
Abstract
We investigated bacterial pathogens on restaurant cutting boards using phenotypic and molecular methods, and determined their antibiotic susceptibility. A total of 32 samples were collected from polyethylene cutting boards in the kitchens of 16 restaurants in Rio de Janeiro, Brazil. A total of 29 bacterial strains were isolated and identified, including Salmonella spp. (n = 11), Escherichia coli (n = 10), Staphylococcus aureus (n = 6), and Listeria spp. (n = 2). Of the 32 cutting boards, 9 (28.1%) harbored at least one bacterial species, 7 (21.9%) had two species, and 2 (6.2%) carried three species. Notably, the detection of two pathogens directly from raw samples using quantitative polymerase chain reaction with high-resolution melting (qPCR-HRM) was significant: Listeria monocytogenes was identified in two samples by phenotypic methods but in 18 samples by qPCR-HRM, while E. coli was found in 10 samples by phenotypic methods and in 29 samples by qPCR-HRM. Antibiotic resistance was another concern, especially for L. monocytogenes strains, which exhibited high resistance to all tested antibiotics. Additionally, multidrug-resistant strains were identified, including a S. aureus strain with strong potential to be methicillin-resistant. Our findings underscore the importance of molecular methods for detecting specific pathogens on food-processing surfaces, highlighting the need for improved monitoring and control measures in restaurant kitchens.
Introduction
Foodborne and waterborne diseases (FWD) are a major global concern, with poor hygiene in food handling contributing to pathogen spread. Eating out is routine for millions, yet foodborne diseases remain a leading cause of morbidity and mortality. The WHO estimates 600 million annual cases and 420,000 deaths due to foodborne outbreaks, with economic losses of $7.4 million annually (PAHO (Pan-American Health Organization), 2022).
In Brazil, the 2017–2018 Household Budget Survey (IBGE (Instituto Brasileiro de Geografia e Estatística), 2019) reported that 32.8% of food expenses went to eating out. Between 2012 and 2021, Brazil recorded 6347 foodborne outbreaks, affecting 821,316 people, with 13,446 hospitalizations and 86 deaths (BRASIL). The leading outbreak sources were households (35.1%), restaurants/bakeries (15%), and daycares/schools (11.7%). The most identified pathogens were Escherichia coli (29.6%), Staphylococcus aureus (12.9%), Salmonella spp. (11.2%), and Bacillus cereus (7.2%).
FWD often result from improper storage, poor food handling, and cross-contamination. Contamination in restaurants can occur at any stage—storage, preparation, or serving—originating from raw food, air, water, or human/animal waste (Bukhari et al., 2021). While health surveillance has reduced FWD incidence, antimicrobial resistance in pathogens such as Cronobacter sakazakii, Listeria monocytogenes, Salmonella Typhimurium, and Campylobacter jejuni poses a growing threat (Odeyemi and Sani, 2016).
Traditional microbiological methods are time-consuming and labor-intensive (Law et al., 2014). In contrast, molecular techniques such as quantitative polymerase chain reaction (qPCR) offer greater sensitivity, specificity, and speed (Foddai et al., 2020). An advanced approach, qPCR with high resolution melting (qPCR-HRM), enables rapid pathogen differentiation by analyzing DNA melting profiles, successfully detecting E. coli, Salmonella spp., L. monocytogenes, and S. aureus (Liew et al., 2004; Singh and Velez, 2023).
qPCR-HRM provides higher sensitivity for low bacterial loads, pathogen differentiation, and high-throughput screening. It can also target virulence and antimicrobial resistance genes, offering deeper insights into bacterial pathogenicity (Singh and Velez, 2023). Integrating qPCR-HRM into routine food safety monitoring could enhance surveillance, reduce contamination risks, and improve public health.
This study investigates the presence of Salmonella spp., enterotoxigenic E. coli, S. aureus, and L. monocytogenes on restaurant cutting boards, along with their antibiotic resistance profiles. Our findings contribute to health surveillance efforts and provide valuable data for future research.
Materials and Methods
Sample collection
A total of 32 samples were randomly collected from polyethylene cutting boards in 16 restaurant kitchens across Rio de Janeiro, representing varying capacities: small (up to 50 seats), medium (up to 100 seats), and large (over 100 seats). Sampling took place between June 14 and September 17, 2021, as previously described (Mendes et al., 2011), with two cutting boards randomly selected from each restaurant.
Briefly, for each board, a sterile sponge was introduced in a sterile Whirl-Pak plastic bag (Nasco, USA) containing 100 mL of 1% Buffered Peptone Water. With a procedure glove, the sponge was squeezed to remove excess liquid and rubbed against the cutting board, in a delimited area of 25 cm2, for each sample. After collection, the sponge was placed back inside the plastic bag, closed, and identified. The samples were transported in an isothermal box with recyclable ice at +4°C to +8°C and stored under refrigeration for further analysis within 24 h from the collection.
