
Abstract
Purpose:
We performed a literature review focusing on case reports and case series studies, aiming to better define the clinical presentation of isolated lateral intraventricular neurocysticercosis (LVNCC) and to discuss the current knowledge of its characteristics, patient demographics, clinical manifestations, treatment, and prognosis, based on the collected data.
Methods:
Data for this study were gathered by conducting searches on the Medline database and Google Scholar using various combinations of the following terms “intraventricular neurocysticercosis (IVNCC),” “brain ventricle cyst,” “cysticercosis of lateral brain ventricles,” “cysticercus cyst in brain ventricles,” and “intraventricular cystic brain lesion.” Articles published in English between January 1980 and March 2023 that reported cases of LVNCC were selected for analysis.
Results:
This study included 48 patients (mean age 33.1 ± 14.1, range 6–70 years) diagnosed with LVNCC. Most patients were from India. The predominant clinical manifestation was headache (87.8%), followed by nausea/vomiting (51.2%), altered sensorium (51.2%), and focal neurological deficits (29.3%). In most cases, symptoms lasted from 10 d to 20 years (67.6%). The mean age at symptom onset was higher than in those with cysts in the third and fourth ventricles (p = 0.010058), and a greater proportion of vesicular cysts was observed (58.3%). Hydrocephalus was common (81.3%), with a significant percentage showing unilateral ventricular enlargement (38.5%). Surgical excision of the parasite (predominantly endoscopic) was the prevailing type of treatment (72.9%). Postoperatively, anti-helminthics were administered in 37.5% of cases. Most patients (80.5%) had favorable clinical outcomes or improved clinical status; six patients died, while the clinical outcomes of seven individuals were not specified in reports.
Conclusion:
LVNCC is a rare form of NCC, typically characterized by symptoms lasting >7 d. Invasion of the ventricle by cysticerci occurs mainly in middle-aged individuals. Endoscopy is the preferred treatment option, although the prognosis is influenced by various factors. Mortality is high in untreated patients.
Introduction
Human neurocysticercosis (NCC), caused by the larval stage of the cestode parasite Taenia solium, is a neglected tropical disease, recognized by the World Health Organization as the leading preventable cause of acquired epilepsy in the developing world since 2010 (Guarda et al., 2018). From clinical, immunological, and therapeutic perspectives, there are two distinct entities: parenchymal NCC and extra-parenchymal NCC (intraventricular and subarachnoid) (Garcia, 2018).
Intraventricular neurocysticercosis (IVNCC), a rare form of NCC, has been studied by many clinicians. Some researchers conveyed their findings through review studies, focusing on various aspects such as demographics, clinical presentation, diagnosis, and treatment options (Sinha and Sharma, 2012; Jensen and Post, 2016; Yamaki et al., 2023). Others shared their experiences through detailed case reports, providing insights into different facets of intraventricular disease (Gupta et al., 2015; Shang et al., 2015; Bahtiar and Wijanarko, 2018).
The lateral ventricle (LV), as one of the possible locations of NCC, has several unique features that set it apart from other brain cavities. As the largest and bilaterally symmetrical ventricle in the brain, the LV has several anatomical features that can be significant during surgical approaches to ventricular lesions (Le Gars et al., 2009). It communicates with the third ventricle (TV) through the foramen of Monro (Scelsi et al., 2020).
Cysticerci infestation typically begins in the choroid plexus of the LV. The cyst can migrate further into the other ventricles to the basal subarachnoid space (Proaño et al., 2009), or it may adhere to the choroid plexus or the ventricular wall (Del Brutto, 2018). A growing cyst can obstruct the ventricular openings (the foramen of Monro, the cerebral aqueduct, the foramina of Luschka and Magendie), leading to unilateral or total acute hydrocephalus. A degenerating parasite can trigger an inflammatory reaction (acute or chronic granular ependymitis), causing partial or complete blockage of cerebrospinal fluid (CSF) flow, ventricular enlargement, periventricular inflammation, and, in severe cases, a “locked ventricle” that may result in herniation (Colli et al., 1993; Nash et al., 2018). A degenerative cyst in the basal subarachnoid space can induce an inflammatory response, leading to meningitis (arachnoiditis) and vasculitis (García and Del Brutto, 2003).
