be recognized as a sequelae by the patient (Hannu, 2011). An astute medical provider recognizing the antecedent infection is still hampered by the lack of diagnostic tests and inconsistent case definitions for ReA (Braun et al., 2000; Townes, 2010). These factors likely lead to significant under-reporting, resulting in an underestimate of incident ReA.
Epidemiologic studies of ReA vary in case identification and methodology due to these challenges. For instance, a study using medical record reviews can only rely on patients utilizing the same health care system for both their initial infection and follow-up visits, and requires accurate diagnoses and documentation (Larsen et al., 2018). Depending on case ascertainment, retrospective study designs can be subject to a limited ability to determine temporality, while prospective studies often rely on patient-reported outcomes, rather than physician diagnosis. Given these feasible differences, reported incidence estimates can vary widely.
To date, four systematic reviews on the incidence of ReA after foodborne infections have been published (Pope et al., 2007; Ajene et al., 2013; Keithlin et al., 2014, 2015); however, most relied on papers published ten or more years ago. The objective of this study was to conduct a systematic review and meta-analysis to estimate the proportion of ReA after enteric infection with the four most common foodborne bacterial pathogens with the largest evidence of association: Campylobacter spp., nontyphoidal Salmonella, Shigella spp., and Yersinia spp. We hope that the findings of this research enhance evidence-based patient management by increasing awareness of ReA among clinicians. In addition, the results of this research should help characterize the burden of PIS in estimates of the public health impacts of enteric infections, particularly foodborne disease burden estimates used in regulatory policy making (Hoffmann et al., 2015; Minor et al., 2015).
Methods
Selection of papers and data extraction
A previously published scoping review of PIS associated with common bacterial enteric pathogens was conducted using PubMed, Web of Science, and Embase to comprehensively identify the peer-reviewed literature (Pogreba-Brown et al., 2019). This systematic review builds upon our scoping review, and follows the criteria outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses recommendations for reporting (Shamseer et al., 2015). The following search strategy applied to all fields (example shown for PubMed) was used to identify articles: (“Campylobacter” OR “Salmonella” OR “Shigella” OR “Yersinia”) AND (“reactive arthritis” OR “Reiter's Syndrome” OR “postinfectious sequelae” OR “sequelae” OR “long-term” OR “long term” OR “consequences” OR “conditions” OR “outcomes”) with restrictions to articles published in English, Spanish, and Portuguese between January 1, 2000 and April 1, 2018 to provide the most recent evidence (full search strategy for each platform included in Supplementary Data). Inclusion of these languages was limited to the ability of the author reviewers. The reference lists of all relevant studies were also reviewed for additional papers.
For this study, all papers were screened initially on title and abstract to ensure that they utilized a case–control (CC) or cohort study design, and reported data on confirmed or probable ReA (Kingsley and Sieper, 1996; Pope et al., 2007) associated with culture-confirmed or author-defined probable cases of Salmonella, Campylobacter, Shigella, or Yersinia (in-depth screening process described in Pogreba-Brown et al., 2019). For CC studies, ascertainment of ReA occurred prospectively after acute infection, such that results from these studies can be interpreted similar to the prospective cohorts (PCs). Papers were excluded from the study if they only used serology for antibodies to determine the pathogen exposure (inability to determine temporality and association), if the studies only reported the proportion of ReA cases with a prior infection based on serosurveillance, if they provided only disease burden estimates through modeling, or there was a coinfection with Chlamydia trachomatis.
After initial screening, full manuscripts were reviewed, and data were extracted through a four-person team (E.A., A.A., A.O.D., and K.P.B.) with multiple quality control checks, such as blinding the inclusion/exclusion results by reassigning 10 randomly selected papers to a new reviewer to check for consistency in screening. Data from each paper were extracted, using a prespecified extraction survey in Qualtrics, independently by two reviewers to determine the proportion who developed ReA. Data on other measures of association (e.g., odds ratio, risk ratio) were not used because of inconsistent reporting among the articles. Conflicts between reviewers were resolved through consensus with a third reviewer. Additional data on the publication year, species, study design, country, study duration, diagnosis of the pathogen, and how ReA was determined were also extracted (data extraction tool included in Supplementary Data).
Method of case ascertainment was defined in three categories: (1) medical chart review, (2) disease confirmed by a specialist, and (3) self-report. Risk of bias was assessed independently by two reviewers against key criteria: selection of participants, assessment of exposure and outcome, outcome not present at start of study, matching or adjustment, assessment of prognostic factors, and adequate follow-up in accordance with methods described by The Cochrane Collaboration risk of bias assessment for cohort studies (The Cochrane Collaboration, 2020). Bias was assessed using four categories (definitely low risk of bias, probably low, probably high, definitely high risk of bias). Authors resolved disagreements by consensus. Institutional Review Board approval was not required for this study.
Meta-analysis
Logistic regression models were used to estimate the weighted proportion of ReA for single pathogens (Greenland, 1987). To account for within- and between-study variability, random-effects models with restricted maximum-likelihood estimator were used for the pooled analysis (Viechtbauer, 2010). When zero ReA case was reported in one study, 0.5 was added to all denominators and numerators that were used to calculate a pooled rate. Heterogeneity of each pooled dataset was evaluated by Cochran's Q test and Higgins I 2 test. The former tested homogeneity hypothesis based on chi-square distribution, while the latter is built on Cochran's Q statistics and degree of freedom (Cochran, 1954; Higgins and Thompson, 2002). If I 2 was >75% or the p-value of the Q test was <0.05, heterogeneity was considered high. I 2 reflects the proportion of variation across pooled studies that could not be explained by chance so a higher I 2 implies larger differences between the studies. I 2 values of 0–50% and 50–75% were considered low and moderate, respectively (Cochran, 1954). When high heterogeneity was observed, study parameters including region (North America, Europe), sample size (≤1000 participants vs. >1000), study design (CC, retrospective cohort [RC], PC), and ReA case ascertainment method (medical chart review, specialist, self-report) were explored by univariate meta-regression if at least four studies included that factor. Otherwise, heterogeneity was explored qualitatively through review of the studies' methodology. Publication bias was assessed by funnel plots for main analysis when >10 studies were involved. The bias was not assessed for exploratory analysis due to small number of studies in each stratum (Egger et al., 1997). A sensitivity analysis using the leave-one-out method was conducted (Viechtbauer and Cheung, 2010), and results are provided in the Supplementary Data; the analysis showed no change in the reported results. All statistical analyses were performed in RStudio (version 1.1.463).
