
Abstract
Consumers can be exposed to many foodborne biological hazards that cause diseases with varying outcomes and incidence and, therefore, represent different levels of public health burden. To help the French risk managers to rank these hazards and to prioritize food safety actions, we have developed a three-step approach. The first step was to develop a list of foodborne hazards of health concern in mainland France. From an initial list of 335 human pathogenic biological agents, the final list of “retained hazards” consists of 24 hazards, including 12 bacteria (including bacterial toxins and metabolites), 3 viruses and 9 parasites. The second step was to collect data to estimate the disease burden (incidence, Disability Adjusted Life Years) associated with these hazards through food during two time periods: 2008–2013 and 2014–2019. The ranks of the different hazards changed slightly according to the considered period. The third step was the ranking of hazards according to a multicriteria decision support model using the ELECTRE III method. Three ranking criteria were used, where two reflect the severity of the effects (Years of life lost and Years lost due to disability) and one reflects the likelihood (incidence) of the disease. The multicriteria decision analysis approach takes into account the preferences of the risk managers through different sets of weights and the uncertainties associated with the data. The method and the data collected allowed to estimate the health burden of foodborne biological hazards in mainland France and to define a prioritization list for the health authorities.
Introduction
According to the World Health Organization, around 200 diseases are of foodborne etiology, constituting a serious public health problem with a significant socioeconomic impact (WHO, 2022).
Food contamination can occur at all stages of the food chain and by various biological hazards. Among these hazards responsible for foodborne diseases, bacteria, viruses, and parasites are the most common. There is a wide range of clinical outcomes associated with foodborne illnesses. Most commonly, they manifest as gastrointestinal symptoms, but they can also produce neurological, obstetrical, and immunological symptoms. The burden of foodborne diseases is very unevenly distributed between low- and high-income countries, in a given country as well as in the population, with children under five bearing the greatest burden (WHO, 2022). Foodborne diseases are largely preventable and partially controlled, and thereby reducing their disease burden. At the national level, it is important to build and maintain adequate food systems and infrastructures to respond to and manage food safety risks along the entire food chain and to promote multi-sectoral actions and collaborations among public health, animal health, agriculture, and other relevant sectors. Effective and transparent risk management by competent authorities is also very important and necessary, as is the integration of food safety into broader food policies. At the food business operator level, it is necessary to ensure the safety of foods as well as to provide supporting proof of good application of hygiene practices and sufficient control of the main hazards of their sector of activity (Federighi et al., 2020). However, the food safety system is not set in stone and the search for improvement is ongoing. For example, improvement will concern better knowledge of the true burden of foodborne biological hazards and their association with food vehicles (Federighi et al., 2020). Given the large number of food-related risks, the public risk manager cannot address all of them at the same time. In order to best allocate means and resources, in particular for official controls, while optimizing food safety, a risk prioritization tool is essential.
The present work was carried out following a formal request from the French risk managers (General Directorate for Food; General Directorate for Competition Policy, Consumer Affairs and Fraud Control; General Directorate for Health). The aims of this study are (1) to identify the foodborne biological hazards that are currently of health concern in mainland France, (2) to estimate their burden, and (3) to propose a transparent and data-based method for ranking these hazards to help the risk manager to better target public health policies and capacities.
For this purpose, a multicriteria decision analysis (MCDA) approach is proposed, considering the different components of the risk as well as the preferences of the risk managers and the uncertainties associated with the data, in order to help the decision-maker to establish the management priorities.
Materials and Methods
Our general approach to ranking foodborne biological hazards consisted of three steps. The first step was to make a list of hazards that are of health concern in mainland France. The second step was the collection of data to estimate the health burden of diseases associated with these hazards through food (incidence, Disability Adjusted Life Years [DALYs]) and then calculate the burden. The third step was the ranking of hazards according to a multicriteria decision support model using the ELECTRE III method (Roy, 1985). The criteria reflect the two components of risk as defined by the Codex Alimentarius (1999): the severity of the adverse effect and the probability of its occurrence.
We tested several sets of parameters and criteria weights that could be used to inform the manager of the impact of choices on the final ranking.
The effect of uncertainty on the risk ranking was also considered as described in the Supplementary Appendix S1.
