
Abstract
The objective of this study was to examine changes in healthcare-seeking behaviors and diagnostic practices around foodborne illness during the COVID-19 pandemic in a large university-based health system. A retrospective cohort study of individuals diagnosed with pathogens commonly transmitted through food between 2015 and 2020 was undertaken using electronic medical record data. Regression models were used to compare measured incidence rates of various foodborne pathogens as well as associated healthcare-seeking behaviors during the pandemic year of 2020 to previous years. Incidence of campylobacteriosis, cholera, and norovirus in 2020 significantly decreased, respectively, by 65.5% (p < 0.01), 90.1% (p = 0.02), and 73.0% (p = 0.03) compared with an average from 2017– to 019. Average annual visits for patients included in our sample significantly increased by 8.0% when comparing the average from 2017–2019 to 2020 (p < 0.01). These results suggest that the pandemic impacted healthcare use related to foodborne disease either due to reduced exposure to foodborne pathogens or reduced willingness to seek healthcare.
Introduction
The COVID-19 pandemic altered many aspects of our lives and behaviors. By the end of 2020, the pandemic resulted in 736,796 reported illnesses, 36,973 hospitalizations, and 13,602 deaths in Ohio [Ohio Department of Health (ODH), 2021]. Early in the pandemic, the Ohio governor issued a statewide stay-at-home order stopping all nonessential, in-person business including closing restaurants, bars and gyms, and limiting mass gatherings (Dewine et al., 2020). Since then, the pandemic has significantly changed life for Ohioans and people around the world. Healthcare delivery and healthcare-seeking behaviors have also significantly changed since the onset of the pandemic. Telemedicine and digital technology adoption have increased throughout the healthcare system due to pandemic-driven changes in healthcare-seeking behaviors (Golineli et al., 2020; Mann et al., 2020). However, little is understood about how healthcare delivery and healthcare-seeking behaviors around foodborne disease (FBD) changed during the pandemic.
Understanding disease trends are critical to establishing public health policies, prioritizing resource allocation, and evaluating effectiveness of intervention programs. Assessing trends in FBD is difficult since many patients do not seek medical care, and of those who do, few are tested to confirm illness etiology (Scallan et al., 2006). Thus, discrepancies in counts and estimates of undiagnosed, diagnosed, and laboratory-confirmed FBD exist. In addition, illnesses commonly perceived as foodborne can have other transmission routes, making their attribution difficult. In the United States (U.S.), FBD trends are largely monitored through Foodborne Disease Active Surveillance Network (FoodNet), an active sentinel surveillance system that is a collaboration between the U.S. Centers for Disease Control and Prevention (CDC), U.S. Food and Drug Administration, U.S. Department of Agriculture, and 10 state/local public health departments (CDC, 2015; Scallan et al., 2011). Owing to underreporting and underdiagnosis of FBD, multipliers are applied to FoodNet surveillance data to provide more accurate estimates of disease burden. These multipliers are typically estimated using self-reported data obtained through cross-sectional surveys of the general population and clinical laboratories in FoodNet sites.
FoodNet data suggest a decrease in laboratory-confirmed FBD during the pandemic (Ray et al., 2021), but it is unclear if this is due to changes in healthcare-seeking behaviors or a true reduction in incidence. This study sought to use electronic medical records (EMR) from a university-based health system to examine the impact of the pandemic on incidence and healthcare-seeking behaviors around FBD. EMRs are an alternative data source that can supplement surveillance data on disease trends and burden (Egger et al., 2012). In addition, EMR data can provide insights into healthcare-seeking behaviors of FBD patients (Tessier-Sherman et al., 2013). Improved understanding of healthcare-seeking behaviors can lead to improved understanding of the changes in incidence of reported, laboratory-confirmed FBD during the pandemic.