Results
A total of 52 articles published between January 1, 2000 and April 1, 2018 were screened for inclusion criteria, resulting in 24 articles with 41 unique outcomes (Fig. 1; Table 1). Studies where ReA cases were determined by medical chart review were all large, retrospective studies where the exposure, defined as culture-confirmed or probable infection with one of the four pathogens and the outcome, ReA diagnosis, were recorded before the study in the same data system. Studies with ReA confirmed by a specialist were PC (n = 9), RC (n = 4), and through CC (n = 3) designs. ReA patients actively identified through routine public health surveillance systems or specialty clinics generally included a questionnaire, physical examination by a clinician and/or a review of the patients' symptoms and medical history. For ReA cases ascertained through self-report, exposures were identified by surveillance data (n = 10) or after an outbreak (n = 12). Follow-up questionnaires were often administered by phone or mail and diagnoses based on a review of patient-reported outcomes.
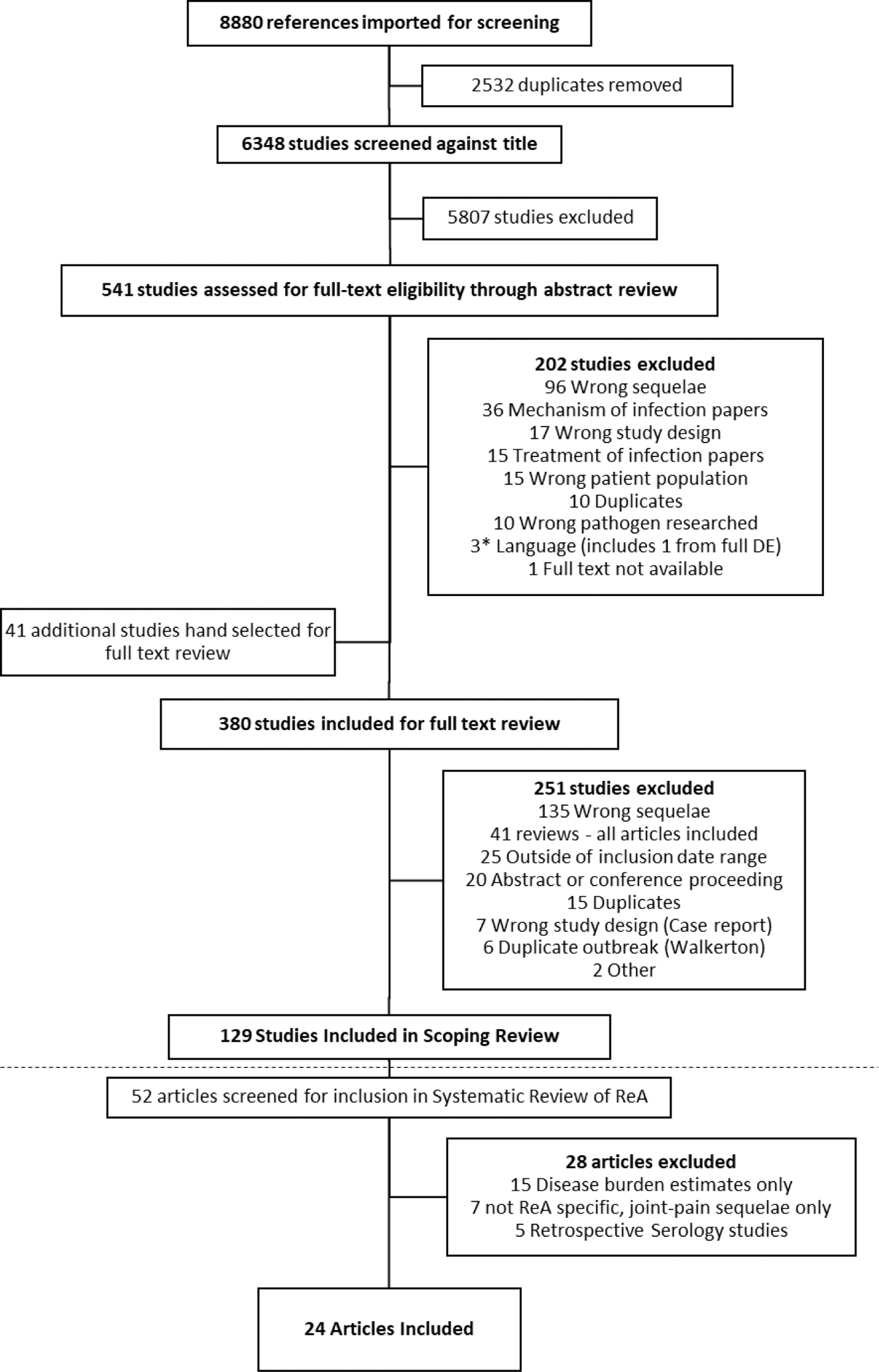
Flowchart of study inclusion for studies of ReA and Campylobacter, Salmonella, Shigella, and Yersinia published from 2000 to April 1, 2018. *See Methods section for inclusion and exclusion criteria. The dashed horizontal lines represent the beginning of the systematic review of ReA for papers included in this article. DE, data extraction; ReA, reactive arthritis.
Population Characteristics and Species Information for the Proportion of Cases Who Developed Reactive Arthritis by Pathogen, 2000 to April 1, 2018
Includes probable diagnoses of epidemiologically linked cases associated with outbreaks.