The prevalence of lateral ventricular infestation ranges from 11% to 43% (Gupta et al., 2015; Teerasukjinda et al., 2016; Jensen and Post, 2016; Simão et al., 2018).
The aim of this study is to systematically analyze individual cases of lateral intraventricular neurocysticercosis (LVNCC) by examining patient demographics (age and sex), clinical presentation (duration of symptoms), parasitic evolution, precise localization of cysts within the ventricle, therapeutic interventions, and associated clinical outcomes
Methods
Search strategy and study selection
This systematic review follows the preferred reporting items for systematic reviews and meta-analysis guidelines. Using the keywords “intraventricular NCC,” “brain ventricle cyst,” “cysticercus cyst in brain ventricles,” “intraventricular cystic brain lesion,” “intraventricular cysticercosis,” “cysticercosis of the lateral cerebral ventricles,” and “neuroendoscopy,” we searched for the published cases and case series in the Medline database and Google Scholar, with no restrictions on publication dates. The review was restricted to articles published solely in English. The search process is detailed in Table 1 and Figure 1.

PRISMA 2009 flow diagram. PRISMA, preferred reporting items for systematic reviews and meta-analysis.
Medline Search String
The papers were screened and reviewed by two investigators (A.I. and Z.M.). In the first step, titles and abstracts were screened by one reviewer (A.I.), with the second reviewer (Z.M.) reassessing if there was uncertainty about the eligibility of the case/series. Next, the full-text articles were reviewed independently by A.I. and Z.M., with a third reviewer (S.O.) involved in resolving conflicts. We excluded cases with migrating cysts, multiple cystic lesions spanning two or more ventricles, and case series lacking individual case descriptions.
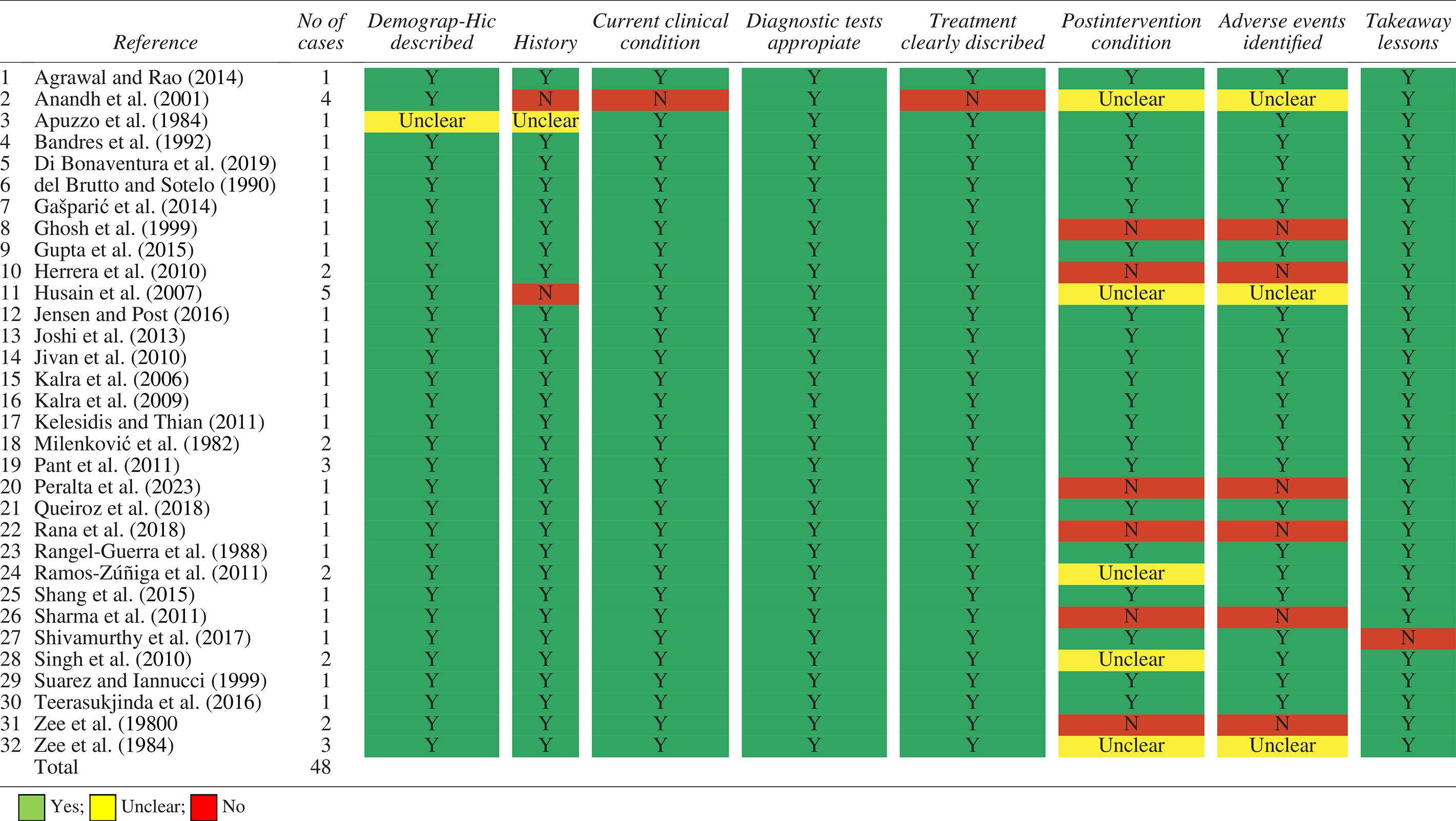
The Joanna Briggs Institute Critical Appraisal Tool: Checklist for Case Reports (Moola et al., 2020) was used to evaluate the methodological quality of case reports and case series (Table 2). The aim was to identify potential biases in the selected studies; however, articles with lower methodological quality were not excluded from the analysis. Most patients are presented in the form of case reports. The following data from eligible cases/series