
Abstract
Listeriosis is a relatively rare but severe foodborne disease, which has significant public health concern of persons with underlying conditions and pregnant women. This study aimed to estimate the morbidity, mortality, and fatality rates of listeriosis over a 10-year period and clarify the epidemiological features of the pathogen in Beijing, China, based on voluntary reporting of sentinel surveillance. A total of 228 listeriosis cases were reported with annual morbidity rate of 1.054 per million inhabitants, including 113 maternal-neonatal cases with mean annual morbidity rate of 63.401 per million live births in Beijing from 2013 to 2022.The morbidity rate increased from 0.094 to 0.868 per million inhabitants from 2013 to 2019 (p for trend = 0.003). The overall and maternal-neonatal fatality rate were 31.82% and 42.86%, respectively. Four serogroups were identified in this study, and 1/2b predominated (89 strains). We observed the morbidity rate of listeriosis increased in Beijing over the past 10 years. Maternal-neonatal cases accounted for a higher proportion than that described in other countries, considering population base and fertility policy in China, official recommendations targeting pregnant women should be actively promoted.
Introduction
Listeriosis, which is caused by Listeria monocytogenes, is recognized as a relatively rare but severe foodborne disease (Rocourt and Bille, 1997; Li et al., 2018). Incidence of listeriosis is estimated to be three to six cases per 1 million persons per year globally (de Noordhout et al., 2014). Although infection is rare, it is a significant contributor to deaths caused by foodborne infections with a high fatality rate of 20–50% (Scobie et al., 2019; Arslan et al., 2015; Goulet et al., 2012; Pelegrín et al., 2014; Huang et al., 2023). Listeriosis is typically associated with certain populations who have weakened immune systems including pregnant women and their fetuses, neonates, elderly people, immunocompromised patients, and patients with underlying comorbidities such as diabetes mellitus and cancer (Friesema et al., 2015; Maertens de Noordhout et al., 2016). Infection with L. monocytogenes in these vulnerable groups can lead to serious clinical presentations including septicemia and central nervous system (CNS) infections, which can be fatal and also lead to adverse pregnancy outcomes including abortion, stillbirth, and neonatal infection (Koopmans et al., 2023; Tran et al., 2023).
In contrast to most other foodborne pathogens, L. monocytogenes is able to grow in food at refrigerated temperatures (Razavilar and Genigeorgis, 1998). Due to the ability to continuously grow and reproduce in a food, it is difficult to control L. monocytogenes in food preparation and production environments (Havelaar et al., 2010). Listeriosis is predominantly transmitted to humans through the consumption of contaminated food products with a high foodborne proportion of up to 99% (Scallan et al., 2011). Continuous surveillance of the epidemiological changes is significant for the prevention and treatment of listeriosis. However, the important impact that this disease has on public health is not always recognized by contrast with many other foodborne infections such as salmonellosis (Garrido et al., 2008). Most cases have been reported in high-income countries. Listeria monocytogenes has become the third most costly foodborne pathogen in the United States (Whitham et al., 2022), with an annual incidence of about 1600 infections (Crim et al., 2015). A total of 2183 confirmed cases were reported in the European Union in 2021 (ECDC and EFSA, 2022).
Unlike European countries and American countries, listeriosis is likely to be under-reported in China due to its status as a non-notifiable disease. During 2013–2017, a total of 211 listeriosis cases were reported with 138 (65.4%) perinatal cases (Li et al., 2019). Listeriosis sporadic case surveillance was included in the national surveillance plan in 2013 in some limited provinces, and Beijing is one of the first municipalities to carry out a surveillance plan. Most studies on the incidence and epidemiological features of listeriosis in China are case reports or literature reviews until now (Wang et al., 2013; Fan et al., 2019; Feng et al., 2013), a comprehensive analysis using long-term continuous surveillance data to understand the secular trend of listeriosis is lacking. Therefore, we investigated the morbidity, mortality, fatality rates, and epidemiological features of clinical invasive listeriosis from sentinel surveillance over 10 years in Beijing, China. This study filled the missing data of listeriosis surveillance to better estimate the epidemiological features and understand the genetic characteristics of L. monocytogenes in Beijing.