Identification and selection of biological hazards
Initially, the identification of biological agents that are pathogenic to humans (bacteria, viruses, prions, parasites) was based on the lists proposed by the Belgian Scientific Institute of Public Health (Belgian Biosafety Server, 2021) (www.biosafety.be). These lists were chosen because they are the most exhaustive. They were drawn up in 2008 and list 335 biological agents that are pathogenic to humans. The resulting list of 335 hazards is referred to as the “long list”. This long list does not include mycotoxins and marine biotoxins, which are considered chemical hazards.
The selection of biological hazards for health prioritization was based on current knowledge of hazards, exposure routes, and population susceptibility. This selection was done in three steps.
In the first step, the “long list” of biological agents pathogenic to humans was screened to select those transmissible through food (“foodborne hazards list” in Fig. 1). Second, the “foodborne hazards list” was screened against one of the following four filters:
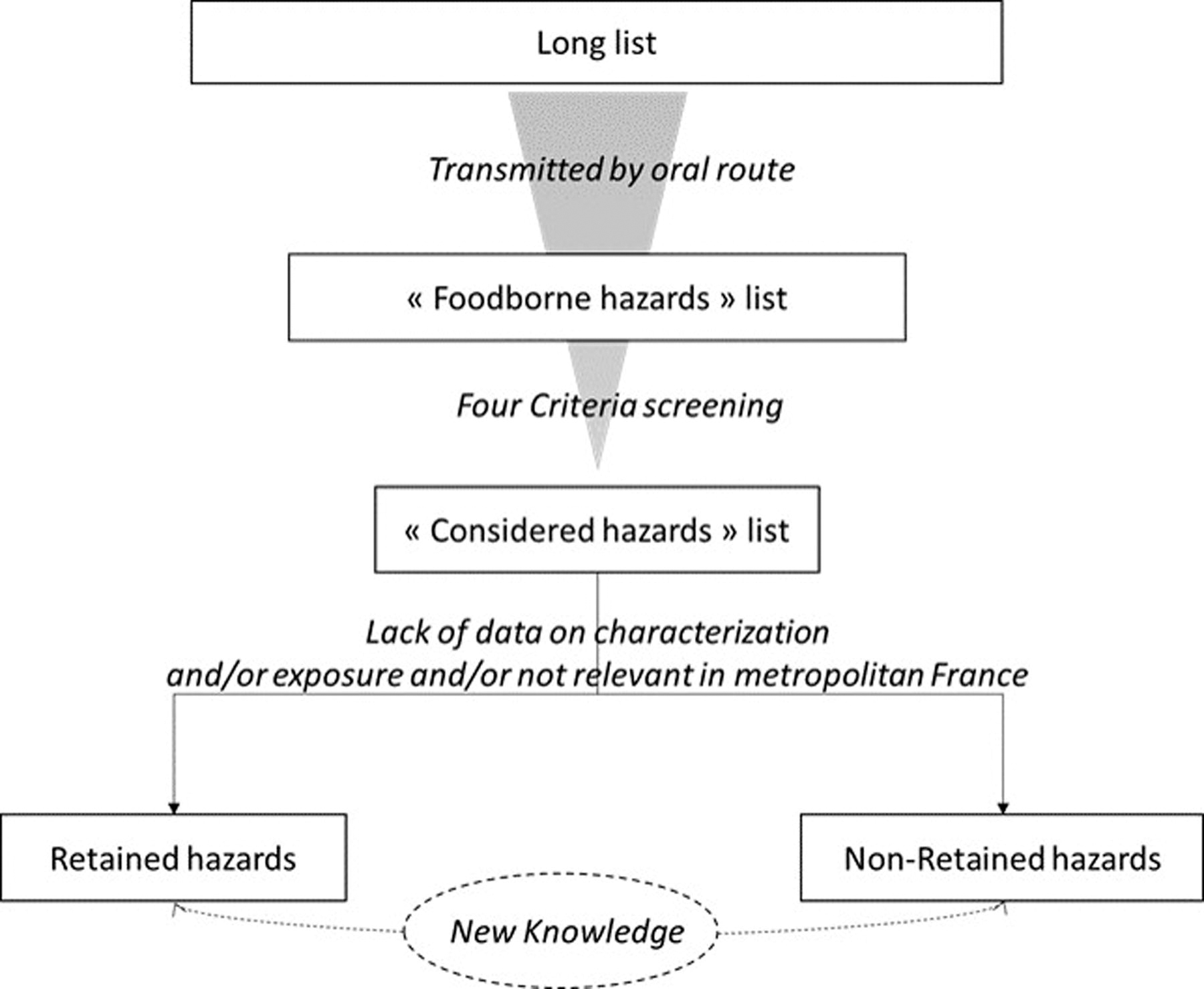
Methodology of selection of relevant biological hazards.