Materials and Methods
A retrospective cohort study was undertaken using EMR data from The Ohio State University (OSU) Healthcare System, which sees approximately 2.5 million patients annually (Anonymous, 2022). Information on clinical encounters, demographics, costs, procedures, medications, laboratory results, clinical reports, order entry, and radiology images for patients seen within the system are stored in OSU Wexner Medical Center’s Electronic Health Record and Information Warehouse (IWD). Diagnoses are coded using International Code of Diagnoses-9 (ICD-9) codes through September 30, 2015, and ICD-10 codes from October 1, 2015, onward.
The sample population covered all patients with data recorded in IWD between 2015 and 2020. Patients with diagnostic codes related to ten foodborne pathogens (Supplementary Table S1) were identified, and their data were extracted from IWD. In consulting with physicians on the study team, multiple visits recording the same diagnostic code were treated as a single illness episode if the visit was within 7 days of the previous visit. Patient visits with the same diagnostic codes that were separated by 8 or more days were considered distinct illness episodes.
Summary statistics were calculated for sociodemographic variables (i.e., age, gender, race, ethnicity, and zip code) overall and by pathogen. Annual differences in sociodemographic variables were tested using Pearson’s chi-square test (Pearson, 1900). Annual incidence rates were calculated for each pathogen using Poisson regression with an offset equal to the log of the total number of patients seen in OSU Healthcare System during the specified time (Frome and Checkoway, 1985). To assess the impact of the pandemic on measured incidence rates, incidence rates for 2020 were compared with the average incidence rate from 2017 to 2019 using a negative binomial regression model. Average annual visits to OSU Healthcare System and rates of different visit types (hospital visits, office visits, and telehealth visits) among patients with FBD diagnosis in 2020 were also compared with an average from the previous three years (2017–2019) using negative binomial regression with an offset equal to the log of the total number of visits made by FBD patients during the specified time. Negative binomial regression was also used to examine annual differences in the number of acute gastrointestinal illness visits (ICD-10 codes A00-A09; R10-R19), respiratory illness visits (ICD-10 codes J00-J99; R00-R09), and all other visits. Finally, a generalized linear model with a binomial distribution and logit link function was used to compare the risk of being hospitalized in 2020 compared with the previous three years (2017–2019) for FBD patients.
Statistical analyses were performed using SAS v.9.4 for Windows (SAS Institute Inc., USA). Ethical approvals were obtained from The Ohio State University Biomedical Institutional Review Board.
Results
A total of 734 unique patients had a total of 887 clinical encounters with a FBD diagnostic code for one of the ten study pathogens from January 1, 2015, to December 31, 2020. A greater proportion of patients diagnosed with FBD were female with a gender ratio near 60:40, and no significant year-to-year differences were observed (p = 0.75) (Supplementary Table S2). Most patients diagnosed with FBD were white non-Hispanic individuals (68.7%) followed by Black non-Hispanic individuals (22.3%). Overall, yearly variations in proportions of different racial groups with FBD diagnostic codes were not significant (p = 0.08). The only significant changes were an 8-fold increase in Asian patients between 2015 and 2020 (p < 0.01) and a nearly 2-fold increase in Black Non-Hispanic patients between 2016 and 2020 (p = 0.04). Although there were no significant yearly differences in the proportion of individuals within each age group (p = 0.45), the proportion of 60–69-year-olds and 70–79-year-olds was higher in 2020 compared with 2019. During the same time period, the proportion of patients aged 40–49 and 50–59 years decreased.
Annual incidence, while not always statistically significant, decreased between 2015 and 2020 for most pathogens (Table 1, Fig. 1). The measured incidence of norovirus, Vibrio cholera, and Campylobacter spp. significantly decreased in 2020 compared with the 2017–2019 average by 73.0% (95% CI: 11.9%, 91.7%; p = 0.03), 90.1% (95% CI: 27.1%, 98.7%; p = 0.02), and 65.5% (95% CI: 41.0%, 79.8%; p < 0.01), respectively (Table 1). Measured incidence of Salmonella spp., Shigella spp., Shiga toxin-producing Escherichia coli (STEC), Listeria monocytogenes, and Yersinia enterocolitica also decreased in 2020 compared with 2017–2019, although these differences were not statistically significant. Measured incidence of Toxoplasma gondii and amebiasis increased in 2020 compared with 2017–2019, but neither difference was significant (Table 1).