Self report of symptoms consistent with ReA without physician diagnosis including reactive arthralgias with an absence of pre-existing rheumatological conditions.
The species column for Salmonella states serotypes/serovars.
ReA, reactive arthritis.
Campylobacter
Eleven articles (Locht, 2002; Zia et al., 2003; Hannu et al., 2002, 2004; Helms et al., 2006; Doorduyn et al., 2008; Schiellerup et al., 2008; Ternhag et al., 2008; Townes et al., 2008; Schoenberg-Norio et al., 2010; Porter et al., 2013) (4 PC, 5 RC, 2 CC) were included to assess the proportion of Campylobacter-associated ReA. These studies accounted for 81,463 confirmed or probable cases of campylobacteriosis (70% came from one medical chart review study; Ternhag et al., 2008), of which 317 developed ReA. The majority of studies were conducted in Europe (n = 9) with two in the United States; three included children in their study populations. Five studies assessed for ReA within 4 weeks to 2 months from initial infection (no data were provided for six studies). Cases were ascertained through self-report (n = 4), medical chart review (n = 3), or diagnosis from a specialist (n = 4).
Meta-analysis
Using these 11 studies, the estimated percentage of Campylobacter cases that developed ReA was 1.71 (95% confidence interval [CI] 0.49–5.84%; Fig. 2). Heterogeneity between the studies was high (I 2 = 99.0%). Ternhag et al.'s (2008) study contributed the most to heterogeneity, and the pooled percentage increased to 2.7 after excluding it. The funnel plot was not symmetric, indicating a high risk of publication bias; the risk of bias assessment was low overall. The factor significantly contributing to the heterogeneity was how ReA status was defined. Specifically, case ascertainment of ReA through medical record review compared with disease status confirmed by specialist (p = 0.02). The estimated percentage of Campylobacter cases that developed ReA was 3.2 (95% CI 1.5–6.7%; I 2 = 91.3%) when the disease was identified by a specialist and 14.4 (95% CI 5.9–31.2%; I 2 = 97%) in self-reported studies. Estimates when cases of ReA were identified through medical chart review were unable to be calculated (n = 3); however, the estimates ranged from 0.03% to 0.14%.
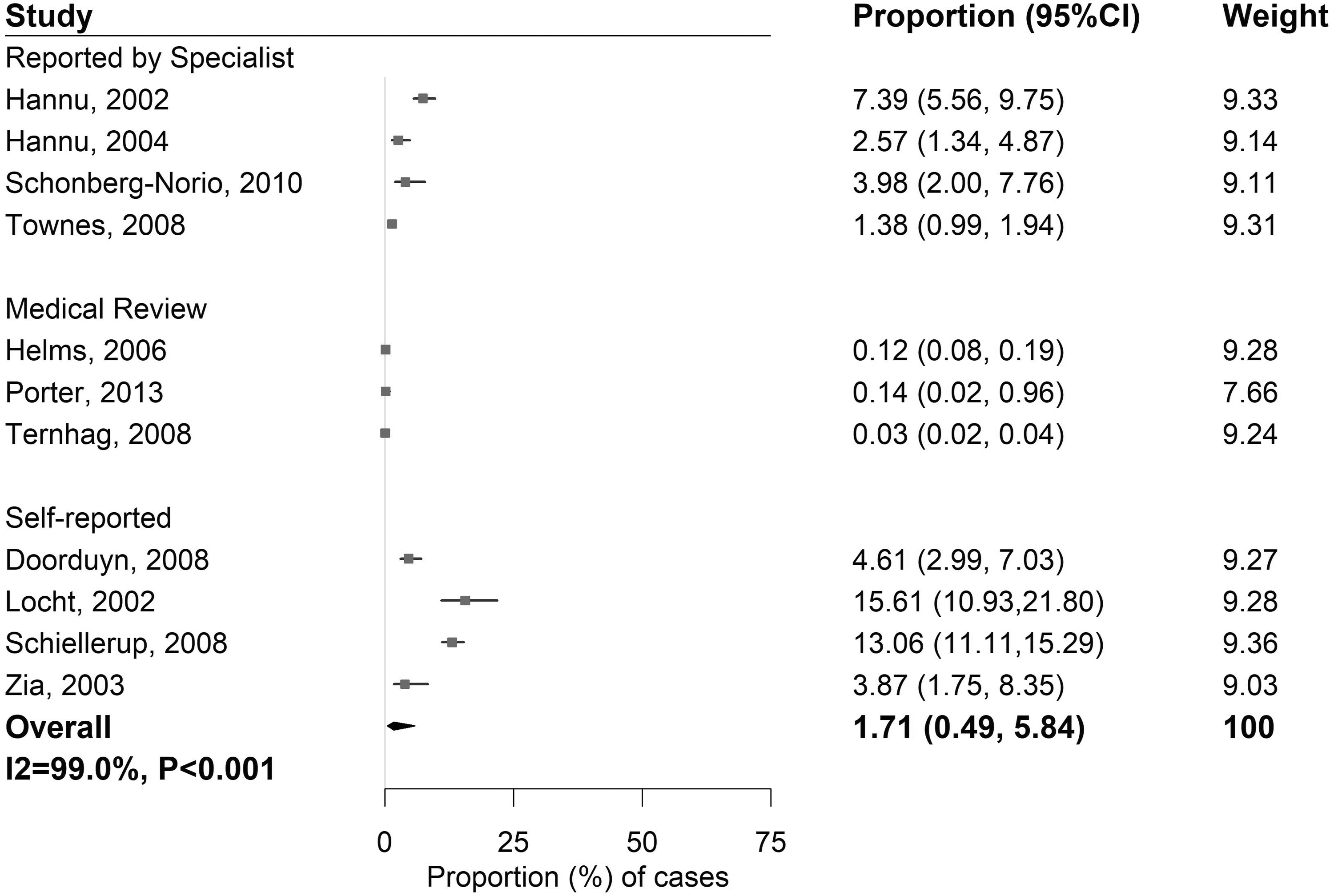
Proportion (%) of ReA cases among patients with an antecedent Campylobacter infection. CI, confidence interval.
