
Abstract
Abstract
Objective:
This study compared older adults' gains in cognitive and everyday functioning after a 60-session home-based videogame intervention with gains seen under formal cognitive training and usual care/no intervention.
Materials and Methods:
Participants were randomized to one of three groups: one group played an off-the-shelf videogame (i.e., Crazy Taxi), the second group engaged in a computerized training program focused on visual attention and processing speed (i.e., PositScience InSight), and the third group received no training. Training in the two intervention conditions consisted of 60 training sessions of 1 hour each, which were completed in 3 months (5 hours a week). Participants received a broad battery of cognitive and everyday functioning assessments immediately before (pretest), after (post-test), and 3 months after (follow-up) training.
Results:
Both training conditions improved on direct assessments of trained outcomes. In the InSight-trained group, we found transfer to untrained measures of visual attention and processing speed that were similar to the trained tasks, and these gains endured for up to 3 months. Participants in the videogame condition showed small additional benefits, not emerging until 3 months after intervention completion, on a measure of both attention and mood. No trained groups showed gain on visuospatial skills or memory.
Conclusion:
Training effects were highly specific to the target of training. Training effects to visual attention and processing speed were, as expected, larger for InSight-trained participants but were also seen for videogame participants. Given that past research has shown that videogame training leads to greater engagement than cognitive training, videogame interventions may represent a choice for more modest gains in a more engaging context.
Introduction
There is an ongoing quest to identify cognitive enhancement approaches that maintain and improve age-sensitive aspects of cognition in later life, and ideally contribute to the maintenance of independent function. There are various methods of intervention that have some empirical support, including physical exercise, 1 ability-specific cognitive training, 2 and generalized engagement in complex activity. 3
With regard to cognitive training, the general finding has been that adults, even into advanced old age, and those at risk of cognitive impairment 4 can continue to profit from cognitive interventions. 5 Indeed, the Advanced Cognitive Training in Independent and Vital Elderly (ACTIVE) 6 study suggested that as few as 10 sessions of training can have discernible residual performance benefits relative to untrained controls, and training gains lasted up to 5–10 years.2,5 Improvements due to training in one cognitive domain, however, generally did not result in improvements in an untrained cognitive domain. 2
One well-researched type of cognitive training to improve speeded visual processing in older adults is the computer-administered Useful Field of View (UFOV) training. Across multiple investigations, studies have shown large improvements in speed, as well as divided and selective attention.7–10 In addition, research has shown some generalization of training effects to non-UFOV tasks.11–14
In the largest study of UFOV training, ACTIVE, training transfer effects were ability specific, but compared with untrained controls, UFOV-trained participants reported less depression, better self-reported health, better quality of life (5 years after training),15–17 and fewer limitations in instrumental activities of daily living (IADLs). 5 The InSight program from Posit Science was adapted from the traditional UFOV training.
Videogame interventions share some features with computer-based cognitive training (e.g., attention and speed demand, require the coordination of multiple abilities, 18 and provide instant performance feedback). 19 In addition, videogames are cognitively and perceptually demanding, and often also similar to computerized cognitive training; videogames might allow for large, ongoing dosages, situated in the home environment; many videogames also allow adaptive and incremental difficulty. 20
At the same time, videogames differ from cognitive training, in that they are less focused on specific cognitive skills, often have higher “stakes” (i.e., there is a mission or objective to complete),18,21 extend the body into new pseudonaturalistic environments, 22 and exist primarily for engagement and leisure.23,24 These differences suggest that videogames may also activate a second route to cognitive improvement, which is “engagement” or stimulation. 25 Engagement interventions differ from traditional cognitive training, in that there is not a specific cognitive domain that is trained, but rather the person participates in one or more activities that may involve learning new skills that require a wide range of cognitive demands (e.g., learning photography, etc).26–28 These types of engagement programs have demonstrated improvement in several cognitive domains.24–30
There is evidence from across the adult life span that videogames can improve attentional measures such as UFOV performance, 31 multiple object tracking, 32 and attentional blink. 33 Cognitive benefits of videogames have also been reported for older adults.34–39 For instance, our previous work reported that two videogames, Medal of Honor and Tetris, improved selective visual attention/UFOV at a magnitude that approached the gains seen in formal UFOV training. 40 In a follow-up study, we showed that one advantage of a videogame intervention over cognitive training was that games increased perceived flow/engagement over time, while engagement declined for those receiving computerized UFOV training. 41 It is important to note that this was a monochromatic MS-DOS-based version of UFOV training. When graphic and game-like aspects of UFOV training were enhanced in InSight, engagement no longer declined in UFOV-trained participants, but it again improved only in videogame-trained participants. 42
The present Research to Examine Videogame Intervention for Visual Attention (REVIVA) study compared traditional cognitive training (UFOV training via PositScience InSight) with videogame training (using the off-the-shelf driving game, Crazy Taxi [CT]), and also with a no-treatment control group. Contributions of this study included (a) focus on older adults, (b) entirely home-based interventions, (c) extended dosages (60 hours), (d) alternative treatment design (comparison of cognitive training and videogame interventions with each other and with controls); and (e) assessment of intervention effects through an extensive theoretically guided hierarchy of primary, near-transfer, and far-transfer outcomes.