Comparison of Case Counts, Incidence Rates, and Percent Change in Incidence Rates for 8 Foodborne Pathogens from 2020 to the Previous 3 Years (2017–2019) Averaged
p-values were significant at alpha = 0.05.
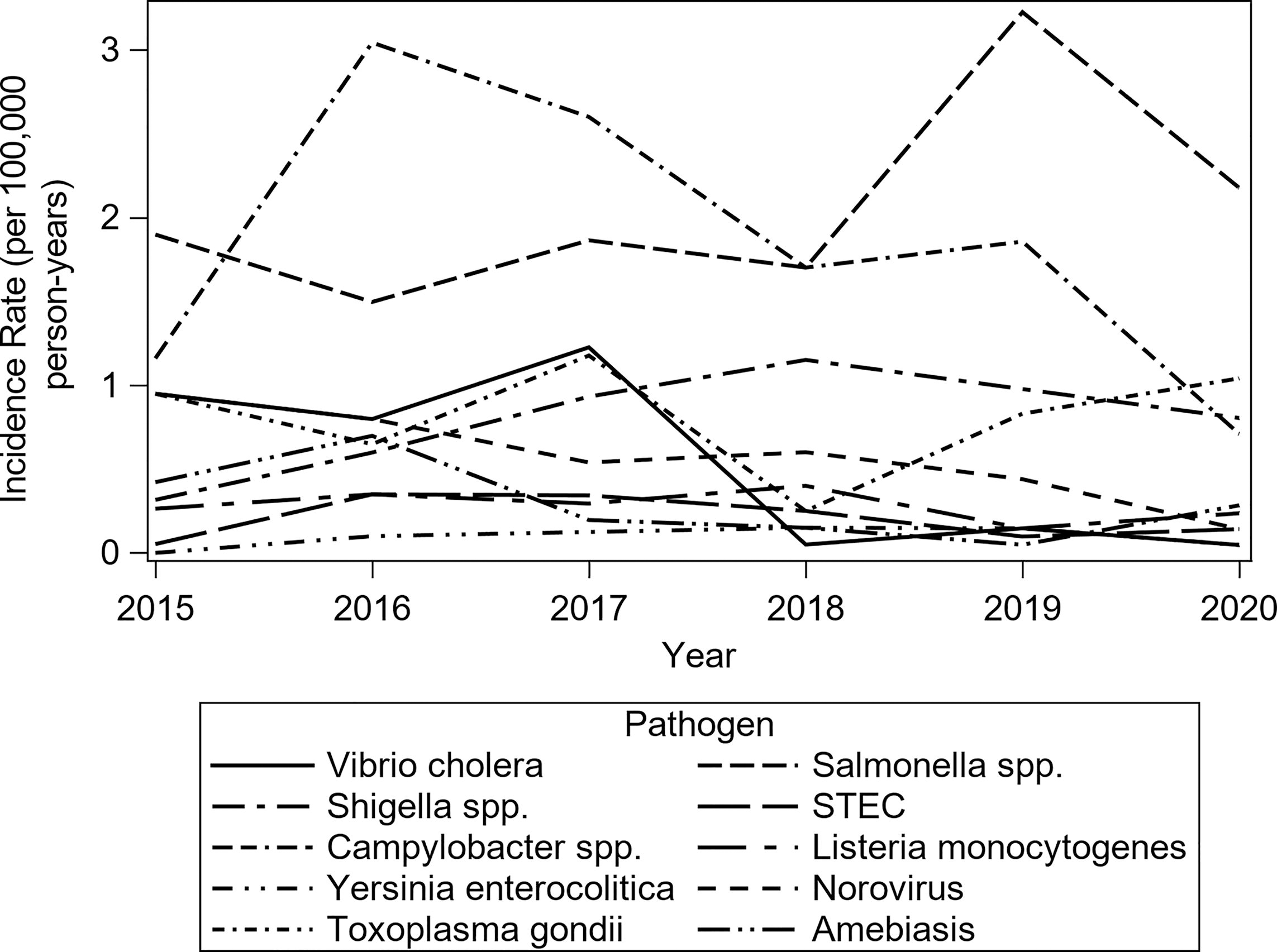
Annual incidence rates of definitive foodborne pathogens from 2015 to 2020.