Nontyphoidal Salmonella
Seventeen articles (Ekman et al., 2000; McColl et al., 2000; Urfer et al., 2000; Dworkin et al., 2001; Rudwaleit et al., 2001; Buxton et al., 2002; Hannu, 2002; Lee et al., 2005; Helms et al., 2006; Doorduyn et al., 2008; Rohekar et al., 2008; Schiellerup et al., 2008; Ternhag et al., 2008; Townes et al., 2008; Arnedo-Pena et al., 2010; Porter et al., 2013; Tuompo et al., 2013) (6 PC, 9 RC, 2 CC) were included to assess Salmonella-associated ReA. These studies accounted for 67,655 confirmed or probable cases with Salmonella (species list in Table 1), of which 483 developed ReA. The majority of studies were conducted in Europe (n = 9) with three in the United States; nine included children in their study populations. Eight studies assessed for ReA within 4 weeks to 3 months from initial infection with no data on duration for nine studies. ReA was determined through self-report (n = 5), medical chart review (n = 4), or diagnosis from a specialist (n = 8).
Meta-analysis
Analysis of these 17 studies found that the estimated percentage of Salmonella cases developing ReA was 3.9 (95% CI 1.6–9.1%; Fig. 3). The funnel plot indicated a high risk of publication bias; the risk of bias assessment was low overall. Heterogeneity between the studies was high (I 2 = 98.7%) with factors of sample size (p = 0.001) and ReA case ascertainment method (p = 0.05) contributing significantly. Helms et al.'s (2006) study contributed the most to heterogeneity, pooled percentage increased to 4.6 after excluding it. For studies with N ≤ 1000, the estimated percentage of Salmonella cases that developed ReA was 6.9 (95% CI 3.3–13.8%; I 2 = 97.1%). Estimates within studies with N > 1000 were not calculated due to the small number of studies (n = 3) but ranged from 0.1% to 1.3%. The estimated percentage of Salmonella cases that developed ReA was 0.7 (95% CI 0.1–6.1%; I 2 = 99.3%) when limiting analysis to studies utilizing medical chart review, 4.0 (95% CI 2.5–6.4%; I 2 = 78.4%) for those confirmed by specialist, and 13.4 (95% CI 2.7–46.3%; I 2 = 98.9%) for those that were self-reported.
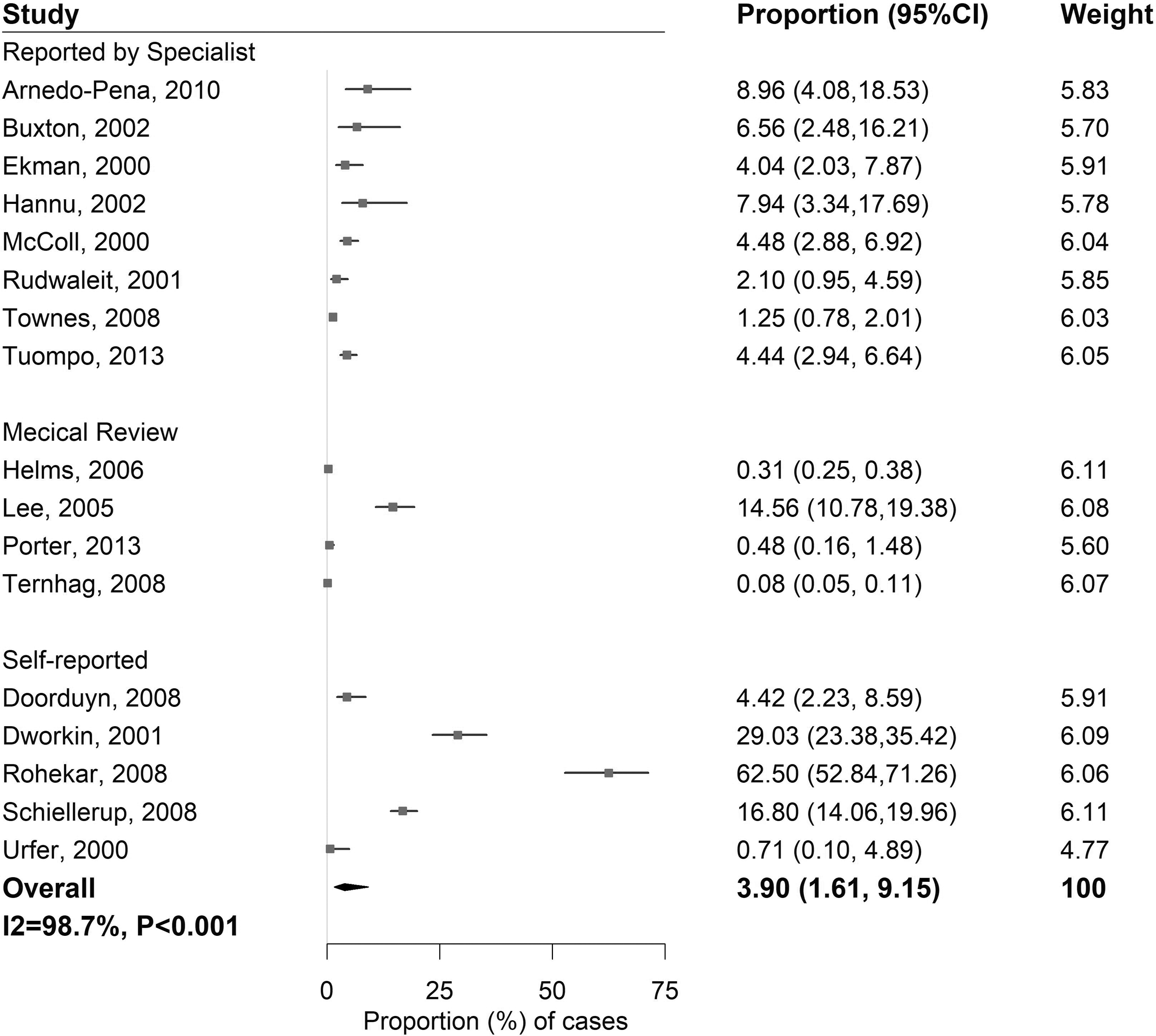
Proportion (%) of ReA cases among patients with antecedent nontyphoidal Salmonella infection.