Methods
Surveillance of listeriosis in Beijing
Beijing Municipal Health Commission launched the Surveillance Project of Human Listeriosis in 2013. Hospitals that have diagnosability and ability to treat foodborne diseases should report laboratory-confirmed cases of listeriosis. The protocol of our study was approved by the ethics committee at Beijing Center for Disease Prevention and Control. We enrolled cases of listeriosis reported from 46 hospitals between January 1, 2013 and December 31, 2022. All samples were collected by sentinel hospitals, and L. monocytogenes were isolated in the microbiology laboratory.
Case definition
Surveillance cases of listeriosis are defined as a patient in whom the isolation of L. monocytogenes was from a usually sterile site, for example, blood or cerebrospinal fluid and with tentatively diagnosed with CNS infection, acute gastroenteritis, skin-soft tissue infection, septicemia, chorioritis, and intrauterine infection. Cases are classified as maternal-neonatal associated infection and non-maternal-neonatal associated patients. Maternal-neonatal cases included maternal-fetal patients and neonatal patients whose bio-specimens were positive for L. monocytogenes. When L. monocytogenes was isolated from samples of both mother and her newborn or fetus, the pair event was considered as a single case, and we describe the clinical features of the mothers (Charlier et al., 2017). Non-maternal-neonatal cases were defined as patients >28 days of age when L. monocytogenes was isolated from blood culture and Cerebrospinal fluid (CSF) (Li et al., 2019). A standardized surveillance questionnaire was used to collect data on socio-demographic information, clinical symptoms, diagnosis, pregnancy-related information, comorbidities (immunosuppressive treatment or underlying disease), food history within the 30 days prior to the onset of illness and outcome of the patients (death, recovery or censor) when discharged from hospitals.
Laboratory isolate characterization
All L. monocytogenes were isolated by microbiology laboratories in sentinel hospitals. A matrix-assisted laser desorption/ionization time of flight mass spectrometry (Bruker, Leipzig, Germany, Microflex LT) was used to identify L. monocytogenes isolates in the Beijing CDC laboratory. Multiplex Polymerase Chain Reaction (PCR) assay was performed for L. monocytogenes serotype (Doumith et al., 2004). Multilocus Sequence Typing (MLST) analysis was performed by sequencing seven housekeeping genes. The alleles and sequences types (STs) were determined by submitting the allelic profiles of L. monocytogenes to the MLST database at the Pasteur Institute, France (https://www.pasteur.fr/mlst).
Statistical analysis
Morbidity, mortality, and fatality rate were the outcomes of interest. This study assumed that the admission rate of patients with listeriosis was 100%, namely, the number of inpatients with listeriosis reported by sentinel hospitals represents the number of listeriosis cases. Data of the resident population were from the National Bureau of Statistics of China between 2013 and 2022. We calculated morbidity, mortality, and fatality rate of calendar year, also fatality rate of different epidemiological characteristics. We performed exact binomial test to estimate 95% confidence interval (CI) of these rates and the Mann–Kendall trend test to analyze the increasing or decreasing trend. Pearson χ2 test and Mann–Whitney U test were used to test the difference between the groups. All tests were two-tailed, and a p-value of ≤0.05 indicated statistical significance. We used R software version 4.1.2 (https://www.r-project.org/) to analyze the data.
Results
Morbidity and mortality rates of listeriosis cases
A total of 228 listeriosis cases were reported in Beijing between January 1, 2013 and December 31, 2022, including 113 maternal-neonatal cases (49.56%) and 115 non-maternal-neonatal cases (50.44%) (Fig. 1). One hundred and thirteen maternal-neonatal cases included 18 (15.93%) neonatal cases (neonatal infection without maternal infection) and 95 maternal cases (maternal infection with or without neonatal or fetal infection). We did not identify outbreaks during the study period. All cases were hospitalized. The mean annual morbidity rate was 1.054 (95% CI: 1.053–1.056) per million inhabitants, increasing from 0.094 (95% CI: 0.093–0.095) per million in 2013 to 2.557 (95% CI: 2.555–2.559) per million in 2019 (p for trend = 0.003). The mean annual maternal-neonatal morbidity rate was 63.401 (95% CI: 31.650–113.438) per million live births, increasing from 10.695 (95% CI: 1.295–38.634) per million in 2013 to 177.143 (95% CI: 120.363–251.431) per million in 2019 (p for trend = 0.003). The number of reported death cases ranged from 0 to 6 cases per year and the mean annual mortality rate per million population was 0.091 (95% CI: 0.090–0.092). The mean annual maternal-neonatal mortality rate was 11.527 (95% CI: 1.396–41.640) per million live births, decreased from 10.695 (95% CI: 1.295–38.634) per million in 2013 to 0 in 2022 (p for trend = 0.016) (Fig. 2).