were extracted: age and sex, symptoms, clinical signs, diagnostic procedures, localization (region, ventricular site, parasite location within the ventricle), treatment, follow-up period, outcome, and year of publication. Patients were categorized into six age groups: under 16, 17–30, 31–40, 41–50, 51–60, and over 60. Data are presented as frequency and percentage. The same methodology was applied in individuals with a parasitic infestation of the TV and fourth ventricle (FV).
Quality Check Analysis—The Joanna Briggs Institute Critical Appraisal Checklist for Case Reports
NCC diagnosis was confirmed in all but two cases using a combination of computed tomography (CT), magnetic resonance imaging (MRI) with advanced techniques (constructive interference in steady state, fluid-attenuated inversion recovery, susceptibility-weighted angiography, fast imaging employing steady-state acquisition), serological tests, and most often with histological confirmation of cysticerci. The imaging findings of NCC cysts were defined according to the neuroimaging criteria (Carpio et al., 2016). We also adopted a set of revised diagnostic criteria and degrees of certainty to confirm the definite and probable diagnosis of IVNCC (Del Brutto et al., 2017).
Results
Literature search results
Through the literature search (search string presented in Table 1), we retrieved and subsequently screened 1225 articles. After applying our inclusion criteria, 1159 papers were excluded, while 66 remaining articles were assessed for eligibility (Fig. 1). Thirty-two articles were part of the final qualitative assessment, presented in Table 2. The included case reports/series were of high quality overall, followed by a comprehensive discussion of the clinical relevance of the reported patients.
Study characteristics
The selected 32 papers with 48 cases that met the inclusion criteria are presented in Table 3. The gender ratio was slightly balanced: 23 women and 25 men. The age ranged from 6 to 70 years (mean value 33.1 ± 14.1, median 33.5), with most patients being between 17 and 50 years old (79.2%). The highest frequency was observed in the age range of 33–49 years (33.3%) (Fig. 2). Patients with cysts in the TV and FV were younger (mean value 29.1, median 26.5, predominantly [47.7%] in the 17–30 age range) compared to those with LVNCC (p = 0.010058) (Fig. 2).