Shigella
Six articles (Hannu et al., 2005; Helms et al., 2006; Schiellerup et al., 2008; Ternhag et al., 2008; Townes et al., 2008; Porter et al., 2013) (2 PC, 3 RC, 1 CC) are included in Table 1 to assess Shigella-associated ReA. These studies accounted for 6415 confirmed cases with Shigella (species list in Table 1), of which 36 developed ReA. Most studies were conducted in Europe (n = 4), while two were conducted in the United States. Three studies included children. The studies varied in duration for onset of ReA (4 weeks [n = 2], 90 days [n = 1], 2 months [n = 1], 6 months [n = 1], no data [n = 1]). Three studies identified ReA patients through medical chart review, two by a specialist, and one through self-report.
Meta-analysis
Using these six studies, the estimated percentage of cases of Shigella that developed ReA was 1.0 (95% CI 0.2–4.9%; Fig. 4). Publication bias was not assessed due to small number of studies included; the risk of bias assessment was low overall. Heterogeneity was high (I 2 = 95.1%) with the factors of population size (p = 0.005), study design (p = 0.01), and case ascertainment (p = 0.005) contributing significantly. Ternhag et al.'s (2008) study contributed the most to heterogeneity, pooled percentage increased to 1.8 after excluding it. For studies with N ≤ 1000, the estimated percentage of Shigella cases that developed ReA was 2.9 (95% CI 0.8–10.3%; I 2 = 91.0%). There were not enough studies to stratify results by method of case ascertainment.
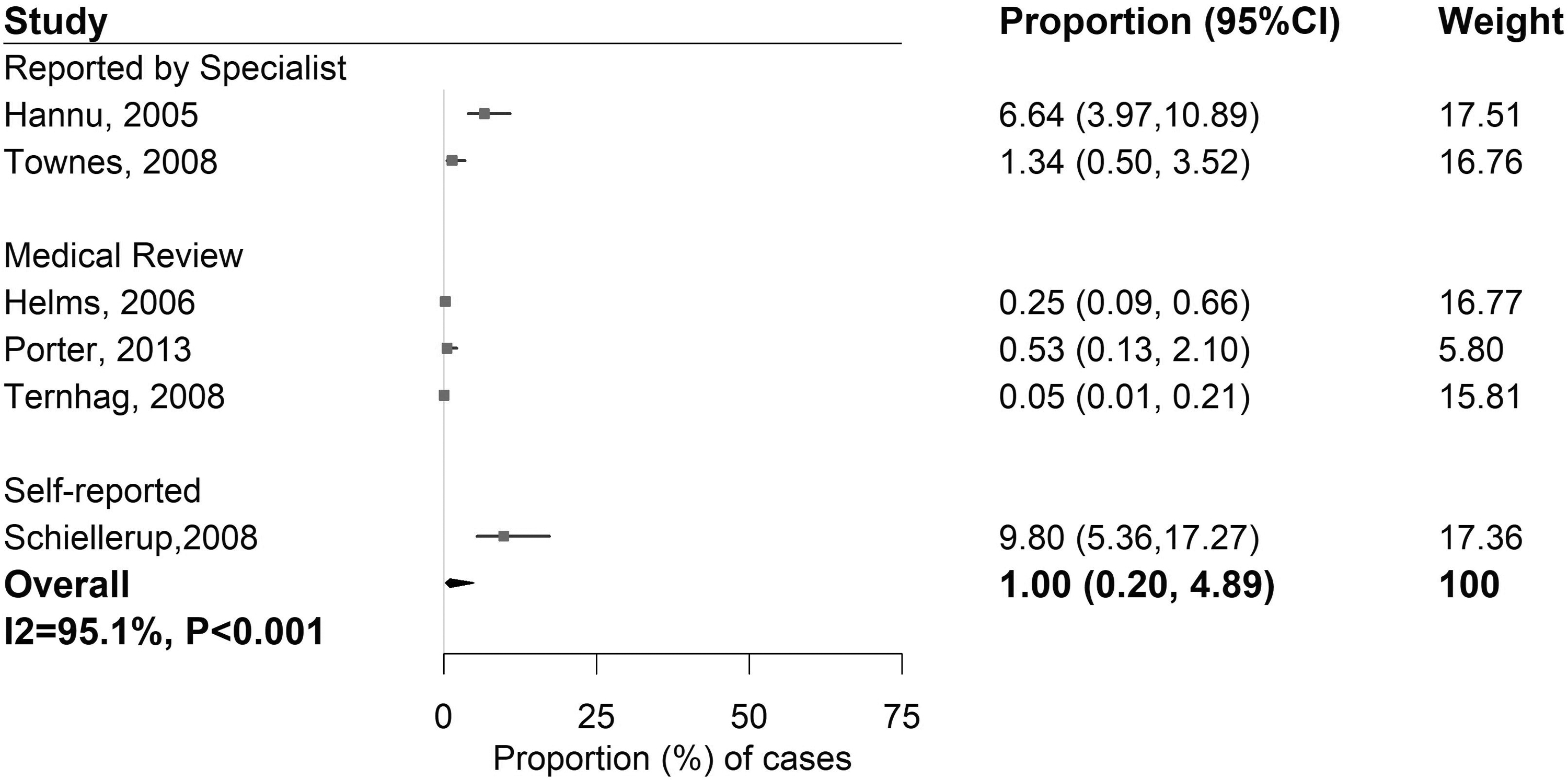
Proportion (%) of ReA cases among patients with an antecedent Shigella infection.