This study was designed to address some of the major critiques of prior videogame training and cognitive intervention research offered by Simons, Boot et al.43,44 For example, because training/control group comparisons may contrast groups that are unmatched in experimental attention and expectations, this study compared two active interventions (videogames vs. cognitive training) with one another. Importantly, these two interventions were presented as active to the participants. At the same time, we retained a traditional testing-only control group to be able to compare training gains against those that could be achieved by retest alone. It is acknowledged that the no-contact control group only controls for some aspects of study participation (practice effects, volunteerism, and study engagement), but the alternative treatment groups then should help us to further control for expectation, placebo effects, motivation, etc., which might also influence performance. Finally, we transparently reported not only all outcomes measured but also those with intervention effects.
Materials and Methods
Ethics statement
All research was approved by the Institutional review board of the University of Florida. Informed consent was obtained for all participants, and the investigation was conducted according to the principles expressed in the Declaration of Helsinki.
Participants
Fifty-four community-dwelling older adults completed the study (CT, n = 17; InSight, n = 19; and Control, n = 18). Participants were community dwelling, aged 65–86 years (mean age = 73.2, SD = 5.5), highly educated (46% had a master's or doctorate degree and 18.5% had a bachelor's degree), 90% white, and 63% female.
Attrition
One hundred forty-nine participants were screened for the study (Fig. 1). A total of 71 (48%) participants were eligible. Seventeen participants (24%) (eight CT, one InSight, and seven controls) withdrew from the study. Withdrawal was not related to randomized group, χ 2 (2) = 5.793, P = 0.055, or to age, education, or gender (P > 0.05).
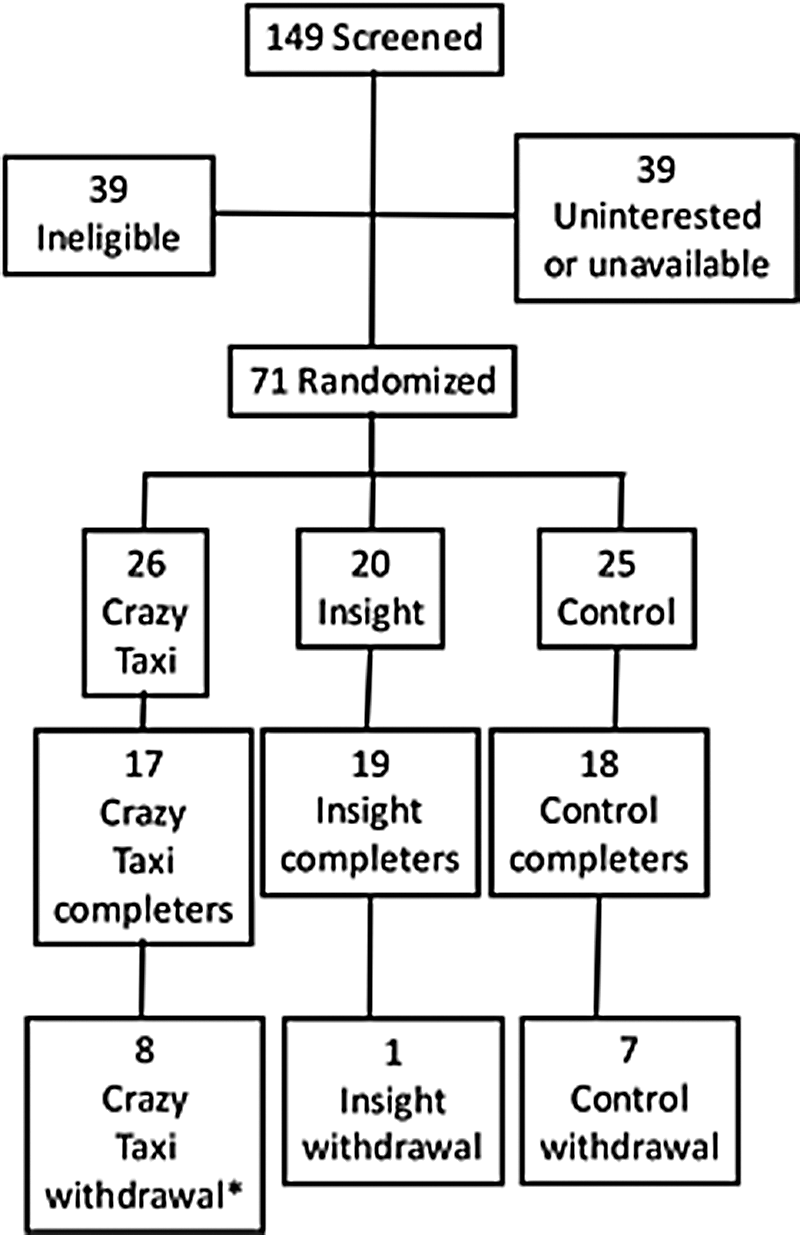
Flow of participants through the trial. *One participant dropped out after training had commenced.