Hazard considered in European regulations related to zoonoses (European Commission, 2003) or microbiological criteria (European commission, 2005);
Hazard considered in the datasheet on foodborne microbiological hazards published by the French Agency for Food, Environmental and Occupational Health and Safety (Anses) (Anses, 2022);
Hazard listed in the European Food Safety Authority (EFSA) zoonoses reports in 2015 or 2016 (European Food Safety Authority and European Centre for Disease Prevention Control, 2017; European Food Safety Authority and European Centre for Disease Prevention Control, 2016);
Hazard taken into consideration in a French Guide to good practice for hygiene and for the application of the HACCP principles, evaluated by Anses.
These filters correspond to significant foodborne hazards that are considered either by food safety authorities (at national or European level) or by food business operators.
Foodborne hazards satisfying at least one of these four filters were retained and resulting in a shorter list of “considered hazards.” For these hazards, the third stage was based on expert opinion. Some hazards were not retained, either because of a lack of data on their characterization and/or exposure (absence of epidemiological and contamination data, low pathogenicity) or because they were not considered relevant to the situation in mainland France (geographical distribution of the hazard, very minor foodborne transmission, the health status of the animal disease, etc.). The lists of “considered” or” retained” hazards were established according to the current state of scientific knowledge. The acquisition of new knowledge on one of these aspects could lead in the future to the inclusion of a hazard that is not currently included or conversely, to the exclusion of a hazard that is currently included. (Fig. 1).
Data collection and estimation of the foodborne diseases burden
The foodborne diseases burden in mainland France was assessed for the short list of considered hazards by combining the incidence and the severity (expressed in DALY) of the resulting diseases as done by Augustin et al. (Augustin et al., 2020).
The annual incidence data for the 2008–2013 period was taken from a study performed in France (Van Cauteren et al., 2017) and from surveillance data collected by the National Public Health Agency (Santé publique France) and by National Reference centers.
For the 2014–2019 period, the performance of the French disease surveillance system of each foodborne hazard was taken into account. Incidence was either provided directly from human surveillance data or corrected for under-reporting/under-diagnosis factors using the multipliers established by Van Cauteren et al. (2017) or expert opinion.
DALYs per case estimates for each pathogen were taken primarily from published studies (Cassini et al., 2018; Havelaar et al., 2015; Havelaar et al., 2012). For a given disease, the DALY summarizes the impact of disease morbidity (“Years Lost due to Disability” [YLD]) and mortality (“Years of Life Lost” [YLL]) in a single measure (Devleesschauwer et al., 2015).
The definition and the data sources for the criteria are detailed in Table 1.
Criteria for Risk Ranking of Biological Hazard
Risk ranking
Criteria
The health ranking of biological hazards is based on two macro-criteria representative of the two components of risk: The probability of occurrence of foodborne infectious diseases and the severity of the hazards (Codex Alimentarius Commission, 1999).
The probability of occurrence criterion is filled in by reference to annual incidence data for the period 2014–2019 (Table 1). The severity of the disease, associated to the hazard, is assessed using YLL and YLD (expressed as years per 1000 cases) (Table 1). These criteria, therefore, make it possible to account for disease-associated mortality and severity.
Aggregation of criteria: ELECTRE III
The choice of the multicriteria aggregation procedure is not straightforward (Guitouni and Martel, 1998). Outranking approaches appeared to be the most suitable as it is difficult to provide explicit compensation between the considered criteria. These methods can compare objects in pairs on each criterion using an outranking relationship. The aggregation of criteria was performed using the ELECTRE III method, one of the outranking methods. ELECTRE III explicitly takes into account indifference (q), preference (p), and veto (v) thresholds to make this comparison (see Supplementary Appendix S2). Thus, the ranking obtained reflects the decision-maker’s preferences. In our illustration, the working group served as a proxy for the actual decision-maker.