Yersinia
Seven articles (Hannu et al., 2003; Helms et al., 2006; Schiellerup et al., 2008; Ternhag et al., 2008; Townes et al., 2008; Porter et al., 2013; Rosner et al., 2013) were included to assess the proportion of Yersinia-associated ReA. These studies (2 PC, 4 RC, 1 CC) accounted for 9582 confirmed cases with Yersinia (species list in Table 1), of which 92 developed ReA. The majority of studies were conducted in Europe (n = 5) with the remaining two in the United States; four included children. The studies varied in duration for onset of ReA (4 weeks [n = 3], 90 days [n = 1], 6 months [n = 1], no data [n = 2]). Determination of ReA cases was made through medical chart review (n = 3), by a specialist (n = 2), or through self-report (n = 2).
Meta-analysis
Using the seven studies included in this review, the estimated percentage of cases of yersiniosis that developed ReA was 3.4 (95% CI 0.8–13.7%; Fig. 5). Publication bias was not assessed due to small number of studies included; the risk of bias assessment was low overall. Heterogeneity between the studies was high (I 2 = 97.5%). Helms et al.'s (2006) study contributed the most to heterogeneity, pooled percentage increased to 4.9 after excluding it. The factors significantly contributing to heterogeneity were the sample size (p < 0.001), and how ReA status was defined (p < 0.001). Specifically, in studies with N ≤ 1000, the estimated percentage of Yersinia cases that developed ReA was 12.8 (95% CI 7.3–21.5%; I 2 = 67.3%). There were not enough studies to stratify results by case ascertainment; however, estimates ranged from 4.17–13.24% for ReA cases identified by a specialist; 0.19–2.78% for those identified by medical chart review; and 11.79–23.37% for self-reported ReA cases.
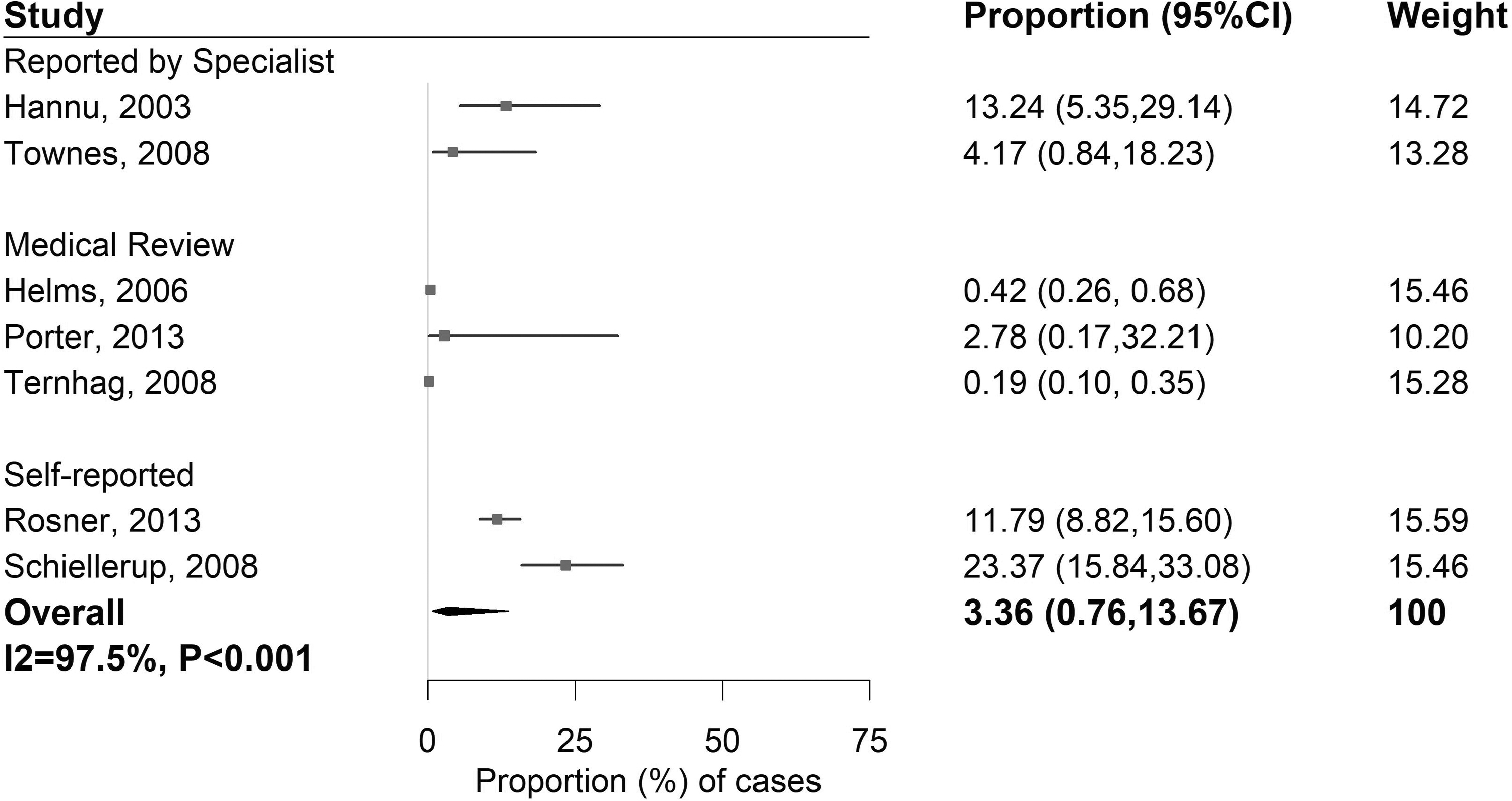
Proportion (%) of ReA cases among patients with an antecedent Yersinia infection.
Overall
The overall estimated percentage developing ReA across the four bacterial enteropathogens was 2.6 (95% CI 1.5–4.7%; I 2 = 98.6%; Supplementary Data). The weights for each study varied only slightly with a range of 1.65–2.55. In the funnel plot, dots representing single studies were distributed symmetrically, but clustered on the top, which implied no obvious publication bias and low variance within single studies. Overall, the risk of bias assessment was not high (Supplementary Data).