Inclusion and exclusion
Inclusion criteria included the following: (a) 65 years of age or older, (b) Mini-Mental State Examination score of ≥24, 45 (c) little or no videogame usage in the past 6 months, 33 (d) distance visual acuity of 20/40 or better as assessed by a Goodlite Backlit Snellen chart, and (e) intention to be in the study region during the time of the study and to participate in a home-based training. Exclusion criteria included the following: (a) baseline scores of ≤120 on the UAB UFOV task 3 (Selective Attention subtask). This represented an endpoint far better (50 milliseconds) than what was achieved by most trained participants in either two previous intervention studies9,39; (b) participants reporting a history of significant motion sickness.
Measures
Measures were selected within a theoretical transfer hierarchy based on preliminary work. 9 Measures utilized with a detailed description are summarized in Table 1; references cited provide complete administration and psychometric details. Proximal outcomes were measures of skills gained in the training (i.e., game practice exercises), and thus provide a measure of training effectiveness. Primary outcomes were those measures of UFOV expected to be improved by either or both cognitive training 9 Secondary outcomes examined the breadth of transfer to (a) visual attention known to be influenced by videogames,31–33 (b) visuospatial skills, (c) everyday function known to improve by UFOV training, 13 and (d) subjective functioning that has been related to UFOV training. 9 A far-transfer outcome, verbal memory, was included to verify the specificity of training to the visual processing domain.
Description of Outcome Measures
For all tasks, higher scores are better, except for those indicated with an asterisk. The UAB UFOV and the road sign test were administered on a Toshiba Satellite Pro 480 CDT with 233MHZ “Tillamook” Pentium processor, running DOS 7.1 that force booted to a proprietary UFOV login shell. Participant responses were made on a 21-inch ELO CRT touchscreen. Four additional computerized tasks, including three MATLAB tasks (Rochester Useful Field of View, multiple object tracking, and attentional blink) and one PSYSCOPE task (Mental Rotation test), were administered on an iMac 2.66 GHz Intel Core Duo computer running OSX 10.5.8, which was connected to a 22-inch NECT MultiSync LCD225LXM touchscreen monitor. For all computer tasks, participants were seated 57 cm from the monitor and were asked to maintain this distance for the duration of the task. A standard computer keyboard was utilized to record responses for mental rotation. Crazy Taxi was administered on a PlayStation 2 attached to a 21-inch television monitor. All remaining measures were paper and pencil.
Design and procedure
This study compared videogame training with an active control group (InSight training; Posit Science, Inc.) and a no-treatment control group on several outcome measures. Assessments were performed at baseline, immediately after training (post-test) and 3 months later (follow-up).
Procedure
In laboratory orientation
After randomization, participants in the CT and InSight groups attended three or four individual, 1 hour in-laboratory sessions focused on game play (e.g., use of equipment and game mechanics). Manuals with step-by-step instructions on game play were developed for both videogame conditions. Once the trainers determined that participants had attained minimum competency, an in-home visit was scheduled, during which the game was set up, and game play in the home environment was practiced. Participants were instructed to keep logs documenting the start and stop time of each bout of training. Testers were blind to intervention condition.
Home-based protocol
Participants randomized to training groups were instructed to play their respective games for a total of 60 hours over a period of 3 months (5 hours a week, 1 hour a day). To monitor compliance with the training protocol, participants were asked to complete training logs each time they engaged in game play, and to send the logs weekly to the study office in postage-paid envelopes. Research assistants reviewed the logs, and telephoned participants to discuss situations of less-than-expected game play or stalled progress. Compliance is addressed below.