Below the indifference threshold, the decision-maker is not able to choose between the two interventions. Above the preference threshold, the decision-maker indicates a strict preference for one of the two interventions. These thresholds are established specifically for each criterion. The veto, above the preference threshold, illustrates that situations may be considered unacceptable by the risk manager who decides to disregard the other information. The working group did not identify any such situations for the exercise, so no veto thresholds were set for the criteria.
The values of the ELECTRE III model (weighting of criteria, preference, indifference and veto thresholds have been proposed by the working group to illustrate the approach. The indifference (q) and preference (p) threshold values proposed for the three criteria scales are shown in Table 2. The decision-maker may choose other thresholds. Two scenarios are considered for example.
Scenarios of Indifference (q) and Preference (p) Thresholds by Criterion
DALY, disability adjusted life years; YLD, years lost due to disability; YLL, years of life lost.
In the first one, the thresholds are set to 0, which means that any difference between two hazards compared on a criterion scale is considered significant.
In the second scenario, we consider, for mortality a difference of ten YLL per 1000 cases allows the decision-maker to distinguish between two hazards (p = 10). The preference and indifference thresholds are higher for YLD. Under a difference of 10 YLD, two hazards will not be considered as different (q = 10). A difference of more than 1000 YLD is required to prefer one hazard to the other. Finally, given the uncertainty in the estimates of disease incidence (Van Cauteren et al., 2017), a q value of 0.3 log10 cases per year (twice the number of cases) and a p value of 0.5 log10 cases per year (3.16 times the number of cases) have been used.
The relative importance of the criteria in the explanation of the risk is translated by the weights given to these criteria. It is up to the risk manager or decision-maker to set these weights. To illustrate the approach, three sets of weights are tested (Table 3) to test the influence of weighting on hazard rank. These weight sets were identified according to the Simos method (Roy and Figueira, 1998) described previously by Anses (Anses, 2020). This method derives weights from experts using three types of information: the order of the criteria, the spread of these criteria, and the order of importance between the most important criterion and the least important criterion.
Set of Different Weights Established for the Three Criteria for the Illustration
The first set of weights (A) corresponds to a situation in which the decision-maker wishes to give as much weight to incidence (50) as to severity (YLL and YLD, that is, 25 and 25). The set of weight (B) distinguishes within severity the impact of mortality (YLL) and morbidity (YLD) and gives greater weight to mortality. Finally, the set of weights (C) illustrates the choice to give more importance for decision-making to the severity of the disease associated with the hazard (YLL and YLD, 43 for each) than to the incidence of that disease (14).
Results
Hazards selection
From the long list containing 335 hazards, we obtained a list of 121 foodborne hazards including 47 bacteria, 13 viruses and Prions, and 61 parasites. After the application of the selection filters, the list of “considered hazards” contains 54 hazards. We decided to add histamine in this shorter list because its levels in food are regulated in the European Regulation 2073/2005 on microbiological criteria for foodstuffs. Among them, the expert panel did not retain 30 hazards (Supplementary Appendix S3). Thus, the final list of “retained hazards” consists of 24 hazards, including 12 bacteria (including bacterial toxins and metabolites), 3 viruses, and 9 parasites (Table 4).
Incidence and Severity (Years of Life Lost [YLL], Years Lost Due to Disability [YLD]) of Foodborne Illnesses in Mainland France
Van Cauteren et al., 2017.
Corrected surveillance data.
Surveillance data.
Expert opinions.
Dupouy-Camet et al., 2016.
Havelaar et al., 2012.
Cassini et al., 2018 (ECDC).
Havelaar et al., 2015 (FERG).
Foodborne diseases burden
Figure 2 illustrates the rank of pathogens in the health burden of biological hazards in mainland France. Salmonella and Campylobacter are the main contributors to the health burden. The ranks of the different hazards differ only slightly between the two considered periods, i.e., 2008–2013 and 2014–2019. Given the disease incidences estimation method, these variations may be due to actual differences in actual incidence or to changes in surveillance systems.