In each by-pathogen meta-analyses, we observed significant heterogeneity between factor levels in the studies. Studies with N ≤ 1000 reported a higher estimated percentage developing ReA (p < 0.001; 6.0%; 95% CI 3.8–9.2%; I 2 = 95.8%) compared with study populations N > 1000 (0.3%; 95% CI 0.1–0.9%; I 2 = 98.9%). In addition, while CC (6.8%; 95% CI 4.9–9.4%; I 2 = 68.7%) and PC (6.0%; 95% CI 2.9–12.1%; I 2 = 97.7%) study designs yielded comparable point estimates for ReA, estimates from RC studies, which most often utilized chart reviews to ascertain cases, were lower (p = 0.02; 1.1%; 95% CI 0.4–2.7%; I 2 = 98.5%). Studies identifying ReA through medical record review had lower rates (p < 0.001; 0.3%; 95% CI 0.1–0.8%; I 2 = 97.5%) than those identified by a specialist (3.9%; 95% CI 2.7–5.6%; I 2 = 83.2%), or through self-report (p < 0.01; 12.0%; 95% CI 6.4–21.4%; I 2 = 97.6%).
Discussion
Utilizing 41 reported outcomes from 24 papers, we found that the estimated percentage of people who developed ReA after infection with Campylobacter spp., nontyphoidal Salmonella, Shigella spp., or Yersinia spp. is relatively low (2.6). However, these four pathogens alone are estimated to cause 3.2 million illnesses in the United States every year (Scallan et al., 2011), which would result in an estimated 84,480 new cases of ReA every year using our overall estimate (Shah et al., 2009; Olson et al., 2019). These findings are similar to previous systematic reviews. Ajene et al. (2013) found that Campylobacter, Salmonella, and Shigella had a weighted mean incidence of 9, 12, and 12 cases per 1000 cases, respectively; however, the authors did not conduct a meta-analysis due to the limited number of included studies. In addition, Keithlin et al. (2014, 2015) reported estimates of ReA after infection with Campylobacter (2.86%) and Salmonella (5.80%), which are consistent with our findings here. These reviews were comprehensive, but on average the included studies were conducted 20 years ago (1978–2008).
Based on our results, a pooled mean is likely a biased estimate, given the influence of large medical chart reviews on the parameter estimates. Studies with very large populations N > 1000 (all medical chart reviews) had ReA estimates of 0.06% of Campylobacter cases developing ReA (data not shown) compared with studies in smaller populations (N ≤ 1000), where 4.55% of patients infected developed ReA. We hypothesize that the difference observed in these results may be due to broader versus more specific surveillance for this condition, meaning for studies that used broader passive surveillance such as medical records or patient databases they may find less cases of ReA in general compared with studies after an outbreak or a specific population of foodborne illness (active, more specific). This hypothesis is also highlighted by a similar subgroup meta-analysis for Salmonella. We found comparable, but slightly higher results with rates of ReA differing by case ascertainment method (2.6% for medical records, 7.7% for cases confirmed by a specialist, and 11.1–16.6% for self-reported cases depending on the scale used). In addition, ascertainment of ReA through medical record review relies on cases of foodborne illness to use the same health care system, which may contribute to the lower proportions observed (if both the foodborne illness and ReA are not identified within the same system this would artificially lower the rate due to patient dropout).
Acute gastrointestinal infection case definitions
ReA estimates varied slightly by pathogen, from 1.00% for Shigella, 1.78% for Campylobacter, 3.36% for Yersinia, and 3.73% for nontyphoidal Salmonella. While there are differences across all four pathogens, the results showed overlapping CIs, indicating that this outcome may be triggered by common pathogenic pathways related to these invasive enteric infections. One hypothesis is that bacterial fragments transit from the site of infection to the joint and induce an inflammatory response; however, it is unclear why these enteropathogens are most strongly linked epidemiologically (Colmegna et al., 2004). In general, most of the studies were conducted on culture-confirmed infections; however, four of the studies (McColl et al., 2000; Urfer et al., 2000; Dworkin et al., 2001; Hannu et al., 2004) included probable cases as well. All four of these studies were conducted after well-documented outbreaks where the pathogen was confirmed for a portion of the cases and others included in the study met the case definition for symptoms, exposure history, and temporality.
ReA case definitions
The definition of ReA has evolved over the years as noted in Hannu et al. (2006). A noted gap is the variability in ReA definition utilized, which in some studies included “joint or musculoskeletal” pain as well as clinical ReA. For many included studies, there were multiple defined outcomes. For example, in Schoenberg-Norio et al. (2010), 39% of patients (n = 79) who were contacted shortly after an acute Campylobacter infection reported joint pain after their infection, but only 8 (4%) met the case definition for ReA (Kingsley and Sieper, 1996). In some papers, data were provided for both types of endpoints and noted the potential for a higher proportion of postinfectious arthropathies, which may be more difficult to diagnose and to attribute to an inciting infection (Curry et al., 2010). A separate review of postinfectious joint pain may be useful; however, the inconsistency in the case definition may limit interpretability (Hannu et al., 2006). It was also difficult to obtain details on temporality and length of follow-up as some papers were excluded due to insufficient information on the temporal association of ReA with acute gastrointestinal infection.
Study design and reporting methods
Our subgroup analyses found more variation in rates of ReA due to study design than pathogen species. Retrospective cohort studies reported lower estimated percentages (1.1%) as compared with CC (6.8%) or PC (5.9%) study designs. Given that retrospective studies for these infections and outcomes are subject to reporting bias, it is possible that some retrospective studies underestimate the disease risk. While prospective studies may be subject to bias due to follow-up loss, the time period of ReA onset is short typically presenting 2 weeks after the initial enteric infection. This allows for the incidence of cases to be determined without any loss of participants, although duration of symptoms can be challenging and was not always reported.