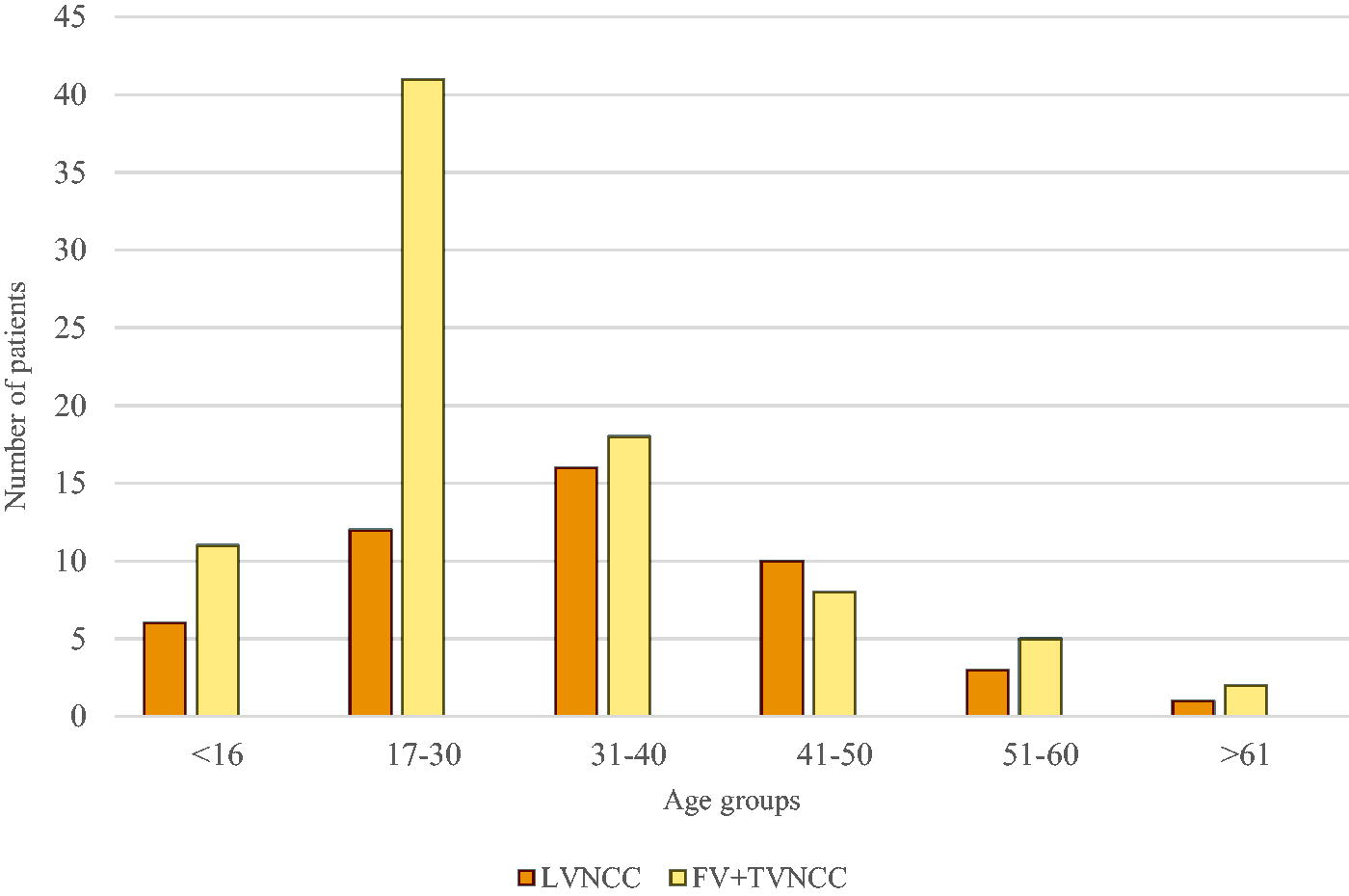
Comparative analysis of age between LVNCC and FV+TV NCC patients. FV, fourth ventricle; LVNCC, lateral intraventricular neurocysticercosis; NCC, neurocysticercosis; TV, third ventricle.
Tabular Presentation of the Lateral Intraventricular Neurocysticercosis
In a series of 21 cases with intraventricular neurocysticercosis six patients harboring the lateral ventricle cysts. Follow-up ranged from 3 months to 5 years (average 18 months).