Flow chart of listeriosis cases selection.
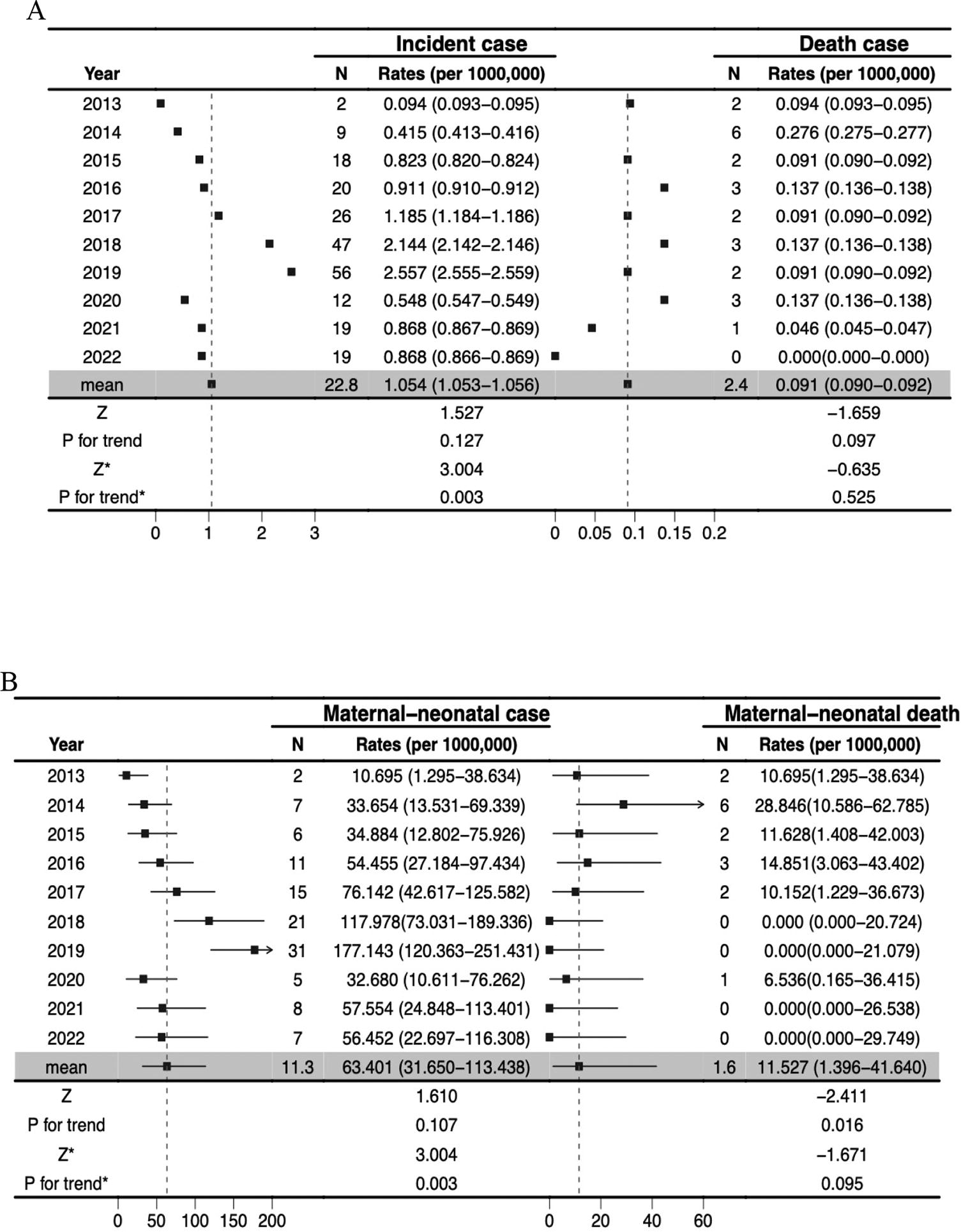
Forest plot of morbidity and mortality rates of listeriosis cases in Beijing, China, 2013–2022.