Although significant decreases were observed in measured incidence rates for two of the ten pathogens examined, healthcare-seeking remained largely constant (Fig. 2). OSU Healthcare System records approximately 250,000 patient visits per month. There was a sharp drop in the number of monthly visits for March–May 2020. In addition, the number of visits jumped up to over 300,000 per month from July to December 2020. Within the cohort of diagnosed FBD patients, the average number of annual visits increased 7.7% (95% CI: 4.8%, 10.6%; p < 0.01) in 2020 compared with the average from the previous 3 years (2017–2019) (Fig. 3). However, when comparing 2020 to 2019 alone, the change was only 2.9% (95% CI: −0.1%, 6.3%; p = 0.09). Notably, the total number of FBD patients seeking care in 2020 was lower than the total for 2019 or the average from 2017 to 2019 (Table 2). Furthermore, the rate for different visit types significantly changed in 2020 compared with the 2017–2019 average. Hospital visit and office visit rates, including visits for symptoms, increased 10.7% (95% CI: 4.9%, 16.8%; p < 0.01) and 10.9% (95% CI: 7.3%, 14.7%; p < 0.01), respectively, whereas telehealth visits increased 15274% (95% CI: 10662.9%, 21861.0%; p < 0.01) (Table 3). However, despite the rates of these visits increasing, total number of visits decreased to 1,700 in 2020 from 2,051.7 on average annually between 2017 and 2019. This suggests that a smaller number of patients included in our sample sought care more frequently in 2020 than in previous years.

Total monthly visits within the Ohio State University (OSU) Healthcare System by year.