Among the 11 countries in which lateral ventricular NCC was found, the highest number of cases was recorded in India (14 cases). In contrast, a significantly lower number of cases were noted in the USA (three cases), Mexico (three cases), Nepal (three cases), Serbia (two cases), Brazil, Indonesia, Guatemala, Hawai’i, EI Salvador, South Africa, Italy, the Dominican Republic, China, Croatia, and Canada (with one case each).
The predominant clinical manifestation was a headache (36/41 patients, 87.8%), followed by nausea and vomiting (22/41, 51.2%), altered sensorium (22/41, 51.2%), focal neurological deficit (12/41, 29.3%), and papilledema (11/41, 26.8%) (Fig. 3). In most patients, symptoms lasted from 10 d to 20 years (25 patients, 67.6%); a small percentage had an acute onset of the disease—within seven d (10 patients, 27%) (Table 3). The cysts were more commonly found in the left ventricle compared with the right ventricle (20 vs. 16), while three patients had cysts in both LVs. In nine patients (18.7%), the side of the ventricle was not specified. The frontal horn and the ventricular body were predominant locations for the parasite (16/23). Two individuals had entrapped (isolated) ventricles. Data were missing in 27 cases (Table 3). Regarding the histopathological/radiological stage of NCC, a higher percentage of vesicular cysts was observed (21 cases, 58.3%) compared with the degenerative stage (12 cases, 33.3%) and multiple confluent (racemose) cysts (2 cases, 5.5%). No relevant data could be obtained for 13 (27.1%) cases.

Frequency of symptoms in LVNCC according to cyst localization. LVNCC, lateral intraventricular neurocysticercosis; LVNM, lateral ventricle not mentioned.
The diagnosis was established using neuroimaging procedures (CT scan and MRI) with or without contrast in all of the cases except for two, combined with serological examinations (8/48 patients—16.6%) and in the majority of cases, histological confirmation of cysticerci in tissue samples (35/48 patients—72.9%). CSF was analyzed in 17 patients (35.4%), with 4 of these cases (8.3%) showing increased levels of both glucose and protein (Table 3).
Most patients underwent a surgical cyst extirpation (35/48 patients—72.9%). Six individuals (12.5%) were treated with open microsurgery (three of whom after 1990), while 29 patients (60.4%) underwent endoscopy, often combined with endoscopic third ventriculostomy (ETV) and occasionally with septostomy. Partial excision of the cyst was performed in one patient, while the rest underwent complete excision. The remaining patients were treated solely with VP shunt/ventriculostomy (five patients) or medical therapy (five patients). One patient was asymptomatic and did not receive treatment, while there was no information on the treatment type for two cases (Table 3).
Postoperatively, anthelmintics, as monotherapy or in combination with steroids and antiepileptic drugs, were used in 18 patients (37.5%). Thirty-three subjects (80.5%) experienced a favorable clinical outcome or improved clinical status. Six patients (12.5%) died: one due to the rupture of a large basilar aneurysm (accidental finding), while the others succumbed to severe ventriculitis or a sudden increase in intracranial pressure (ICP) caused by brain herniation. Follow-up periods ranged from 1 week to 16 years and were reported for 26 out of 41 patients (63.4%) (Table 3).
Discussion
The patients included in this study were predominantly from India, a territory where NCC is endemic (Flisser, 1994). There has been a notable reduction in the number of patients from other endemic areas, such as Mexico and Nepal, as well as from high-income countries, where LVNCC may be linked to international travel or migrations (Garcia, 2018).
The disease affects both sexes almost equally. Analysis of age data reveals that patients with lateral ventricular disease typically present at an older age compared to those with infections in the TV and FV. This delay in clinical presentation may be due to the larger space available in the LVs, allowing the parasite to grow for a longer time before affecting cerebral tissue.
Comparisons between patients with subarachnoid lesions and those with either ventricular or parenchymal NCC show that individuals with subarachnoid NCC are generally older in both scenarios (Marcin Sierra et al., 2017; Nateros et al., 2023). Contrary to some reports suggesting a preference for the occipital horn (Suri et al., 2008), our findings indicate that cysts most commonly localize in the anterior horn and body of the LVs.