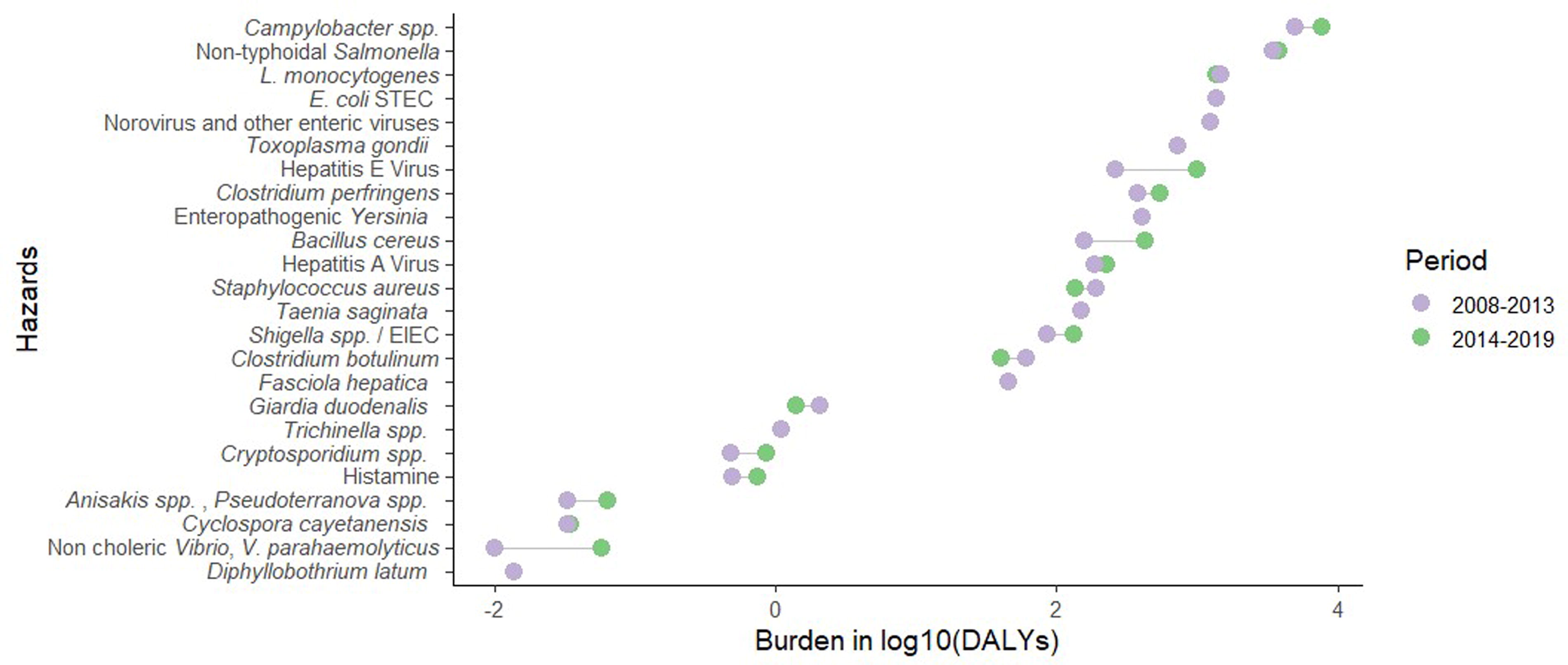
Rank of the different foodborne biological hazards according to the burden of diseases expressed in DALYs for two periods. DALY, Disability Adjusted Life Years.
Figure 3 illustrates the association between foodborne pathogens in 2019. Bacteria account for 81.5% of the foodborne burden. Within bacteria, non-typhoidal Salmonella and Campylobacter contribute to 66% of the burden. Foodborne viruses account for 11.6% of the burden, whereas parasites are associated with 6.9%.

Sunburst diagram showing the repartition of the foodborne burden of diseases (FBD) (expressed in DALY) in 2019 according to types and sub-categories of biological hazards. DALY, Disability Adjusted Life Years.