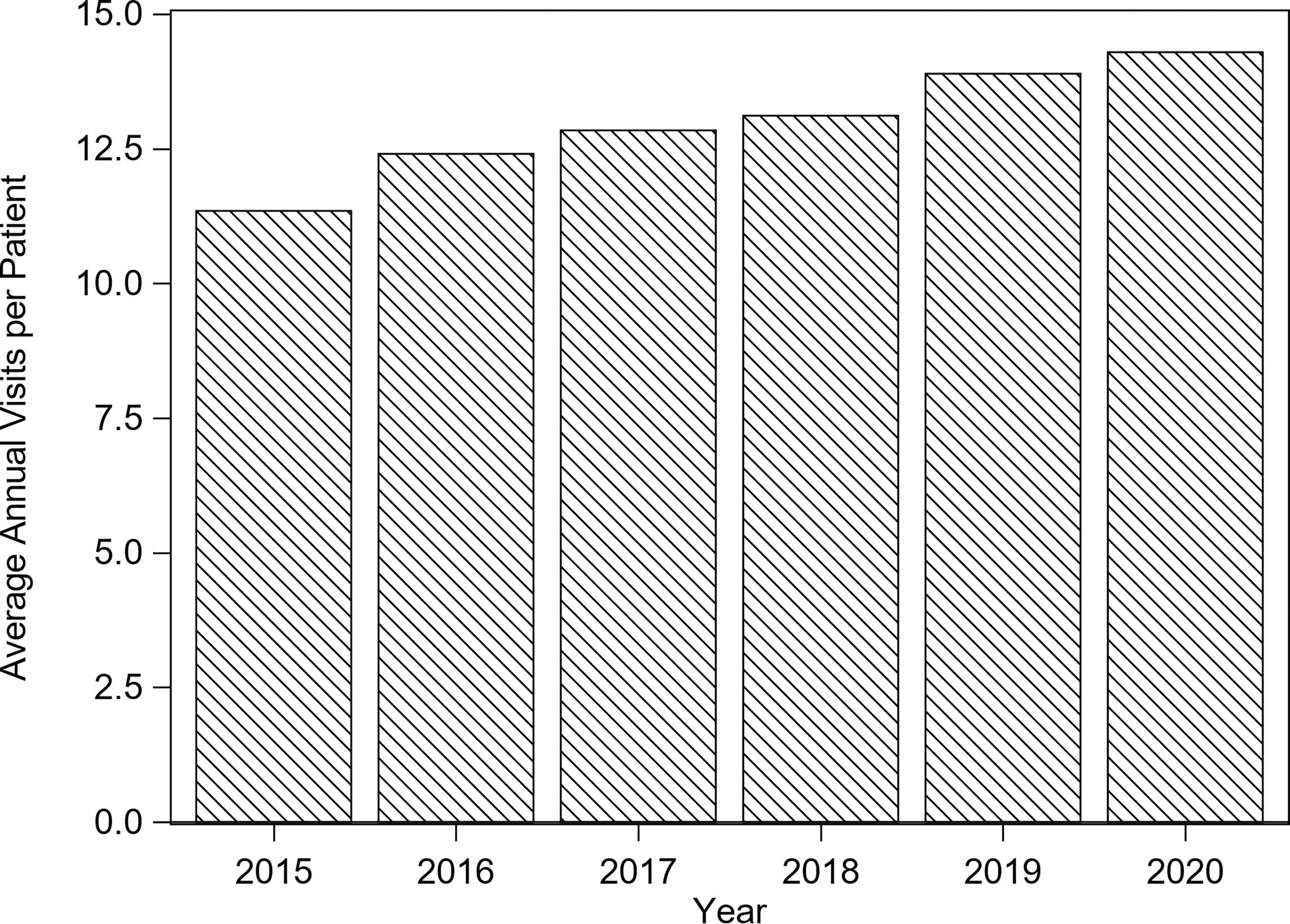
Average number of annual visits among patients with a foodborne disease diagnosis.
Comparison of Average Number of Annual Visits per Patient from 2020 to 2019 and to the Average from the Previous 3 Years (2017–2019)
p-values were significant at alpha = 0.05.
Comparison of the Rates of Different Visit Types per Patient and Reason for Visit from 2020 to the Average from the Previous 3 Years (2017–2019)
Patients had initial ICD-10 code for AGI (A00-A09, R10-R19).
Patients had initial ICD-10 code for respiratory illness (J00-J99, R00-R09).
Patients had other initial ICD-10 code (mental or behavioral conditions, skin conditions, musculoskeletal conditions, etc.).
p-values were significant at alpha = 0.05.
AGI, acute gastrointestinal.
Finally, reasons for seeking care also changed in 2020 compared with the previous three years. Rates of respiratory and other related visits significantly increased 24.9% (95% CI: 14.5%, 36.2%; p < 0.01) and 35.5% (95% CI: 31.4%, 39.7%; p < 0.01), respectively, in 2020 compared with the 2017–2019 average (Table 3). While rates of respiratory and other related visits increased, the rate of gastrointestinal related visits decreased 1.6% (95% CI: −13.0%, 11.3%; p = 0.80), though this decrease was not statistically significant. However, the total number of acute gastrointestinal (AGI) visits in 2020 was lower than the average total number of annual visits from 2017 to 2019. Lastly, FBD patients in 2020 had 1.81 (95% CI: 1.20, 2.72; p < 0.01) times greater risk of being hospitalized than FBD patients seen from 2017 to 2019.