Headache, nausea/vomiting, and altered sensorium were the most common clinical manifestations, generally indicative of increased ICP. Symptoms lasted from one week to several years, with a small percentage experiencing an acute onset. The duration of clinical manifestation before diagnosis varies significantly based on cyst location and its development. A growing cyst obstructing CSF flow manifests its symptomatology more rapidly, whereas inflammation, a slower developing process, may lead to signs and symptoms emerging several years after infection (Amelot and Faillot, 2014).
The presence of focal neurological deficits (hemiplegia, ataxia, vertical gaze paresis, vertigo, diplopia, gait ataxia, and upper gaze palsy) can be explained by the compression of local brain tissue by the parasite (e.g., corticospinal tract, visual pathways, periaqueductal gray matter, and floor of the FV) (Del Brutto et al., 2017).
Seizures are uncommon in the intraventricular form of the disease (Husain et al., 2007; Goel et al., 2008; Suri et al., 2008; Bustos et al., 2017). Visual disturbances, such as blurred vision, vision deterioration, loss of vision, and photophobia, were observed in 16–46.15% of cases (Citow et al., 2002).
Hydrocephalus (symmetrical or asymmetrical) was diagnosed in 81.3% of patients and has been noticed by many authors (Cuetter and Andrews, 2002; Husain et al., 2007; Goel et al., 2008; Bustos et al., 2017). Unilateral ventricle enlargement, the main characteristic of LVNCC, results from the unilateral obstruction of the foramen of Monro. Clinical manifestations typically progress gradually and are less severe compared with other hydrocephalus forms (Filho et al., 2011). The ensuing hydrocephalus can be incomplete or complete, acute or chronically progressive. The acute form may develop secondary to the obstruction of CSF flow, leading to increased ICP and potentially severe outcomes, including death within hours due to brain displacement, distortion, or herniation, as observed in three cases from this study (Zee et al., 1984). Occasionally, warning symptoms such as chronic headache, nausea, vomiting, and behavioral disorders may precede the acute event for months (Llompart Pou et al., 2005). An inflamed intraventricular cyst can mimic a tumor, potentially obstructing the foramina of Monro (Stern, 1981).
Ventricular inflammation, acute or chronic, is a significant condition that can be explained by an inflammatory reaction around a dead or dying cyst, and the formation of fibrous adhesions between the cyst capsule and the ventricular wall. Symptoms develop gradually as inflammation progresses. This can lead to scarring, partial or complete obstruction of CSF flow, hydrocephalus, and periventricular inflammation (Citow et al., 2002; Cuetter and Andrews, 2002; Araujo et al., 2008; Nash et al., 2018).
Treatment approaches vary, including both surgical and medical options. Endoscopy, often combined with ETV and occasionally with septostomy, was the primary treatment modality in the reviewed studies and is reported to be highly effective (Husain et al., 2007; Goel et al., 2008; Proaño et al., 2009; Singh et al., 2019). The main goal of this procedure is to manage obstructive hydrocephalus and to resect the cyst either partially or completely (Husain et al., 2007; Goel et al., 2008; Kumar et al., 2017). Complete resection can be challenging due to the risk of damaging surrounding structures. If the cyst is in the involutional or granular phase, antigenic materials released into the ventricles can cause local inflammation, leading to scarring and adherence of cysticerci to the ventricle wall or within the subarachnoid space. Partial resection with additional ETV is increasingly seen as a promising approach (Husain et al., 2007; Kaif et al., 2019). The Infectious Diseases Society of America and the American Society of Tropical Medicine and Hygiene recommend neuroendoscopy as the first option for treating LVNCC. If cyst excision poses significant surgical risks, treatment should focus solely on managing hydrocephalus (White et al., 2018).
Ventricular enlargement, a common clinical sign, was predominately treated by endoscopy, ETV, external ventricular drainage, and VP/VA shunts (Husain et al., 2007; Goel et al., 2008; Bustos et al., 2017).
All patients treated endoscopically showed favorable outcomes or improved clinical status. In most cases, the cyst was successfully removed (Husain et al., 2007; Goel et al., 2008; Kaif et al., 2019; Singh et al., 2019). Partial removal of the cyst does not lead to recurrence (Husain et al., 2007; Kaif et al., 2019), though some studies suggest that total resection may result in longer progression-free survival compared with partial resection (Zhenye et al., 2017). Cyst rupture during surgery is generally harmless and without complications (Husain et al., 2007). However, endoscopy carries risks, with some neurosurgeons reporting complications such as intraventricular hemorrhage, memory loss, hemiparesis, mutism, and aphasia (Proaño et al., 2009).