Microbiological analysis
Plastic bags containing the sponge with diluent were homogenized in a Stomacher Enrichment Sample Homogenizer (Merck-Germany) at speed 2, for 60 s. After this step, the samples were processed aiming the isolation of the microorganisms of interest. For counting and identification of E. coli, a Petrifilm™ EC plate (3M, USA) was used according to the manufacturer’s recommendations. For the identification of Salmonella spp. strains, we used the methodology previously described in the Bacteriological Analytical Manual—Food and Drug Administration (BAM/FDA, 2024). The presence of S. aureus in the samples was assessed according to the recommendations of the ISO 6888-1 (ISO 6888-1, 1999), using Baird Parker agar. L. monocytogenes research was carried out according to the methodology previously described (Hitchins et al., 2022), in the BAM/FDA. The reference strains used as standards to test the selection media according to BAM/FDA, are described below.
Molecular analysis
All isolated strains identified by a specific microbiological method previously described were submitted to molecular identification and species confirmation.
Genomic DNA extraction and purification
Genomic DNA was extracted and purified using the Gram-positive and Gram-negative protocols of the PureLink™ Genomic DNA Mini Kit (Invitrogen), according to the manufacturer’s instructions. Purified genomic DNA were stored at −20°C for further analysis.
Bacteria detection by qPCR-HRM
qPCR-HRM was used to confirm the presence of pathogens in the samples collected in the restaurants, detected by the conventional phenotypic methods previously described. To determine specific reference melting temperatures (Tm) for each species, the following reference strains were used with the specific Tm indicated and were supplied by the Collection of Pathogenic Bacteria at INCQS/FIOCRUZ:
E. coli (Ts) INCQS 00310 (ATCC 11775) → 78.8°C (±0.5°C)
E. coli (EHEC) INCQS 00171 (CDC EDL-933) → 75.8°C (±0.5°C)
L. monocytogenes INCQS 00673 (ATCC ATCC BAA-751) → 74.5°C (±0.5°C)
L. monocytogenes (Ts) INCQS 00353 (ATCC 15313) → 74.5°C (±0.5°C)
S. aureus (Ts) INCQS 00358 (ATCC 12600) → 79.8°C (±0.5°C)
S. aureus INCQS 00306 (ATCC 33591) → 79.8°C (±0.5°C)
Salmonella enterica subsp. enterica serovar Choleraesuis INCQS 00028 (ATCC 10708) → 80.6°C (±0.5°C)
Strains indicated as Ts are Type strains, EHEC is enterohemorrhagic E. coli.
qPCR-HRM experiments were carried out using the MeltDoctor-HRM Master Mix reagent (ThermoFisher), which contains a fluorescent DNA intercalating agent (Syto-9) that emits fluorescence when bound to double-stranded DNA and is the MasterMix indicated by the equipment manufacturer for qPCR-HRM reactions. The primers used are described in Table 1, and the reaction parameters used are listed in Table 2. The reactions were analyzed with the QuantStudio™ Flex Real-Time PCR Systems (QS7) thermocycler (Applied Biosystems). Additionally, raw cutting board samples were also submitted to pathogens detection by direct analysis through qPCR-HRM.