Discussion
Given that the COVID-19 pandemic disrupted nearly all parts of life, unsurprisingly, changes in incidence of and healthcare-seeking behavior around FBD were observed in 2020. To our knowledge, four studies have examined changes related to FBD during the pandemic and none have determined whether any changes were due to true changes in incidence or changes in healthcare-seeking behaviors (Armistead et al., 2022; Bassal et al., 2021; de Miguel Buckley et al., 2020; Ray et al., 2021). One study conducted using Colorado Health Observation Regional Data Service (CHORDS) data found a 52% decrease in AGI visits during 2020 compared with the average from 2017 to 2019 (Armistead et al., 2022). However, the study only looked broadly at AGI visits, did not examine changes for specific FBD, or assess the relationship between decreased visits and AGI incidence. In contrast, the present study analyzed various aspects of FBD patient healthcare-seeking behaviors to better characterize how decreased healthcare visits may affect decreases in diagnosed FBD during the pandemic. By examining changes in both healthcare-seeking behaviors and FBD incidence, a better understanding of how the pandemic affected other infectious diseases may be developed.
The results of this study corroborate results from the FoodNet Annual Report (Ray et al., 2021), suggesting that incidence of laboratory-confirmed FBD decreased during the pandemic. FoodNet found significant decreases in nearly all monitored foodborne pathogens for 2020 (Ray et al., 2021). The authors of the FoodNet Annual Report acknowledged that a combination of COVID-19 control measures and changes in healthcare-seeking behavior may have contributed to the observed results. However, a limitation of surveillance data is that it does not allow for an analysis of changes in healthcare-seeking behaviors during 2020. In the present study, significant decreases in incidence were observed for three pathogens (norovirus, Vibrio cholera, and Campylobacter spp.) in 2020. While not significant, incidence for five other pathogens (Salmonella spp., Shigella app., STEC, Listeria monocytogenes, and Yersinia enterocolitica) decreased in 2020. This lack of statistical significance could indicate that decreases were within the normal range of variation for these pathogens. Another explanation could be that the present study was underpowered to detect smaller decreases in incidence rates for pathogens with few cases captured within OSU Healthcare System.
Significant decreases in incidence observed in the present study may be due, at least in part, to decreased healthcare-seeking behaviors. Although FBD incidence decreased in 2020, the average number of annual visits among patients with FBD diagnoses remained constant and, in some cases, increased. However, fewer total patients with FBD diagnoses sought care in 2020 than in prior years. This suggests that, though there were fewer patients willing to seek care, those that sought care did so more frequently in 2020. In addition, the finding that patients in 2020 had higher risk of being hospitalized than in previous years suggests that primarily patients with severe FBD were seeking care during the pandemic. Total visits to OSU Healthcare System dropped from March to May 2020, corresponding with the first cases of COVID-19 being reported within Ohio and the governor’s stay-at-home order (Dewine et al., 2020). By July 2020, total visits had risen to new highs compared with previous years, likely due to an increase in COVID-19 related visits or rescheduling of previously cancelled visits. Even though there were fluctuations in total monthly visits within OSU Healthcare System, they were largely expected given the environment surrounding the pandemic.
Other studies have found similar results regarding changes in healthcare-seeking behaviors in 2020. Two studies have noted decreased hospital admissions and emergency room visits for non–COVID-19–related illnesses (Birkmeyer et al., 2020; Westgard et al., 2020), although neither study explored reasons for this. A case study in Rhode Island found that fear of contracting the virus may have played role in both the reduced number of illnesses due to social distancing and reduced willingness to seek care (Messac et al., 2020), but these results cannot be generalized to the larger population. One study of respiratory illnesses in Alaska found a significant reduction resulting from enhanced social distancing measures (Nolen et al., 2020). However, social distancing measures may not have the same effect on FBD as they do on respiratory diseases as the transmission modes are different. A Spanish study that examined the impact of the pandemic on FBD found a significant decrease in FBD cases in 2020 (de Miguel Buckley et al., 2020). However, the study speculated that social distancing reduced FBD by limiting dining out but offered no evidence to support the claim. Similarly, an Israeli study of found significant decreases in incidence of shigellosis and salmonellosis with shigellosis incidence showing a far greater decrease (Bassal et al., 2021). The authors speculated this was due to Shigella spp. transmission via direct person-to-person contact, not just through contaminated food like Salmonella. However, the authors failed to consider the possibility that people were less willing to seek care during the pandemic. Further research is needed to verify these decreases in incidence in other populations and identify whether the observed changes are due to changes in healthcare-seeking behaviors or due to improved hygiene and control measures implemented during the pandemic.