Training
CT is a driving game with key features that include rapid navigation through an urban environment, attending to speed and roadway features. The game was selected as an exemplar of “action videogames,” which may be distinguished from strategy or role-playing games by speed (objects pop in and out of the visual field, often at high velocity), elevated perceptual, cognitive and motor loads (e.g., monitoring multiple characters simultaneously), and having items of interest often presented at the periphery of the visual field and under divided attention conditions. In CT, game narrative is simple, and involves picking up passengers and dropping them off at their destination. Training first focused on simply driving through a field without braking to develop competency with the controller and game mechanics. CT includes eight “Crazy Boxes,” which are supplemental environments in which specific maneuvers are practiced. In each Crazy Box, participants practiced the given maneuver until they achieved a predefined criterion. From there, they proceeded to the main game environment (“the city”) and engaged in active game play, with the goal of picking up as many passengers and earning as much money (more money required further and more complicated drives) as possible. In later weeks, participants mostly practiced in the main game environment. In CT, feedback was minimal, and consisted of two in-game metrics: how many passengers were picked up, and how much money was earned. They received this feedback after every bout within the game. For InSight, task-specific performance feedback was offered; for example, how many bubbles were successfully tracked or how quickly a participant had responded to specific stimuli. They also received feedback after every bout within the game. The time of each bout depended on the performance of each participant.
InSight training has been described as a process-based intervention.46,47 Participants practiced the five InSight tasks (Table 1), which are visual and cognitive tasks. Training was aimed at improving processing speed and accuracy. The program offers an algorithm-controlled sequence of tasks, with the specific challenges set to a difficulty level and presentation speed that was adapted to participants' performance. To estimate user's threshold, InSight uses a Bayesian maximum-likelihood algorithm (Zippy Estimation by Sequential Testing [ZEST]). This adaptive algorithm uses a prior response to estimate a threshold, and this ensures that the difficulty level is adapted to participant's skills. All training is performed at the 85% correct level of the psychometric functional estimated by ZEST algorithm. Performance is monitored at baseline, before, during, and after training. “There are threshold measurements using a double randomly-interleaved ZEST algorithm set at 50% plus half the distance between the randomly correct level and 100% correct level (see equation below). The log-mean of the two ZESTs are used as the baseline measure. The threshold level is calculated as follows: ThreshLevel % = [(100–100/n)/2] + 100/n, where n is the number of choices on a trial” (page 19). A lapse rate of 5% (number of incorrect responses due to input errors) is also used. 48 More information about the InSight program can be found at www.brainhq.com/brain-training-products/insight
Equipment
Both games were lent to participants until the training period ended, and then equipment was returned to the study. After the 3 months follow-up was completed, we provided interested participants with details on how they could acquire the games and game systems used in the study.
No-treatment control group
Participants randomized to this group were assessed on all measures at baseline, post-test, and follow-up. This group was included to control for practice effects, as well as to monitor normative levels of change over time.
Statistical analyses
To evaluate the effects of intervention at the post-test and follow-up occasions, we adapted the procedures used by the ACTIVE study. 9 Specifically, a repeated-measures, mixed-effects analysis was conducted for each proximal, primary, and secondary outcome described above, focusing on group differences in initial change (from baseline to post-test) and in maintenance (from baseline to 3-month follow-ups). To control for Type I error and to focus on the specifically hypothesized effects, training group differences were examined not in omnibus but as the fixed effect of two orthogonal contrasts: (a) the mean of the two treatment groups (CT, InSight) was compared with that of the control group and (b) the mean of the CT group was compared with that of the InSight group. Hypotheses were tested by comparing these group difference contrasts on proximal, primary, and secondary outcomes at immediate post-test and 3-month follow-ups to baseline scores, yielding net differences. The net effect of the first contrast was defined as (change in the mean of training groups–change in the mean of control group). The net effect of the second contrast was defined as (change in the mean of CT group–change in the mean of InSight group). Results are expressed as effect sizes (i.e., difference in means divided by pooled baseline standard deviation) to allow direct comparison of different outcomes.
For this analysis, the repeated-measures model was fitted to the available data, ignoring missing data. To guard against violations of parametric assumptions, and following the practice of the ACTIVE study, 9 all dependent measures were pooled across study occasions, and then subjected to an inverse-normal transformation on rank-ordered scores using the Blom weighting approach. 49 Alpha criterion for significance was set at ≤0.05. Intent-to-treat analyses were used, meaning that all participants were included, even if their participation was less than prescribed.
Results
Compliance
Preliminary analyses examined compliance with interventions based on participant logs. There were four extreme outliers in self-reported participation: one low (CT) participant reported only 4.25 hours, and three high (two CT and one InSight) participants reported times of 277.6, 423.6, and 100.2 hours, respectively. Despite this, the groups did not differ significantly in time in training (P = 0.112). Excluding outliers, InSight participants reported an average of 66.2 hours in training (SD = 21.2, range = 23.7–95.9). CT participants reported an average of 72.4 hours in training (SD = 11.0, range = 53.8–97.2), and the groups did not differ, t(30) = 1.01, P = 0.32.