List of Primers Used for Pathogens Identification by qPCR-HRM
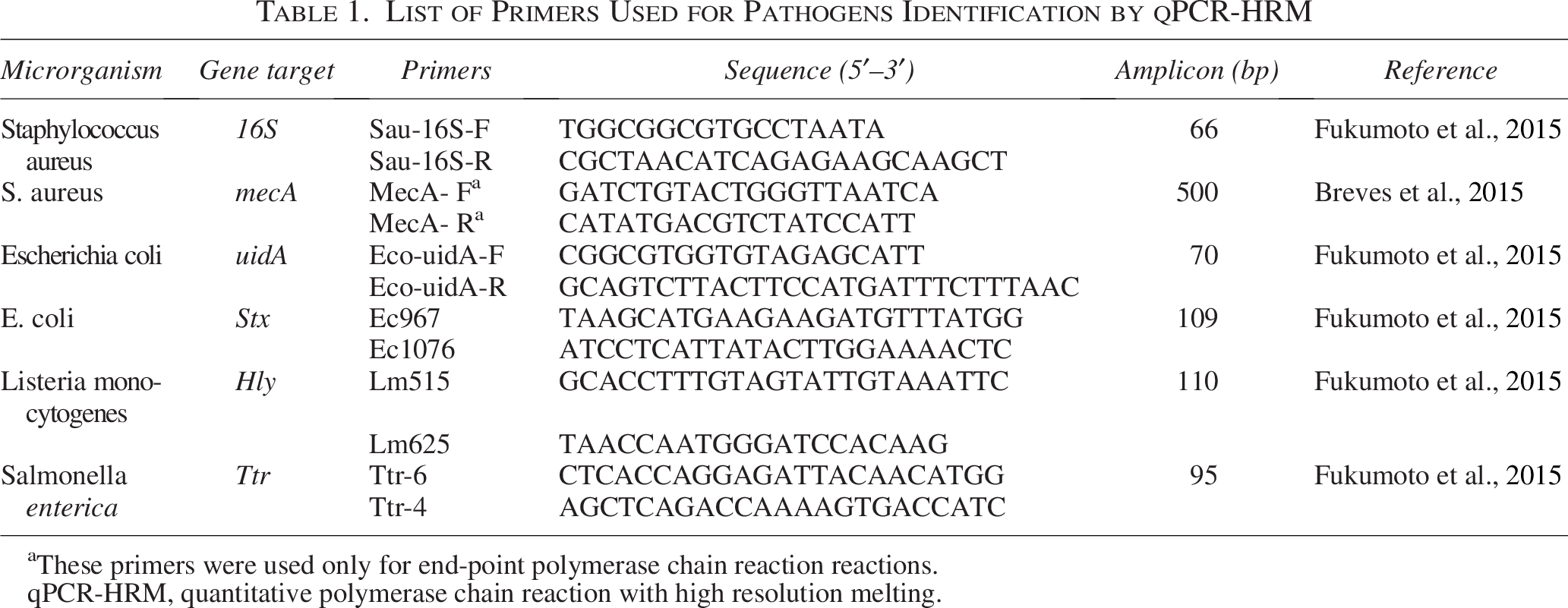
These primers were used only for end-point polymerase chain reaction reactions.
qPCR-HRM, quantitative polymerase chain reaction with high resolution melting.
Reaction Parameters of qPCR-HRM in QS7
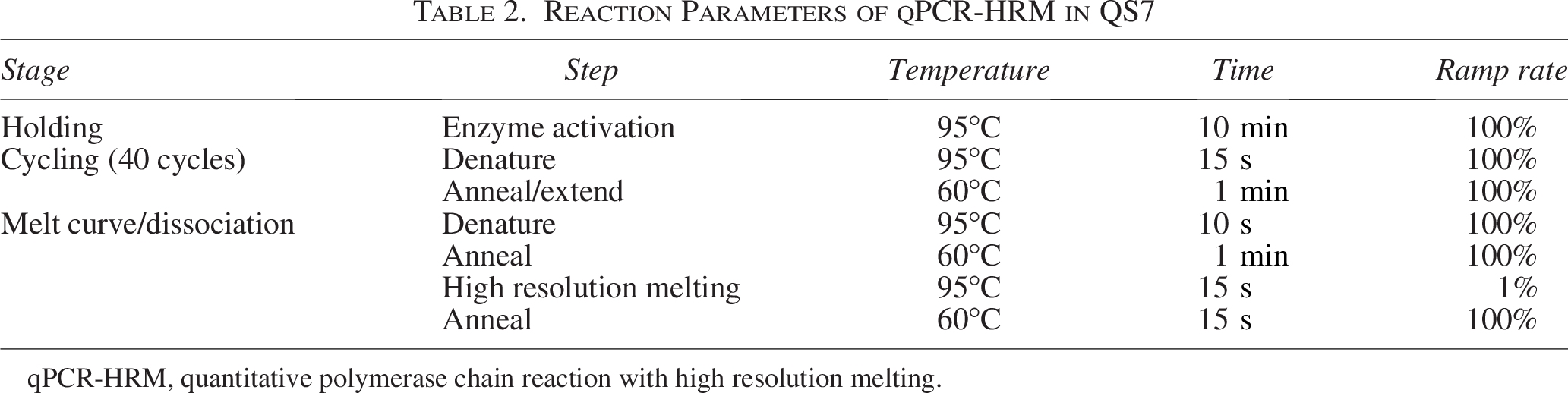
qPCR-HRM, quantitative polymerase chain reaction with high resolution melting.
Antimicrobial susceptibility tests
Disk-diffusion test
The determination of susceptibility to antibiotics was performed using the disk-diffusion test (Bauer et al., 1966), providing qualitative results, following the EuCAST criteria. In the disk-diffusion test, filter paper discs containing antibiotics at fixed concentrations were used. Table 3 shows the antimicrobials used in the antimicrobial susceptibility test (AST).