For patients with FBD diagnosis, an increase in the average number of annual visits per patient was seen in 2020 compared with an average from 2017 to 2019. Given that the rate of respiratory-related visits increased in 2020 when compared with the previous three years, this suggests that perhaps patients made more COVID-19–related healthcare visits in 2020. Among the FBD study population, frequency of healthcare visits remained constant between 2019 and 2020 and increased when comparing 2020 with the average from 2017 to 2019. This consistency in visit frequency suggests that FBD patients were still seeking care or their appointment types had changed. For example, FBD patients may have made more AGI-related visits in prior years but made more COVID-19–related visits in 2020. This could also explain why visits remained high, but FBD incidence decreased. Since FBD patients made fewer gastrointestinal-related visits in 2020, this again suggests fewer patients overall sought care for FBD in 2020. Those FBD patients that sought care made more frequent visits, specifically for COVID-19 or respiratory-related illnesses. Furthermore, each visit type rate increased, especially telehealth visits, suggesting a major shift in how patients sought care during the pandemic. When comparing visit data with incidence data, our results showed a decrease in FBD incidence despite the average number of annual visits and demographics of FBD patients remaining constant or even increasing in 2020. As stated above, appointment types and underlying reasons for the visits may have changed, which may partly explain why FBD incidence decreased in 2020. Changes in other behaviors such as eating out less frequently, closing of daycare centers, limited travel, improved handwashing, and social distancing may also have contributed to observed decreases in incidence.
The present study has several limitations. First, this study is limited to patients seen within OSU Healthcare System, and as such, the results cannot be generalized to the entire U.S. population. Second, patients in this study may not be representative of all patients with FBD since many patients do not seek medical care (Scallan et al., 2011). Furthermore, few children were included in this study since most children in OSU Healthcare System’s catchment area visit a children’s hospital system instead. Third, we assumed that entire year of 2020 was impacted by the COVID-19 pandemic, even though cases were not reported within Ohio until March 2020. Fourth, this study used EMR data, which are not designed for research purposes and, thus, could bias results (Verheij et al., 2018). Potential sources of bias may include delivery of care (only patients seeking care are included), incorrect recording of diagnostic codes, improper extraction of EMR data, and improper translation into an operational database (Verheij et al., 2018). In addition, EMR data and ICD codes can underrepresent the number of laboratory-confirmed illnesses. Finally, even though the pathogens included in the study are commonly perceived as foodborne pathogens, source attribution data were not available. Therefore, the source of these illnesses may not necessarily be foodborne.
In conclusion, this study found significant decreases in measured incidence of norovirus, Vibrio cholera, and Campylobacter spp. in 2020, while healthcare visit frequency remained constant or even increased among a smaller number of FBD healthcare seekers. This study provides a first step in examining the intersection of incidence, diagnostic practices, and healthcare-seeking behaviors using EMR data. Future studies should use larger, more representative datasets and explore the relationships with a wider group of pathogens.
Footnotes
Acknowledgments
The authors would like to thank Jing Ding and the OSU IWD for providing study data.
Authors’ Contributions
J.A.B.: Conceptualization, Methodology, Software, Validation, Formal Analysis, Data Curation, Writing—Original Draft, Writing—Review and Editing, Visualization, Project Administration, Funding Acquisition. R.L.S.: Conceptualization, Methodology, Validation, Writing—Review and Editing, Funding Acquisition. J.M.B.-L.: Conceptualization, Methodology, Validation, Writing—Review and Editing, Funding Acquisition. B.B.K.: Conceptualization, Methodology, Validation, Data Curation, Writing—Original Draft, Writing—Review and Editing, Supervision, Project Administration, Funding Acquisition.
Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
Research support was provided by state and federal funds appropriated to The Ohio State University, College of Food, Agricultural, and Environmental Sciences, Ohio Agricultural Research and Development Center.
Supplementary Material
Supplementary Table S1
Supplementary Table S2