Six people (three of whom were treated after 1990, with the introduction of endoscopy) underwent open surgery and experienced a favorable outcome. Traditional microsurgical techniques have been used for years (Apuzzo et al., 1984; Ginier and Poirier, 1992; Kalra et al., 2006; Kotha, 2013). However, this approach has several drawbacks, including the need for craniotomy, potential blood loss, risk of delayed hydrocephalus, and the possibility of brain retraction, which can damage vital structures (Goel et al., 2008).
Five patients had VP shunt or ventriculostomy as the sole form of treatment and experienced fatal outcomes due to ventriculitis or brain herniation. VP shunt failure appears to be a common complication, associated with the risk of infection, drainage system occlusion, or cyst migration (Cuetter and Andrews, 2002; Anandh et al., 2001; Kelley et al., 2002). External drainage remains justified in patients with severe infection and ependymitis (Jensen and Post, 2016). Ventriculostomy, typically performed with ETV and sometimes combined with septostomy, is usually sufficient for managing obstructive hydrocephalus, and is commonly followed by removal or decompression of the cyst. ETV provides CSF diversion and avoids subsequent shunting. Successful outcomes of ETV range from 40% to 100% (Psarros and Coimbra, 2004; Suri et al., 2008; Proaño et al., 2009).
Eighteen patients (37.5%) received albendazole, either as monotherapy or in combination with steroids and antiepileptics, as part of postoperative treatment. Khade et al. (2013) found that patients who underwent resection of a single cyst with concomitant antiparasitic therapy had a lower rate of delayed hydrocephalus compared with those who did not receive such treatment. However, these findings were not confirmed by other studies (Nash et al., 2018; Milenković et al., 2023), possibly due to inadequate follow-up. Nevertheless, combining antiparasitic drugs with steroids is believed to reduce the rate of shunt failure rates in individuals requiring CSF shunting (White et al., 2018; Jensen and Post, 2016).
Nash et al. (2018) point out that long-term follow-ups are often neglected. In our study, we found documented follow-up data for 26 individuals (54.2%), all of whom exhibited favorable outcomes.
Limitations and Drawback of the Study
One limitation of this study is that it did not perform searches in more databases, which may have excluded some relevant case reports. Additionally, ambiguous cases might not be published due to the peer review process, and publication bias is a common issue in systematic reviews, particularly those involving case reports and series. Nevertheless, we believe that our search strategy remains thorough and inclusive, adequately covering the relevant literature necessary for this systematic review. When placed within the context of a rigorous systematic review, this data can offer useful clinical insights and support informed decision-making.
Conclusion
Lateral ventricular NCC is a serious condition characterized by rapid progression. Diagnosis relies on neuroimaging, serology, and histological confirmation of the parasite. Hydrocephalus is the dominant diagnostic sign, while headache, nausea, vomiting, and altered mental status are the most common manifestations of the infection. The duration of symptoms varies from one week to several years, with some cases presenting acutely. Invasion of the ventricle by cysticerci occurs mainly in middle-aged individuals. Endoscopy is the preferred treatment option, though prognosis depends on various factors. Untreated patients face high mortality rates. Continued research and long-term follow-up studies are needed to better understand disease progression, aid timely diagnosis, refine treatment protocols, and improve patient outcomes.
Footnotes
Authors’ Contributions
Z.M.: Conceptualization (equal), data curation (lead), writing—original draft (lead), writing—review and editing (supporting); A.I.: Formal analysis (lead), data curation (supporting); visualization (equal); M.S.: Visualization (equal), writing—original draft (supporting); M.R.: Visualization (equal), writing—original draft (supporting); G.K.: Validation (equal); S.M.: Validation (equal); S.O.: Conceptualization (equal), supervision (lead), writing—review and editing (lead). All authors agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosure Statement
The authors have declared that no competing interests exist.
Funding Information
This work was supported by the Ministry of Science, Technological Development and Innovation of the Republic of Serbia; Grant No.