Fatality rates of listeriosis cases
Overall, 112 (99.12%) of 113 maternal-neonatal cases and 64 (55.65%) of 115 non-maternal-neonatal cases documented the outcomes when they were discharged from the hospital in the years under study. The total fatality rate is estimated at 31.82% (95% CI: 25.01–39.25%), and the mean annual fatality rate was 33.33% (95% CI: 13.34–59.01%) (Supplementary Figure S2). Among 112 maternal-neonatal cases, 42.86% (95% CI: 33.55–52.55%) of them resulted in abortion (n = 19), stillbirth (n = 24), or infant death within 24–48 h of birth (n = 5). The mean annual fatality rate was 45.45% (95% CI: 16.75–76.62%) in maternal-neonatal cases. Table 1 summarizes fatality rates in different socio-demographic features and clinical and microbiological characteristics of the 176 listeriosis cases that reported outcomes. The fatality rate of maternal-neonatal cases with less than or equal to 28 weeks of gestation is significantly higher than that with more than 28 weeks of gestation (p < 0.001).
Fatality Rates of Listeriosis Cases, Maternal-Neonatal Cases, and Non-Maternal-Neonatal Cases in Beijing, China, 2013–2022

CI, confidence interval; CNS, central nervous system.
Epidemiological features of listeriosis cases
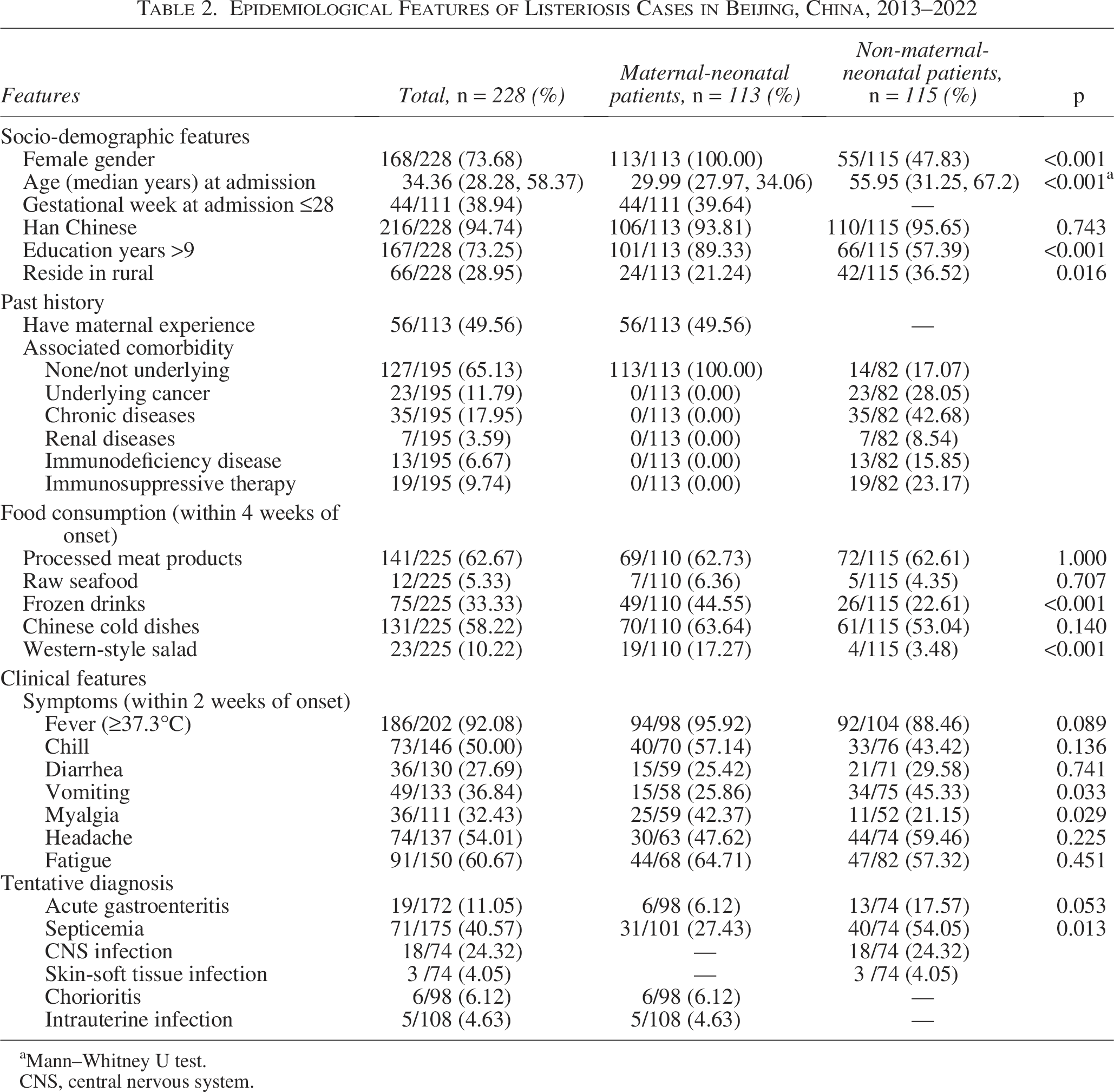
One hundred and fifteen non-maternal-neonatal listeriosis cases were documented during the study period, including 40 cases of septicemia, 18 cases of CNS infection, 13 cases of acute gastroenteritis, and 3 cases of skin-soft tissue infection. Patients older than 60 years accounted for 41.73% (48/115). The most frequent immunosuppressive comorbidities in non-maternal-neonatal patients were chronic diseases (including diabetes, hypertension, and cardiopathy) (35, 42.68%) and underlying cancer (23, 28.05%). Fourteen (17.07%) patients reported without ongoing comorbidities: 85.71% (12/14) of them were younger than 50 years, and had no report of substantial infection before listeriosis (Table 2).
Epidemiological Features of Listeriosis Cases in Beijing, China, 2013–2022
Mann–Whitney U test.
CNS, central nervous system.
Serotyping characteristics
Amniotic fluid and blood were the most sensitive samples for microbiological diagnosis. For non-maternal patients, 65 (98%) and 16 (76%) were positive in blood and CSF cultures, respectively (Supplementary Table S3). Four serovars were determined among the 228 clinical isolates (Table 3). Serotype 1/2b (89, 39.04%) was the most common infecting serogroup of strains, where serotyping was performed (188/228, 82.46%).