Antibiotics Used for the AST
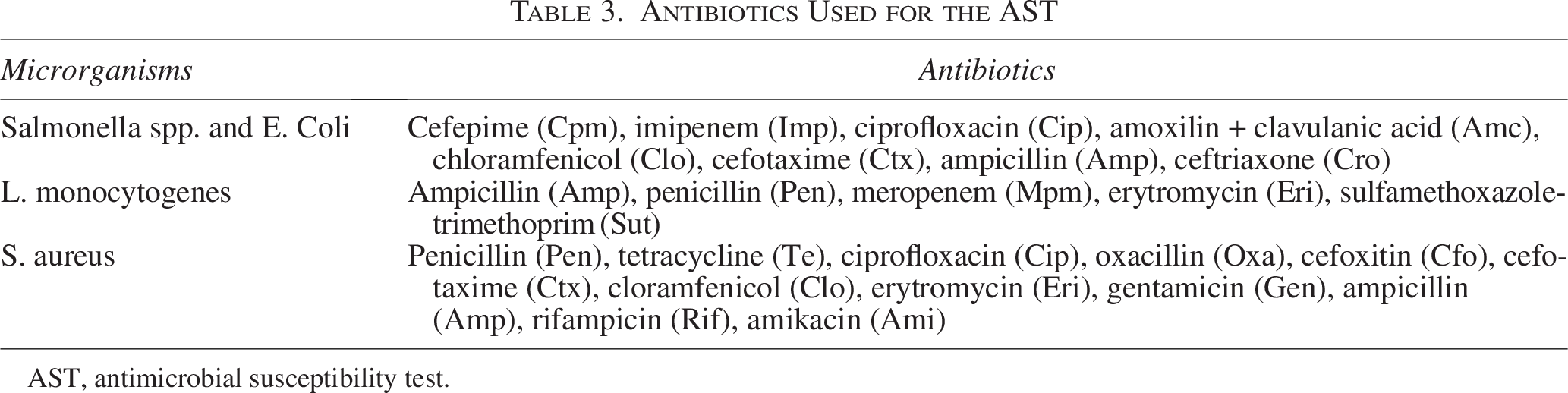
AST, antimicrobial susceptibility test.
Minimum inhibitory concentration test
Strains with resistant or intermediary profiles after disk-diffusion tests, were submitted to MIC for the quantitative AST.
To determine the minimum inhibitory concentration (MIC), a strip (M.I.C. Evaluator™ strips—OXOID) with a gradient of antibiotic concentration was used, indicating the minimum concentration necessary to inhibit the growth of the microorganism. The MIC test was performed according to the EuCast manual (EUCAST, 2023).
Control strains
Control strains used for AST were as follows: E. coli ATCC 25922 E. coli and Salmonella spp.), S. aureus ATCC 29213 (S. aureus) and Streptococcus pneumoniae ATCC 49619 (L. monocytogenes).
Results
Pathogen detection on restaurant cutting boards
From 32 raw samples collected from cutting boards, phenotypic analysis identified Salmonella spp. (11 strains, 34.3%), E. coli (10 strains, 31.2%), S. aureus (6 strains, 18.7%), and L. monocytogenes (2 strains, 6.2%). Fourteen samples (43.7%) showed no growth of these pathogens. At least one species was recovered from nine samples (28.1%), two species from seven samples (21.9%), and three species from two samples (6.2%).
Pathogen detection by qPCR-HRM
qPCR-HRM confirmed 10 of the 11 Salmonella spp. strains (90.9%) identified by phenotypic methods from eight cutting board samples. Serological analysis identified serovars Infantis (n = 3), Corvallis (n = 1), and Muenchen (n = 1), all belonging to S. enterica subsp. enterica. Six strains could not be serotyped and were classified as “others.”
All 10 E. coli strains (100%) identified phenotypically were confirmed by qPCR-HRM, and 29 strains were detected in raw samples using the molecular method. qPCR-HRM screening for the stx gene, which encodes Shiga toxin (EHEC), found the gene in only 2 of the 10 isolated strains (20%), but in 13 of the 29 total E. coli detected in raw samples (44.8%).
For S. aureus, qPCR-HRM confirmed four of the six strains identified phenotypically (66.6%). However, no S. aureus strains were detected directly from raw samples using qPCR-HRM. This discrepancy warrants further investigation to understand the potential detection limitations of molecular methods for S. aureus in this context.
Both L. monocytogenes strains isolated phenotypically were confirmed by qPCR-HRM (100%), while 20 L. monocytogenes strains were detected directly from raw samples using qPCR-HRM (Fig. 1).