Ranking with ELECTRE III method
The rankings of the 24 foodborne biohazards using the outranking method are presented in Figure 4, which shows the impact of the weights for the three criteria on the ranking. The MCDA method defined equivalents between the different hazards. Thus, 11, 10, and 15 different ranks were, respectively, obtained with the scenario 2 thresholds for the sets of weights A, B, and C (Fig. 4). It is noted that the threshold scenario 1 leads, as expected, to more equivalents, and thus fewer hazard groups. For example, the number of groups for set (C) of weight decreases from 15 to 12 groups while using scenarios 2 and 1, respectively.
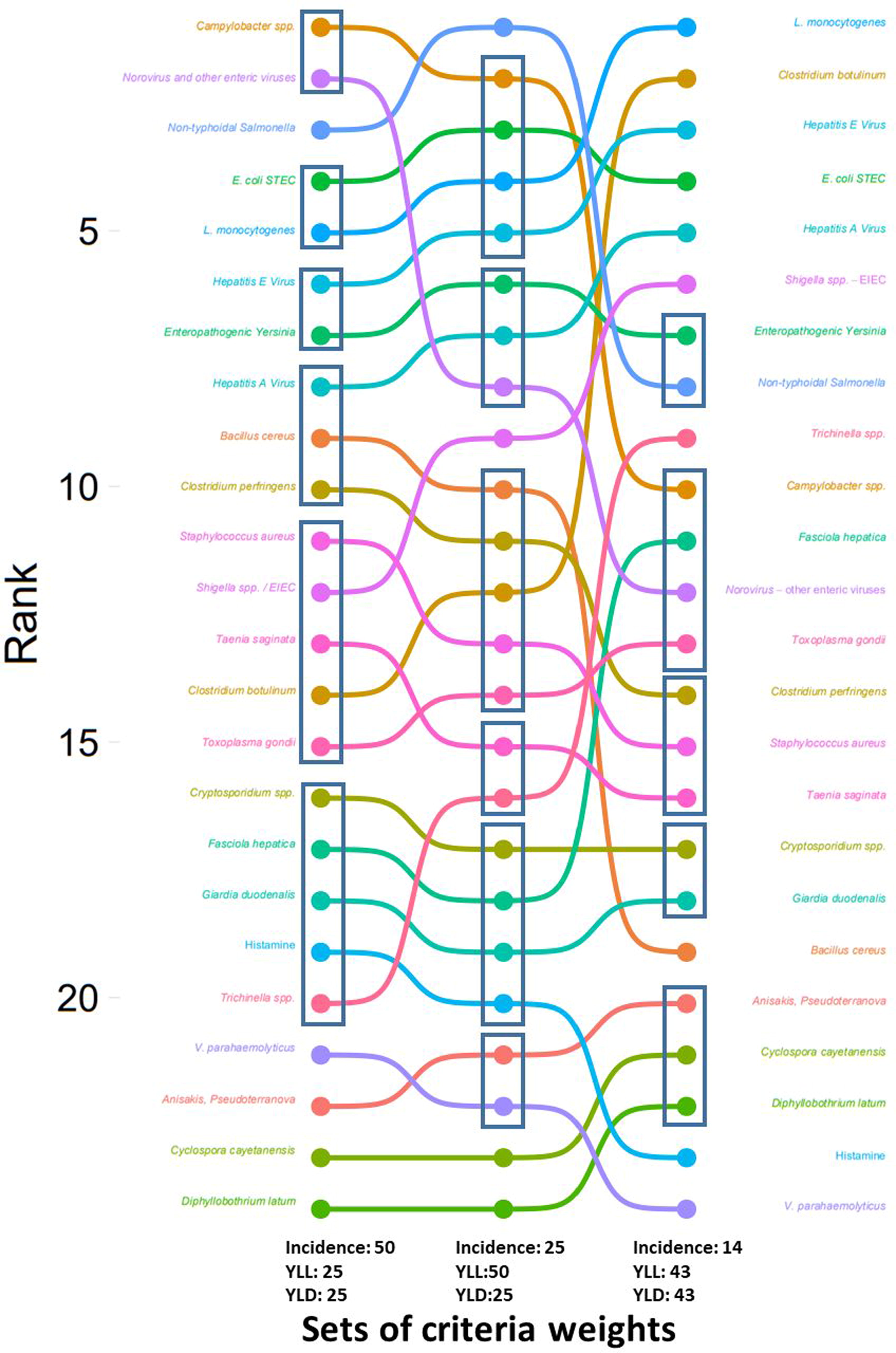
Prioritizations of food-borne biological hazards obtained with the three sets of weights given to the three criteria (number of cases/value of YLL/value of YLD) (Table 3). Boxed hazards have equivalent ranks. The ranks were obtained with scenario 2 values of indifference
Some hazards are minimally impacted. For example, histamine and Cyclospora cayetanensis still have the lowest level of risk regardless of the weighting of the three criteria. This is explained by the fact that these hazards are not very severe and present few cases in France. Other hazards are strongly affected by the weight. As an example, Clostridium botulinum is 14th out of 24 for the weight set A and 2nd for the weight set (C). These ranking examples are presented as an illustration of the method; the choice of weights is ultimately up to the risk manager.