Characteristic of Listeria monocytogenes Strains Isolated from Cases of Listeriosis in Beijing, China, 2013–2022
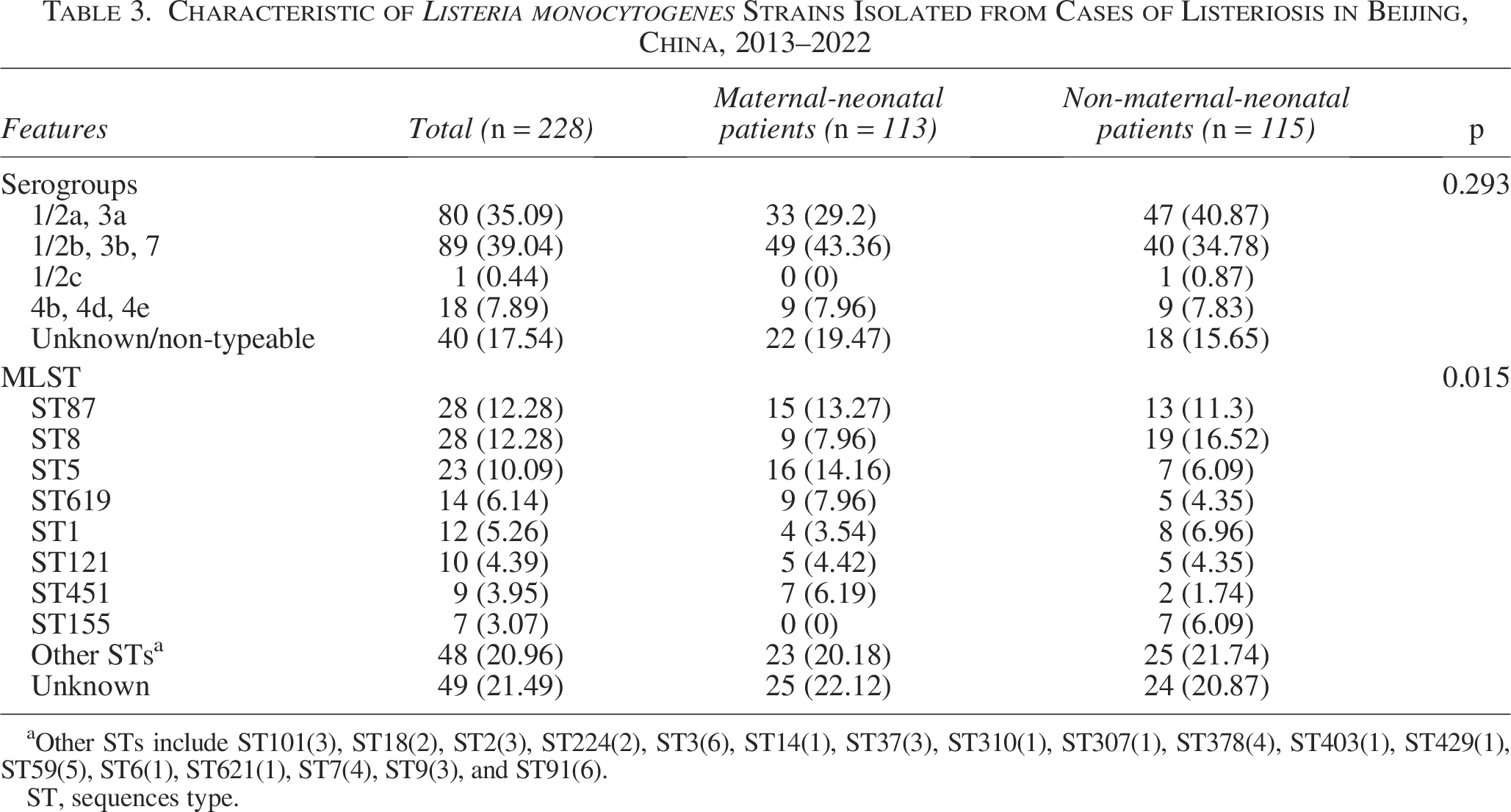
Other STs include ST101(3), ST18(2), ST2(3), ST224(2), ST3(6), ST14(1), ST37(3), ST310(1), ST307(1), ST378(4), ST403(1), ST429(1), ST59(5), ST6(1), ST621(1), ST7(4), ST9(3), and ST91(6).
ST, sequences type.
The prevalence of serogroups in the study period is shown in Supplementary Figure S1. The number of listeriosis cases caused by serotype 1/2b regularly increased from 1 in 2013 to 23 in 2019. The proportion of serotype 1/2b varied between 35.29% and 100.00% and that of serotype 1/2a between 35.29% and 52.94%. By MLST, the strains were distinguished into 26 individual sequence types. ST8 and ST87 were the predominant (28, 12.28%) STs, followed by ST5 (23, 10.09%). ST5 was the predominant MLST in maternal patients, while ST8 was the predominant ST in non-maternal patients.