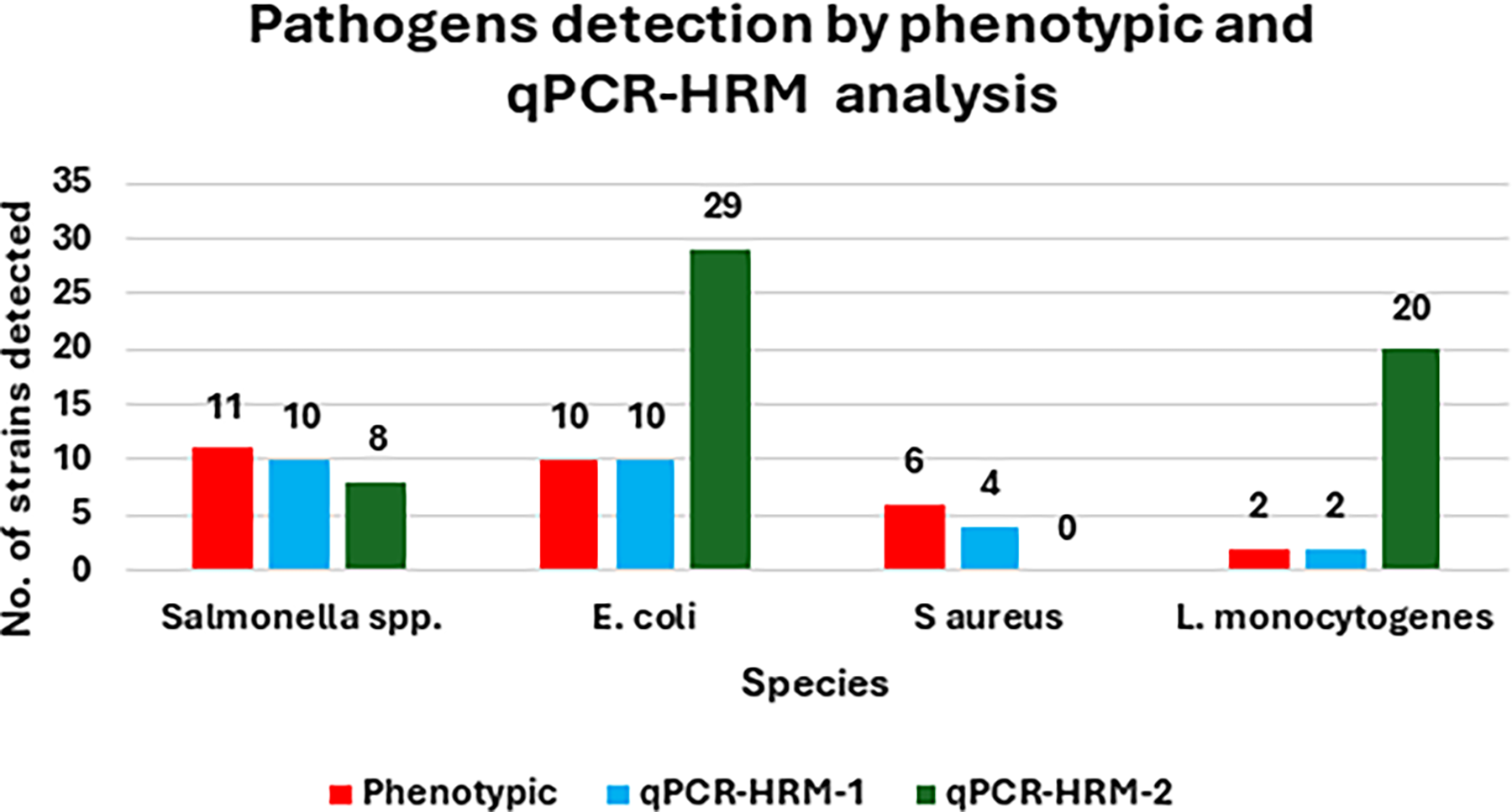
Comparison of the phenotypic and molecular (qPCR-HRM) analysis for pathogens detection. qPCR-HRM-1, from isolated strains; qPCR-HRM-2, from cutting board raw samples. qPCR-HRM, quantitative polymerase chain reaction with high resolution melting.
Antimicrobial susceptibility testing
All isolated pathogen strains underwent AST using the disk-diffusion method, with resistant (R) and intermediate (I) strains further analyzed using MIC testing.
L. monocytogenes (two strains): exhibited the highest resistance profile, with both strains resistant to penicillin, meropenem, erythromycin, and sulfamethoxazole-trimethoprim. One strain was also resistant to ampicillin. Both were classified as multidrug-resistant (MDR), as defined by Magiorakos et al. (2012).