Discussion
This work introduces a transparent methodology to identify relevant foodborne biological hazards and proposes an assessment of their health burden in mainland France. It also paves the way for prioritization by the risk manager based on the determinants of the burden and a multicriteria method that allows the weights of the risk components to be objectively defined and the rankings to reflect the preferences of decision makers.
It is important to note that the selection of hazards results from the application of filters related to food safety. For this, we tried to remain consistent with the international definition of a foodborne hazard and with the target geographical perimeter, namely mainland France. The selection of hazards could certainly be different in another territory. In the same way, the evolution of scientific knowledge on hazards, the acquisition of new data, the emergence of hazards and/or a health crisis could also modify the selection. Similarly, the globalization of trade and markets, and climate change are elements likely to modify the lists of hazards (Feliciano et al., 2020). Indeed, it seems necessary to regularly update and refresh the selections in light of appropriate scientific monitoring. Thus, for example, the rationale for excluding tick-borne encephalitis virus (TBEV) (see Supplementary Appendix S4) from the retained hazards list because of the exceptional nature of foodborne transmission in France may now be reconsidered in the light of recent cases of foodborne transmission in France (Gonzalez et al., 2022; Mailles et al., 2023). More data are needed on the geographical distribution and the incidence of foodborne cases in France. The same observation and reasoning can also be made with Clonorchis sinensis/Opisthorchis spp. whose involvement in foodborne outbreaks in some Western European countries must constitute a warning worth monitoring (Pozio et al., 2013; Robertson, 2018).
We estimated that foodborne diseases caused by 24 biological hazards in mainland France resulted in 17,057 DALYs between 2008 and 2013 and 21,181 DALYs between 2014 and 2019. Norovirus caused the most illnesses but Campylobacter and Salmonella represent the highest foodborne disease burden. These estimates are in line with our previous study using a semi-quantitative approach (Augustin et al., 2020). Similar findings have been reported by other industrialized countries (Havelaar et al., 2015) and in particular recent studies from Denmark (Pires et al., 2020) and the Netherlands (Lagerweij et al., 2020).
The foodborne disease burden was estimated according to a top–down approach, using epidemiological data. The main advantage is that it directly measures outcomes and impacts of interest to public health. The main drawbacks are that surveillance data remain incomplete (Van Cauteren et al., 2017), depending on the effectiveness of epidemiological information collection.
For the 2008–2013 period, the incidence estimates used in this study are mainly derived from a French study conducted by the National Public Health Agency (Van Cauteren et al., 2017). In this study, different approaches have been used to estimate the incidence of illness depending on the data available for each hazard (direct estimation, “pyramidal approach,” syndrome data scaled down). For the 2014–2019 period, we applied the same corrective factors established in this study to estimate the incidence of illnesses from the surveillance data. The underlying assumption is that the surveillance system did not change during the last period. However, the uncertainty of the epidemiological data is considered in the confidence score for the ranking. As there is no French study estimating the severity of foodborne diseases, different international sources of data were used to estimate YLL and YLD (see Material and Methods). Further research is needed to obtain specific DALY estimates for France.
According to our results, there is no meaningful evolution in the number of illnesses related to foodborne pathogens between the two periods studied. For most foodborne diseases, the estimated incidence falls within the credible interval of previous estimates by Van Cauteren et al. 2017.The observed changes for Campylobacter and Bacillus cereus are not significant between these two periods, due to the many sources of uncertainty. Concerning hepatitis E, the availability of diagnostic tests and better knowledge of hepatitis E have led to a considerable increase in the number of people tested since 2010, resulting in an increased incidence of recorded cases (Couturier et al., 2018).