Training effects
Models comparing training groups at immediate post-test and at the 3-month follow-ups are shown in Table 2. Measure means, by group and occasion, are shown in Table 3. Figure 2 illustrates the 3-month trend for all outcomes that showed a group difference.
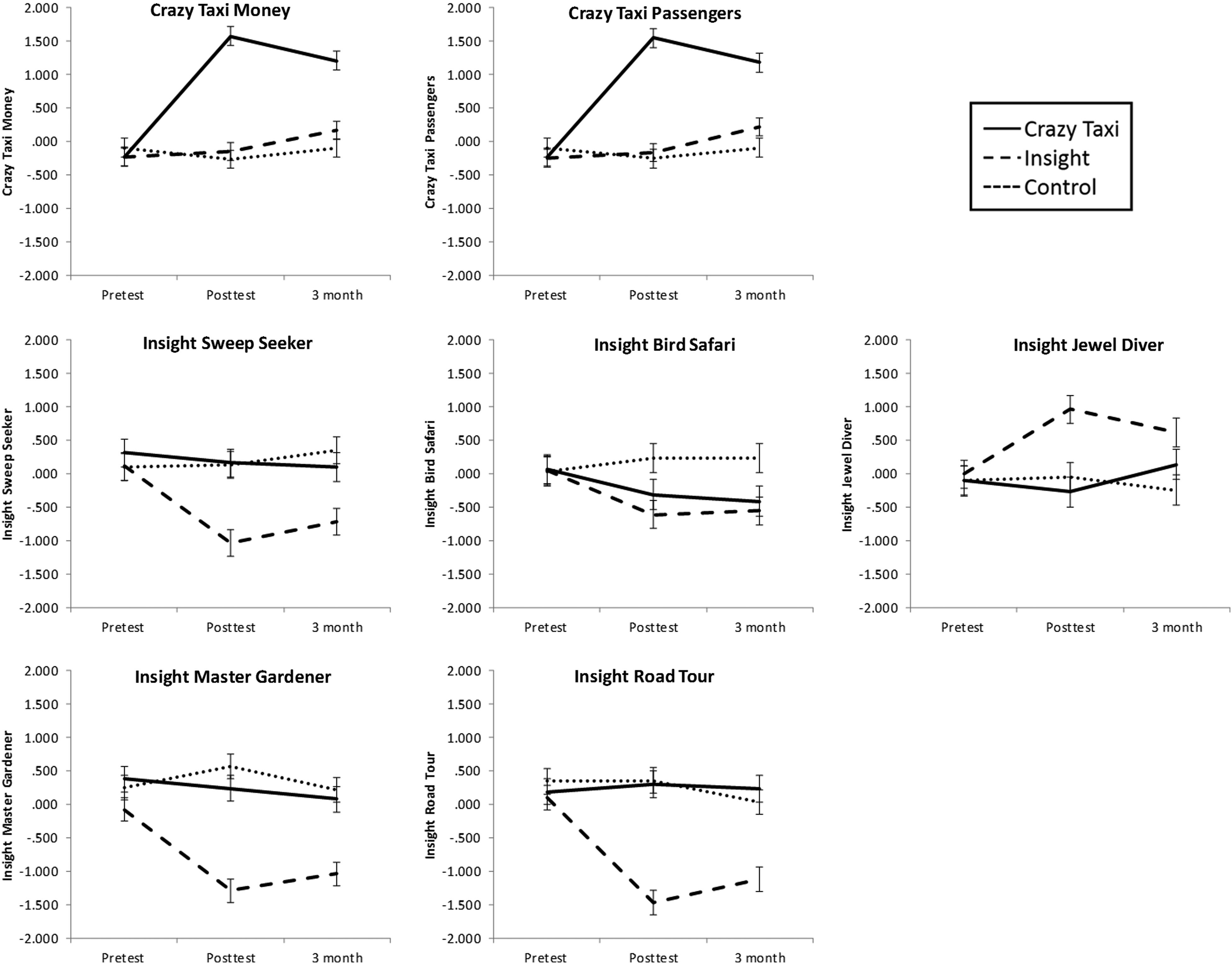
Outcome measures showing group differences over time. Values shown are for proximal, primary, and secondary outcomes that showed group differences in change. Values are Blom-normalized, z-transformed scores, standardized to an overall mean of 0 and standard deviation of 1. Error bars represent 95% confidence intervals of the difference.