S. aureus (five strains): two strains were resistant to penicillin (MIC 50 µg/mL), and one showed resistance to tetracycline, oxacillin, cefoxitin, cefotaxime, and ampicillin. All five strains were resistant to ciprofloxacin and erythromycin, with two exhibiting MIC values >256 µg/mL for erythromycin and one at 75 µg/mL. All were susceptible to chloramphenicol, gentamicin, rifampicin, and amikacin. One MDR strain, resistant to oxacillin, penicillin, tetracycline, ciprofloxacin, and erythromycin, had a high probability of being methicillin-resistant (MRSA). However, the mecA gene could not be conclusively detected.
Salmonella spp. (11 strains): 5 strains were resistant to amoxicillin/clavulanic acid and amikacin; 3 to ciprofloxacin and ceftriaxone; 2 to imipenem; 1 to cefotaxime and cefepime. All were susceptible to chloramphenicol.
E. coli (10 strains): resistance was observed for cefepime (6 strains), imipenem (4), ciprofloxacin (5), amoxicillin/clavulanic acid (6), chloramphenicol (2), cefotaxime (4), ampicillin (5), and ceftriaxone (7). Two strains were MDR, resistant to three antibiotic classes. Figure 2 presents susceptibility profiles for each pathogen based on disk-diffusion and MIC testing.
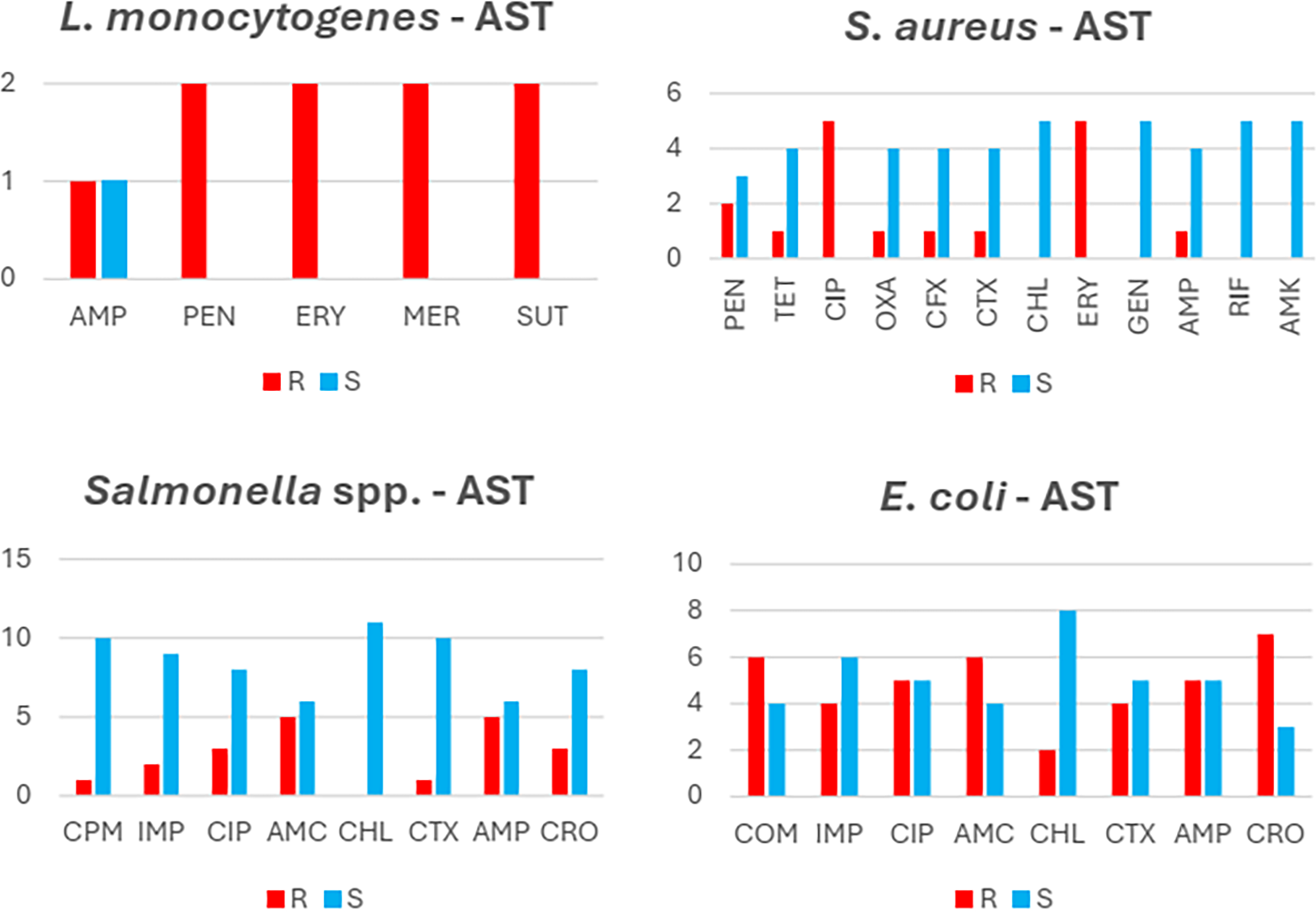
Susceptibilty profiles of the four pathogens isolated in the study. AMC, amoxicillin + clavulanic acid; AMK, amikacin; AMP, ampicillin; CFX, cefoxitin; CHL, chloramphenicol; CIP, ciprofloxin; CPM, cefepime; CRO, ceftriaxone; CTX, cefotaxime; ERY, erythromycin; GEN, gentamicina; IMP, imipenem; MER, meropenem; OXA, oxacillin; PEN, penicillin; RIF, rifampicin; SUT, trimethoprim/sulfamethoxazole; TET, tetracycline.