In order to prioritize the management of foodborne hazards, the burden factors are considered as criteria in a MCDA model. The advantage of not aggregating the two criteria YLL and YLD responds to the criticism sometimes leveled at the DALY. For some authors, it is more an evaluative measure than a purely descriptive one (Solberg et al. 2020).
The choice of this approach is consistent with the review of methods for prioritizing biological, chemical and nutritional risks related to food on the basis of public health risk (Van der Fels-Klerx et al., 2018). The authors in the study of Van der Fels-Klerx et al. (2018) highlight the value of MCDA approach for comparing a large number of objects by integrating qualitative and quantitative data, the uncertainty associated with this data and the decision preferences of managers. This is also the approach adopted by Eygue et al (2020) to rank biological and chemical risks in food. Their risk-ranking framework includes eight criteria also related to the severity and the likelihood. The authors use the PROMETHEE outranking method, which is broadly based on the same principles as ELECTRE III method, that is, the use of preference and indifference thresholds and on the upgrading relationship. The application of the different methods to the ranking of alternatives may lead to different results. The inconsistencies, often minor (Kangas et al., 2001), are due to differences in both the preference estimation process and the calculation techniques. This makes it difficult to identify the best method among the available upgrading methods (Garre et al., 2020; Polatidis et al., 2014). The advantage of the ELECTRE III method lies in the use of a “veto threshold.” In the field of health risk management, the veto threshold is legitimized by the fact that the risk manager may deem some situations unacceptable. The proof of concept shows the decisive impact of the parameters of the ELECTRE III method (sets of weights and preference and indifference thresholds applied to the criteria) on the ranks obtained. For the purposes of the exercise, we arbitrarily defined the value of these parameters. However, it is essential that these values are established by the risk manager using a formalized approach. It should be noted that the manager can adjust the weights of the criteria according to the objectives of the ranking.
Conclusions
In response to a formal request from the French Risk Managers, we have developed a multicriteria approach to rank food-related biological risks based on the severity and incidence of hazards in order to help the manager to prioritize them. The risk manager still has some work to do in order to propose a ranking of biological food hazards that matches his or her vision of priorities. This work should make it possible to identify two main elements: what are the relative values of the number of cases and the severity criteria, and at what point do we consider that management should be different (p and q values)?
This approach is not limited to biological risks alone, as we have also applied it to chemical risks and to food-hazard combinations (Anses, 2020) with the aim of moving toward integrated food safety management. Although we initially chose the ranking criteria based on the Codex Alimentarius definition of risk, the MCDA approach makes it possible to add criteria of another nature, in particular socioeconomic criteria, in order to go further in the objectification and transparency of the decision-making process.
Footnotes
Acknowledgment
The Anses Working Group on Prioritization of food risks included the coauthors F.A.P., L.G., J.C.A., G.B., M.F., M.G., R.P., M.M., M.S., P.K., as well as (in alphabetical order) Sophie ALLAIN, Nathalie ARNICH, Nawel BEMRAH, Estelle CHAIX, Nicole HAGEN-PICARD, Laïla LAKHAL, Mathias LUNGHI, Eric MARCHIONI, Gilles RIVIERE, Brigitte ROUDAUT, Louis-Georges SOLER, Bruno TESTE.
Disclosure Statement
The authors declare no conflict of interest.
Authors’ Contributions
Conceptualization: F.A.P., L.G., P.K., M.F., and M.S. Methodology, investigation and formal analysis: All authors. Data curation: F.A.P., L.G., and P.K. Writing—original draft preparation: F.A.P., L.G., M.F., and P.K. Writing—review and editing: G.B., J.C.A., M.G., N.J.D.S., M.M., R.P., and M.S. Visualization: F.A.P., L.G., and P.K. All authors have read and agreed to the published version of the article.
Funding Information
This research received no external funding.
Supplementary Material
Supplementary Appendix S1
Supplementary Appendix S2
Supplementary Appendix S3
Supplementary Appendix S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.