Analysis of Immediate Training Gains and 3-Month Maintenance
Asterisked values are those that are significantly different from zero: * p < .05, ** p < .01, and ** p < .001.
Bolded values are significantly different from zero, p < .05.
Net effects represent standardized mean differences, where (mean change of Crazy Taxi, InSight) minus (mean change of control) are divided by pooled baseline standard deviation. Positive values indicate that training groups improved more than controls.
Net effects represent standardized mean differences, where (mean change of Crazy Taxi) minus (mean change of InSight) are divided by pooled baseline standard deviation. Positive values indicate that Crazy Taxi improved more than InSight.
Means and Standard Errors for All Study Outcomes by Occasion and Group
UFOV, Useful Field of View; JOLO, judgment of line orientation; IADL, instrumental activities of daily living; PANAS, positive and negative affect scale; HVLT, Hopkins verbal learning test; M, mean; SE, standard error.
Proximal outcome: Crazy Taxi
The average of the two training groups exceeded controls at immediate post-test (effect size, ES = 2.4), and the CT group exceeded the InSight group in passengers and money earned (ES = 3.6). The superiority of CT over InSight was maintained at the 3-month follow-ups with some effect dissipation (ES = 2).
Proximal outcome: InSight
For sweep seeker, jewel diver, master gardener, and road tour, the InSight group improved more than the other two at immediate post-test (ES range = 1.1–2.3) and at follow-up (ES range = 0.7–1.7). The jewel diver outcome no longer differed between InSight and CT groups at the 3-month follow-ups. For Bird Safari, both trained groups improved more than controls (ES = 0.9), but InSight and CT groups did not differ from one another at immediate post-test or follow-up.
Primary outcomes: UAB UFOV and Rochester UFOV
InSight improved more than CT at immediate follow-up (ES = 0.5, 0.7), and this difference was maintained at the 3-month follow-ups (ES = 0.6, 0.8).
Secondary outcomes
On the multiple object tracking outcome at immediate post-test, InSight improved more than CT (ES = 1.6) but not control; this difference disappeared by the 3-month follow-ups. For attentional blink at the immediate post-test, CT improved more than InSight (ES = 1.1) but not control. By 3 months, InSight had continued to improve, while CT had some effect dissipation, but both trained groups were now better than controls (ES = 0.9). For the Timed IADLs, neither treatment group differed from controls at the immediate post-test. By the 3-month follow-ups, both training groups had continued to improve and performed better than control (ES = 0.8) but did not differ from one another. Finally, for the Geriatric Depression scale, no groups differed at the immediate post-test, but by the 3-month follow-ups CT had continued to improve and now reported less depressive symptomatology than the InSight group (ES = 0.5).
Discussion
The REVIVA study demonstrated that participants could comply with and benefit from home-based interventions involving either computerized cognitive training or videogames. Both intervention conditions provided durable improvements (3 months) on their immediate targets of training. InSight training generalized to other measures of the trained ability (UFOV); CT-trained participants showed benefits in a variety of tasks (Bird Safari, attentional blink, and depression symptoms). Both treatments also showed benefits on a measure of Timed IADL. As such, the results replicate over a century of research across the life span, showing that most training effects are highly specific, and transfer only to outcome measures that overlap substantially with the trained skill.5,43,50–53
There are two ways to view the transfer patterns in this study: from one perspective, particularly for InSight training, multiple measures of visual attention showed gain after training, supporting the notion that the “true score” of the visual attention construct improved. From another perspective, apparent training represents nothing but generalized practice effects to other tasks with very similar task demands. These findings echo a century of similar findings, from Thorndike (1901) 49 to Owen (2010) 50 to, in older adults, the ACTIVE study. We argue that the common ground of both perspectives above is that cognitive training/practice produces highly specific effects (which are also often durable and of medium or larger effect size). Do such narrow training effects have practical value? By analogy, in the physical training and rehabilitation literature, isolating muscle groups and focusing on particularly focused outcomes (e.g., muscles supporting mobility after knee surgery) is often the goal of treatment. One could imagine, then, that cognitive training may be useful in a similar kind of “spot training”: it provides focused, specific, and durable gains in selected areas. We acknowledge that this comparison with physical training is reasoning by analogy, and only additional research can determine whether the training gains here have practice significance. In the context of a broader tool kit of cognitive intervention and rehabilitation strategies, some approaches might produce broader and less specific gains (e.g., complex activity engagement and physical exercise), and others may provide more focused improvements (e.g., cognitive training). In this study, we find that videogame benefits, if any, more closely resemble cognitive training (specific) than cognitive engagement. A growing body of studies examining the integration of narrower and broader intervention approaches may shed light on the costs and benefits of a diversified cognitive intervention tool kit.