There were large differences in estimated percentages for studies conducted through medical chart review (0.3%) as compared with the other two methods, either disease status confirmed by a specialist (3.9%) working on a study, or through self-report (12.0%). These findings are consistent with the other systematic reviews (Pope et al., 2007; Ajene et al., 2013; Keithlin et al., 2014, 2015) and make sense with the study design processes. Medical chart review relies on the infection and ReA being reported in the same hospital or billing system and a narrow case definition of International Classification of Diseases (ICD)9 or 10 codes—we would expect this proportion to be low. In addition, there is no ICD9 or 10 code for ReA (only Reiter's disease or dysenteric arthritis) so medical chart reviews will inherently underestimate risk. Self-reported symptoms vary by questionnaire used and can capture fewer specific outcomes—we would expect estimates from these studies to be high. In addition, only one study (Schiellerup et al., 2008) used a previously validated questionnaire and not all studies published the questions used, so interpretation of the self-reported symptoms is limited. It is important to note that there is no widely used and validated questionnaire for ReA. It is likely that some of the symptoms are associated; however, it is difficult to differentiate these clinical syndromes postinfection without a validated scale or confirmation by a specialist. Disease status confirmed by a specialist, who, in these studies, is someone who is clinically assessing patients often as part of a study or patient follow-up (such as after an outbreak), would then be considered a gold standard of these three methodologies with a more accurate representation of the disease burden of ReA.
Health economic and disease burden for these pathogens are inconsistent in their considerations of the impact of ReA (Scharff, 2012; Tam and O'Brien, 2016; Schmutz et al., 2017; Sundström, 2018), which can be substantial (Söderlin et al., 2003). However, given the potential economic and health care burden of these infections, it is critical this work continue to be developed. In the course of our review, we found several economic burden papers, many of which contained useful incidence and prevalence estimates. Utilizing the economic estimates was outside of the scope of this review, but our team believed these to be useful for future research and have identified these papers by pathogen in the Supplementary Data.
Limitations
This article expands on the efforts of previous systematic reviews (Pope et al., 2007; Ajene et al., 2013; Keithlin et al., 2014, 2015) using a more robust method of determining PIS rates of ReA in persons with these infections (i.e., assessing heterogeneity by reporting method, including more recently published articles). The inclusion/exclusion criteria for this systematic review (i.e., using a more specific case definition of ReA and confirmed or probable acute illness definitions) may have contributed to the overall lower rates of ReA compared with previous estimates in the literature.
For Shigella and Yersinia, three studies used a retrospective study design and reporting method through medical record review. The high heterogeneity may be due to type of medical records used and population served through each dataset: Porter et al. (2013) used a U.S. military database, Helms et al. (2006) used three national registries, and Ternhag et al. (2008) used hospital discharge and cause of death data. Due to the varying reporting methods and populations, high heterogeneity is expected. Interpretation of the overall estimates for ReA from these two pathogens should be limited, and more research should be conducted to explore this association further.
One limitation of the meta-analysis is the high I 2 value for some of the analyses, particularly for Campylobacter, and the pooled analyses across pathogens and likely reflects the varied study designs, as well as potential differences in populations. Interpretation of the results from this article is limited as the I 2 values are high, indicating that pooled analyses are not as appropriate. By providing ranges of the estimates as well as making comparisons across the pathogens stratified by variables in the regression, we hope to facilitate an appropriate interpretation of the estimates reported. The other limitation is high publication bias in single pathogen sections. Obvious asymmetric patterns in the corresponding funnel plots were observed, so caution is needed in interpreting the results. For example, the funnel plots for Salmonella (Supplementary Data) indicated that results from studies with relatively large samples or small variabilities did not converge, so further investigation was needed to explain the deviation. We should also note that for some analyses, there were only a few eligible studies included, limiting confidence around point estimates. This important limitation highlights the need for more epidemiologic research on ReA as sequelae of these enteric pathogens using more robust exposure and outcome definitions.
Finally, all of these studies were conducted in developed countries with no studies available in low- and middle-income countries, which is a notable gap in the literature. Among the countries included, there are differences related to health care systems that may have had an impact on health seeking behavior, but differences in study design, regardless of country, account for the largest variety in the estimates obtained from this dataset.
Conclusions
Consideration of ReA as a sequelae of enteric infection is important both for evidence-based patient management and for public health priority setting. This study provides an advancement in the risk estimates for use in subsequent models. Moving forward, more prospective studies identifying bacterial enteric illness cases through foodborne surveillance with valid clinical outcome assessments considering a range of postinfection arthritic symptoms are needed to better understand the true risk. While such studies are ongoing (Porter et al., 2020), these efforts should be complemented by basic science and preclinical research to elucidate disease mechanisms and to potentially facilitate the development of interventions to mitigate postinfectious ReA.
Footnotes
Authors' Contributions
All authors have contributed significantly to this article.
Acknowledgments
Data are available upon reasonable request from the corresponding author. We thank members of the “Long-term Sequelae of Foodborne Diseases” Workgroup. Those who were not authors helped us to contribute their insights, edits, and biweekly time; we also thank Andre Markon, Aurelie Pohl, Angela Lasher, Andre Estrin, and Beverly Wolpert.
Disclosure Statement
The views expressed in the submitted article are the authors' own and not an official position of the institution, funder Department of the Navy, Department of the Army, Department of Defense, nor the U.S. government. The findings and conclusions in this study are those of the authors and do not necessarily represent the official position of the U.S. government. The views expressed in this article are those of the authors and do not necessarily reflect the official policy of the U.S. Department of Health and Human Services, the U.S. Food and Drug Administration, the U.S. Department of Defense, or the U.S. government. Some authors are employees of the U.S. government. This work was prepared as part of their official duties. Title 17 U.S.C. §105 provides that “Copyright protection under this title is not available for any work of the United States Government.” Title 17 U.S.C. §101 defines a U.S. government work as a work prepared by a military service member or employee of the U.S. government as part of that person's official duties.
Funding Information
This work was supported by the U.S. Food and Drug Administration (Grant No. HHSF223201710181P).
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.