Discussion
This study introduces a molecular detection method based on real-time PCR (qPCR) with HRM, referred to as qPCR-HRM, for identifying foodborne pathogens and characterizing E. coli pathotypes. Compared with conventional phenotypic methods, qPCR-HRM demonstrated superior sensitivity, confirming 69% of the strains identified phenotypically. This highlights the necessity of molecular verification to ensure accurate species identification.
From 32 cutting board samples, phenotypic methods isolated 29 strains, while qPCR-HRM detected 57, a 196% increase. Notably, L. monocytogenes was found in 62.5% of raw samples by qPCR-HRM but only 6.25% by phenotypic methods, highlighting a 10-fold sensitivity increase. These results emphasize the limitations of traditional methods and the need for molecular approaches in food safety monitoring. The study also identified oxacillin-resistant S. aureus and enterohemorrhagic E. coli (EHEC) strains. One S. aureus strain showed resistance to penicillin, oxacillin, tetracycline, and ciprofloxacin.
The detection of Salmonella spp., E. coli, and S. aureus, common in foodborne outbreaks, suggests inadequate hygiene in restaurants (Dos Santos). Contamination may stem from poor cleaning, damaged cutting boards, or cross-contamination. Notably, only serology could classify Salmonella strains into serovars, while phenotypic methods and qPCR-HRM confirmed only genus-level presence.
qPCR-HRM analysis of raw cutting board samples did not detect S. aureus, despite 66.6% of phenotypically identified strains being confirmed by qPCR-HRM. This discrepancy warrants further investigation. A possible explanation is DNA degradation due to prolonged food storage, nucleases, or environmental conditions. Notably, three S. aureus isolates exhibited MDR, with one resistant to four antibiotic classes. Although this strain showed phenotypic resistance to oxacillin and beta-lactams, it lacked the mecA gene.
Our study also detected E. coli strains harboring the stx gene, characteristic of EHEC. Among 29 E. coli strains identified by qPCR-HRM, 13 carried the stx gene, including 2 isolated phenotypically. While five E. coli strains exhibited MDR profiles, resistance was not associated with the presence of stx, indicating that virulence and antibiotic resistance traits occur independently. Regardless, both MDR and EHEC strains present serious health risks, capable of causing severe conditions such as septicemia and meningitis (Froder et al., 2021).
Our study detected E. coli strains with the stx gene, characteristic of EHEC. Among 29 E. coli strains identified by qPCR-HRM, 13 carried stx, including 2 confirmed phenotypically. Five strains showed MDR profiles, but resistance was unrelated to stx, indicating independent virulence and resistance traits. Both MDR and EHEC strains pose serious health risks, potentially leading to septicemia and meningitis (Froder et al., 2021).
The detection of L. monocytogenes on restaurant cutting boards is concerning due to its link to listeriosis, a severe risk for immunocompromised individuals, pregnant women, and newborns (Goulet et al., 2013). Its persistence on food-contact surfaces highlights the need for strict hygiene. Despite Brazilian regulations requiring smooth, washable, and waterproof cutting boards, contamination occurred. Though few L. monocytogenes strains were phenotypically isolated, all showed high antibiotic resistance with MDR profiles, emphasizing the threat of resistant pathogens in food-handling environments.
Salmonella spp. isolates were classified into the serovars Infantis, Corvallis, and Muenchen, all of which are known to cause gastroenteritis and septicemia in immunocompromised individuals (Bertani, 2020). Salmonella contamination of cutting boards presents a significant risk for cross-contamination, particularly from poultry and pork products, emphasizing the need for rigorous cleaning protocols (Medeiros et al., 2011; CDC (Centers for Disease Control and Prevention), 2022). Among the Salmonella isolates, only one strain was MDR, while two were fully susceptible to all tested antibiotics. No resistance was observed for chloramphenicol or cefepime. Despite this relatively low resistance, the detection of pathogenic Salmonella serovars in food establishments warrants heightened surveillance and stricter hygiene enforcement.