The InSight results, in particular, show that targeted training improved multiple measures of UFOV and at least one measure of spatial distribution of visual attention (multiple object tracking), although the latter effect was small, and disappeared by 3 months. These results confirm that when the goal is to maximize specific gains in a narrow domain, it is hard to beat focused cognitive training.39,54 That said, we should not dismiss these findings of specificity as simply “teaching the test,” because in this study we found these UFOV improvements over three very different operationalizations from three different laboratories. In the language of classical test theory, it seems that InSight training improved the “true score” or latent construct of UFOV, and not just the practiced tests. A similar specificity was observed for CT, in that game players (only) got substantially better on multiple in-game performance metrics.
The study also confirmed that training effects in older adults can be durable. Effects found at the immediate post-test mostly persisted, with minimal dissipation, at the 3-month follow-ups. Given that other studies have found training maintenance for up to 10 years, 5 this study supports the idea that training-related improvements are not ephemeral.
Videogame training did appear to affect multiple outcomes. Bird Safari has participants respond quickly and accurately to birds in the periphery of a display. Task difficulty is increased by reducing the discriminability of birds, degrading visual conditions, and increasing speed of presentation. 47 As such, it is a clear measure of both processing speed and the spatial distribution of visual attention. This shares many surface features with a driving game, in which participants must quickly scan and respond to obstacles coming from the periphery of view at fast speed. Here, the classic “identical elements” of training and outcome likely promoted transfer of learning. It is noteworthy that for this task, gains from videogame training were not appreciably smaller than those seen in InSight.
The cognitive benefits of CT raise questions about the mechanisms by which a driving videogame might produce these improvements. Action videogames seem to foster a general improvement in the speed of processing, possibly because games demand fast nonstop decisions in rich dynamic environments.55,56 Games usually demand constant, divided attention. One study found that videogame players (VGPs) used broader visual search in virtual scenes than non-videogame players (NVGPs), who were more likely to persevere in a fixed zone. 57 VGPs also required fewer exposures to changing stimuli to detect their presence. These previously observed patterns are consistent with the improvements seen in Bird Safari, attentional blink, and Timed IADL, all of which required broad visual search and rapid decision making.
CT also appeared to produce improvements in depressed mood (better than those seen with InSight). These results, combined with Timed IADLs in particular, seem promising insofar as they suggest that videogames may help improve outcomes with real-world values (functioning and mood). The effect on depression bears similarity to the effects seen with a measure of engagement and flow,41,42 in that these outcomes suggest that game play made older participants feel more engaged and more positive, beyond any perceptual and cognitive benefits. To the extent that mood is an important element of quality of life, these affective improvements may not be trivial.58,59
Optimism regarding the meaning of findings in this study must be tempered by acknowledging several limitations. First, expectations for improvement were not measured, which means that we cannot be certain that some of the apparent intervention group differences (especially treatment vs. control) are not due to different levels of motivation and engagement. In addition, as is true for much cognitive aging research, the sample was small and positively selected (mostly white and mostly well educated). Attrition rates were fairly high; however, once enrolled in an intervention condition, all but one participant showed levels of compliance in accordance with, or in excess of, study training goals. In a study with so many outcomes (which we included to permit a breadth of evaluation), there is a risk of spurious findings by Type I error alone. The large number of statistical comparisons made here, despite the attempt to limit them through planned orthogonal contrasts without omnibus tests, means that some reported P-values <0.05 may be Type 1 error. Type 1 error may be a plausible explanation for “sleeper” effects (i.e., effects that do not emerge until the 3-month follow-ups). Future replications will be clearly needed. We tried to mitigate these concerns by using focused planned contrasts. There are relatively few positive findings that appeared to affect single outcomes at single occasions, lending support to the idea that effects identified as significant were real and durable. With two exceptions, all significant effects had effect sizes >0.7. We acknowledge that this speculation by anecdote may be specious, but we include it as a next step thinking about participant perception variables to collect in future research.
We believe that the larger consideration encouraged by this study is one of trade-offs between training gains and broader outcomes of intervention. For focused cognitive improvement, nothing beats cognitive training. But cognitive training, as deployed in this study, comes with costs: participants must have computers, tablets, or smartphones, and they also need to pay recurring costs for Internet and software subscriptions. Moreover, the overwhelming conclusion from over a century of cognitive training studies 52 is that programs like InSight represent a good investment for people with focal improvement goals that map onto what the programs offer. A surprising finding was that in two visual attention transfer outcomes (multiple object tracking and attentional blink), differences in immediate post-test emerged in part because one trained group improved (InSight and CT) while the other did not. While this may represent sampling fluctuation (which would also be surprising given the strong effect size of the difference between groups), it also raises the possibility that in some instances, some interventions may actually have negative effects on some outcomes (e.g., an intervention that emphasizes accuracy might produce poorer performance on a speed outcome). Indeed, a meta-analysis 68 found a trend for a negative impact of off-the-shelf games on cognition for older adults, likely because they were often too difficult. Future replications will be needed to further understand this effect.