Discussion
We estimate the morbidity and mortality of listeriosis and clarify the epidemiological characteristics of the pathogen in Beijing based on information from voluntary reporting of sentinel surveillance. The morbidity rate of listeriosis increased in Beijing over the past 10 years under our study, but it still is lower than that in the United States and the European Union (Ray et al., 2021; ECDC and EFSA, 2022). And maternal-neonatal cases account for a much higher proportion than is usually described in China, which highlights the need to focus more efforts on the prevention of listeriosis in pregnant women. We observed that 1/2a and ST87 (ST8) were the dominant serotype and MLST of isolated L. monocytogenes strain. This study has provided useful evidence for the estimation of listeriosis burden and will enable listeriosis to be included in country prioritization exercises.
We found the annual incident rate (0.11/100,000) in Beijing was lower than that in New Zealand (0.70/100,000) (Jeffs et al., 2020). Listeriosis has not been included in the notifiable disease lists in our country and the missed diagnosis and missing report in the passive sentinel surveillance may be the reason for the lower incidence obtained in Beijing. There was no national clinical listeriosis surveillance in Beijing until 2013, but many journals have published listeriosis case reports (Li et al., 2019). One systematic review was conducted to retrieve articles from 1963 to 2010, and the results showed that there were 147 patients with listeriosis in China (Feng et al., 2013).
Taking into account the impact of COVID-19 on the conduct of listeriosis surveillance, we analyzed trends in rates from 2013 to 2019 and found an overall increasing trend in morbidity of both the whole population and maternal-neonatal population. While the notification rate of listeriosis has remained stable in European countries during the same period (ECDC and EFSA, 2022). So, the increase in the number of cases in recent years can be considered as the increased reporting awareness of doctors and the increase in the number of sentinel hospitals. In addition, we found an overall decreasing trend in mortality rates over the study period in keeping with findings from previous reviews (Scobie et al., 2019; Bennion et al., 2008). The overall fatality rate is similar to that described in other report (23.78%) (Fan et al., 2019).
Pregnant women are at high risk of listeriosis, approximately 12–20 times more prevalent than in the general population, resulting in a maternal, fetal, or live-born neonatal infection (Girard et al., 2014; Elinav et al., 2014). The morbidity of maternal-neonatal case in Beijing is 60 times more common than that in the general population and is nearly two times higher than that in the United States (Pohl et al., 2019). In a contrast, the incidence of pregnancy-associated listeriosis in Ningbo women and children’s hospitals was 16.69/100,000 births, which is much higher than our results (Ke et al., 2022). Considering we included an investigation of tissue samples obtained from hospitalized women after miscarriage, the perinatal incidence could also be higher due to undiagnosed spontaneous abortions and stillbirths. Our study shows that the proportion of maternal-neonatal listeriosis cases in Beijing was much higher compared with other countries (Garrido et al., 2008; Awofisayo et al., 2015; Jackson et al., 2010; Filipello et al., 2017; Charlier et al., 2017; Elinav et al., 2014). An unexpectedly higher incidence of listeriosis in Asian-origin mothers than that in other ethnics was reported in New Zealand, which is most likely associated with differences in food consumption habits in this population, for example, fresh fish, shellfish, and pre-prepared foods (Jeffs et al., 2020). Strategies should be in place to prevent maternal-neonatal listeriosis in those with predisposing factors.
By contrast, the maternal-neonatal fatality rate is similar to the rate reported by Spain (45%) but much higher than previously reported in China (10.6% and 26.4%) (Li et al., 2018; Garrido et al., 2008; Lu et al., 2021). However, a prospective study indicated that 83% of infected mothers in France experienced major fetal or neonatal complications, which is worse than what has been estimated in retrospective studies (Charlier et al., 2017). Furthermore, the decreasing fatality rates may reflect improvements in the identification of high-risk foods and in the efficient treatment and clinical management over the past 10 years. Consistent with the results of a prospective study, we found fetal losses occurred more often at less than 29 weeks of gestation in maternal-neonatal cases. Given the limited number of cases and the unavailability of some clinical information, we fail to clarify the difference in case fatality rate among different serogroups, the presence of underlying conditions, which had been identified in previous research (Scobie et al., 2019; Maertens de Noordhout et al., 2016; Charlier et al., 2017).