We could not determine whether cutting board contamination resulted from improper cleaning, cross-contamination, or handling practices.
While phenotypic methods remain widely used due to cost-effectiveness, discrepancies with molecular detection for L. monocytogenes and E. coli may stem from bacterial expression variations, viable but nonculturable cells, or limitations of culture-based techniques. These discrepancies highlight the complementary nature of both methods: molecular techniques detect genetic material from live and dead cells, while phenotypic methods assess microbial viability. Integrating both enhances contamination risk assessment.
Despite this limitation, our study underscores the advantages of molecular methods like qPCR-HRM, which confirmed all phenotypically identified species and significantly improved detection, 3-fold for E. coli and 10-fold for L. monocytogenes. These findings support adopting molecular techniques in food safety monitoring. To our knowledge, this is the first study to detect foodborne pathogens using qPCR-HRM.
While cutting boards are key contamination vectors, other surfaces like knives, countertops, sinks, and food handlers’ hands also contribute to pathogen transmission. Our study focused on cutting boards due to their direct food contact, but future research should assess multiple kitchen surfaces and equipment for a broader contamination analysis. Sampling food handlers and raw ingredients could further clarify bacterial spread. Despite this limitation, our findings highlight the need for strict hygiene and sanitation in commercial kitchens.
Regular inspections and health certifications ensure restaurant compliance with hygiene protocols, maintaining public trust (Soragni et al., 2019). Strengthened surveillance and monitoring are vital for preventing foodborne illnesses and protecting public health.
While we acknowledge that the sample size is limited, our study provides valuable insights into the presence of foodborne pathogens on cutting boards used in restaurant kitchens. The selected restaurants varied in capacity (small, medium, and large), allowing us to capture data from different operational scales. Additionally, our primary objective was to assess the effectiveness of qPCR-HRM for pathogen detection rather than conduct an epidemiological survey. Future studies should expand sampling across multiple regions and a larger number of establishments to further validate our findings and improve the generalizability of the results.
We acknowledge that our study was qualitative rather than quantitative, focusing on the presence of foodborne pathogens rather than determining their infectious doses. While detection confirms contamination, pathogen load is a key factor in assessing public health risks, as infectious doses vary depending on the microorganism and host susceptibility. For instance, L. monocytogenes poses a high risk even at low doses (∼100 CFU/g), particularly for immunocompromised individuals, pregnant women, and newborns. EHEC (E. coli O157:H7) has an infectious dose as low as 10–100 CFU, while Salmonella spp. typically requires a higher dose (∼104–106 CFU) to cause illness. However, even low levels can be problematic due to cross-contamination and improper food handling. Future studies should incorporate quantitative methods (e.g., qPCR with standard curves or culture-based enumeration) to determine microbial loads and better assess potential health risks. Despite this limitation, our study underscores the widespread presence of foodborne pathogens in restaurant kitchens, reinforcing the need for strict hygiene practices to mitigate contamination risks.
Conclusions
Our findings reveal widespread foodborne pathogens on restaurant cutting boards, highlighting consumer health risks and the advantages of qPCR-HRM for detection. The presence of MDR strains, including a potential MRSA, underscores the need for stricter food safety practices and antimicrobial resistance surveillance. Enforcing hygiene measures, regular disinfection, and proper food handling is crucial to ensuring food safety and protecting public health.
Authors’ Contributions
B.d.S.C.: Conceptualization, data curation, formal analysis, investigation, methodology, validation, visualization, and writing—original draft. K.C.S.: Data curation, formal analysis, and methodology. C.T.M.P.R.: Data curation, formal analysis, and methodology. A.C.C.D.O.: Data curation, formal analysis, and methodology. S.M.d.R.L.: Conceptualization, data curation, project administration, resources, supervision, visualization, and writing—review and editing. I.d.F.: Conceptualization, data curation, funding acquisition, project administration, resources, supervision, visualization, and writing—review and editing.
Footnotes
Acknowledgments
The authors are grateful to the Graduate Program in Health Surveillance—PPGVS (INCQS/FIOCRUZ), Sequencing core Plataforma Genomica de Sequenciamento de DNA/PDTIS-FIOCRUZ, Laboratorio de Enterobacterias—IOC/FIOCRUZ, Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES)—Finance Code 001 and to the restaurants that contributed to the study, providing access to their cutting boards.
Funding Information
No funding was received for this article.
Ethical Approval
No human ethical approval was required as no human samples were analyzed in this study. Since the bacterial isolates were obtained from food samples, the study was registered with the Genetic Heritage Council under registration number A894817.
Data Availability Statement
All data are incorporated into the article. There are no additional data to be shared.
Disclosure Statement
The authors have no financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the article.