In contrast, consistent with other studies from the engagement literature, videogame interventions may offer smaller, less focal gains as a secondary benefit of entertaining, engaging leisure pursuits.25–30 Moreover, they may more easily confer mood benefits (although UFOV training may also improve mood). In this study, we intentionally selected a very low-cost legacy game system that could be obtained at minimal cost, required no Internet, and (other than the console) used equipment already in the home. This suggests, to us, that gaming interventions may be more ubiquitously employed at lower cost, and might confer broader benefits for those who are not seeking to improve or remediate specific cognitive functions.
We have evidence from past studies that videogame playing might be more motivating and engaging than more traditional computer-based cognitive training.41,42 According to Weber et al., 24 the videogames may be especially gratifying when they facilitate a cognitive synchronization of specific attentional and reward networks under conditions of balance between challenge and skill. This study does not support the idea that this engagement translated to stronger cognitive gains or better compliance, but these earlier results do suggest that gamification of existing cognitive training could be one route to improve engagement.
Some outcomes (Timed IADL, Geriatric Depression Scale, attentional blink) showed apparent delayed effects, evinced in group differences that were not apparent until 3 months post-training. The ACTIVE study showed some delayed training transfer (self-rated IADLs did not differ between trained and control participants until 5 years post-training; motor vehicle crash rate differences emerged between some treatment groups and control participants 5 and 10 years post-training).2,5,11 One account for these delayed effects in the ACTIVE study was that trained participants might have experienced attenuated decline relative to controls, but this account is unlikely to explain 3-month follow-ups. We can only speculate, based on anecdotal reports from some participants, that their perceptual engagement with the world is altered by training, such that they regularly experience a broader attentional field of view and faster perception in everyday life. This speculation is untestable in this study, but may be a fruitful area for future research, as it could also help account for some of the delayed effects in the ACTIVE study.
In our previous study, we did find a modest effect of a first-person shooter game (Medal of Honor) on selective attention among older adults after 9 hours of training. In this study, we changed our videogame intervention to CT because the driving focus shared task characteristics with visual attention measures (fast paced, stimuli appearing at the periphery of complex displays at unpredictable times—so a need for divided attention in both time and space, as well as a need for focus attention at times), but the content of the game was less violent than Medal of Honor (a concern expressed by some participants in our previous study), and also required less learning of complex game scenarios and controller maneuvers (which could reduce time in active game play). Our choice of game served to reduce difficulty and complexity of game challenge, as indeed it has been reported that action videogames as defined by first- or third-person shooter games are too challenging for older adults and might present a substantial mismatch between the difficulty of the game play and the diminished perceptual, cognitive, and motor abilities that characterize the older age group, which might cause frustration instead of attentional learning. 68
At this stage, the literature on action videogames posits that at least three key processes need to be part of the training to enhance attentional control and thus performance on tasks such as the UFOV—these are a load on divided attention, the need to flexibly switch between divided and focused attention (as when precise aiming is needed) and the need to make decisions under time constraints. What is presently missing from the literature on game-based interventions when using commercially available titles is a clear method for characterizing what cognitive skills are trained by particular games, how to objectively quantify the level of difficulty, how to report the meaningful adaptive ladders that parametrically increase the level of challenge, as well as how to initiate inexperienced gamers into complex game mechanics. This is especially true when investigators deploy off-the-shelf games. Since games, game platforms, displays, and controllers/interfaces all continue to experience rapid technological evolution, attempts to objectively quantify these parameters seem essential for moving the field forward in a theoretically coherent way. It remains however a tall order.
Footnotes
Acknowledgments
This research was supported by the Robert Wood Johnson Foundation (RWJF) Grant 64441 to Patricia Belchior. P.B.'s work on the article was also supported by a Supplement to Enhance Diversity Grant U01-AG-014276-S1 to Michael Marsiske. Kelsey Thomas's work on the article was supported by the National Institute of Aging under Grant T32 AG020499.
Author Disclosure Statement
Karlene Ball owns stock in the Visual Awareness Research Group (formerly Visual Awareness, Inc.), and Posit Science, Inc., the companies that market the Useful Field of View Test and speed of processing training software (which includes the InSight training program). Posit Science acquired Visual Awareness, and Dr. Ball continues to collaborate on the design and testing of these Assessment and Training programs as a member of the Posit Science Scientific Advisory Board.