The non-maternal-neonatal fatality rate was lower than the reported in reviews in China (23.78%), England (28.7%), and Denmark (27%) (Li et al., 2018; Jensen et al., 2016; Scobie et al., 2019). The main comorbidities were chronic diseases and cancer in agreement with those observed in previous studies (Friesema et al., 2015; Wang et al., 2013). Despite most non-maternal-neonatal listeriosis are people with comorbidities, the study also indicated that L. monocytogenes can infect people without underlying diseases, which could be accounted for inherited susceptibility to listeriosis (Charlier et al., 2017). The most common clinical manifestation of non-maternal-neonatal cases was septicemia, followed by CNS infection, which is similar to cases from 2011 to 2017 in China and England (Fan et al., 2019; Scobie et al., 2019).
In line with the results of studies in China, our results confirm the fact that the most frequent serotypes identified in human listeriosis were 1/2a, 1/2b, and 4b (Zhang et al., 2013; Wang et al., 2015; Lu et al., 2021; Zhang et al., 2019). Whereas, we found the predominant serogroup of clinical L. monocytogenes strains in Beijing was different from those reported serotype 4b being the preponderance of serogroup from other countries including England, Australia, Brazil, Japan, and Spain (Almeida et al., 2017; Jennison et al., 2017; Garrido et al., 2008; Scobie et al., 2019; Baba et al., 2021) (Supplementary Tables S4). By contrast, some studies observed serotype 1/2a as the leading serotype causing human infections (Mammina et al., 2013; Lukinmaa et al., 2003; Lopez-Valladares G et al., 2018).
It is widely accepted that food is the source of human L. monocytogenes. The average prevalence of L. monocytogenes in Chinese food products was 4.42% (Li et al., 2018). However, there was a slight difference in prevalence of STs between human isolates and foodborne isolates. The most predominant sequence types were ST87 and ST8 from human isolates, while the most predominant sequence types were ST9 from pork and ST8 and ST87 from aquatic products in China (Yin et al., 2020; Chen et al., 2018).
Nevertheless, ST87 is seldom linked to human infections in other countries such as Austria and Switzerland (Althaus et al., 2014; Cabal et al., 2019). ST5 is the most prevalent ST type in maternal-neonatal patients, and studies have shown that ST5 in maternal-neonatal cases is more likely to result in fetal loss compared with ST87 (Zhang et al., 2019). Due to their own characteristics, some types may not be widely spread, and there are differences in the types of circulating food, production links, processing technology, and eating habits between different regions, resulting in relatively unique STs in different regions (Supplementary Tables S5). The study using Whole Genome Sequencing (WGS) revealed the discovery of a new genomic island of L. monocytogenes (LGI-2) with a wide diversity of strains in China (Zhang et al., 2016).
Strengths and Limitations
Since notification of listeriosis is not mandatory in China and this case information comes from voluntary reporting from sentinel surveillance, there are many under-reporting and under-diagnosis of listeriosis cases. When it comes to mortality and fatality analysis, non-maternal-neonatal patients who were lacking of outcomes were failed to be included. The outcome was not captured at a defined time point following infection but at the time of data entry following receipt of completed questionnaires. This limitation suggests that the actual rates of listeriosis might be higher than reported here.
Conclusion
In conclusion, the present study observed the morbidity rates of listeriosis increased in Beijing over the past 10 years, but it still is lower than that in other countries, indicating that better harmonization of data collection systems is required to assess the burden of listeriosis. Obligatory notification of listeriosis, application of a standardized food, and clinical questionnaire would be valuable in all diagnosed or suspected listeriosis. Besides, maternal-neonatal cases account for a much higher proportion than is usually described in China. Considering the large population base and national fertility policy, official recommendations (food hygiene and avoidance of at-risk food) targeting pregnant women should be actively promoted.
Authors’ Contributions
T.W., Y.N., and J.J. were involved in the collection of clinical data. X.Z., P.Z., and Y.L. performed the molecular subtyping tests. T.W., C.W., and Y.W. performed the data analysis. X.M., T.G., W.L., and L.W. designed the study, drafted, and revised this article.
Footnotes
Acknowledgment
Funding Information
This work was supported by
Data Availability Statement
The data are not publicly available due to the containing information that could compromise the privacy of research participants.
Ethical Statements
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Disclosure Statement
No competing financial interests exist.