
Abstract
Abstract
Objective:
To evaluate the effects of 24-week exergame-based intervention on health-related quality of life (HRQoL) and pain in patients with fibromyalgia as well as to analyze the effectiveness of the intervention in subgroups of patients with different pain intensity levels.
Design:
Single-blinded, randomized controlled trial.
Setting:
University facilities
Participants:
Fifty-five women with fibromyalgia participated in the study.
Intervention:
The exercise group (EG) completed 24 weeks of exergames focused on mobility, postural control, upper and lower limbs coordination, aerobic fitness, and strength. A total of 120 minutes per week, divided into two sessions of 60 minutes, was completed.
Main outcome measures:
The Euroqol-5 Dimensions-5 Levels (EQ-5D-5L) was used to assess the HRQoL. In addition, pain intensity was measured using a visual analog scale (VAS).
Results:
Twenty-five out of 28 women allocated to the EG completed the intervention, which means an 89.29% of adherence. They were randomly divided into an exercise (age = 54.04 [8.45]) and a control group (52.72 [9.98]). Significant effects on the perceived health status and pain intensity (P < 0.05) were found. K-means clustering procedure revealed two groups with different response to the intervention. The respond group obtained significant effects of the exergame intervention in EQ-5D-5L, pain VAS, and VAS-EQ, compared with those who did not respond.
Conclusions:
Exergames could be a useful tool to improve perceived health status and pain intensity level in women with fibromyalgia with a reduced health-related quality of life.
Introduction
Fibromyalgia is a chronic disease characterized by general pain. It is commonly accompanied by other symptoms, such as fatigue, stiffness, or sleep disturbance. 1 These symptoms frequently cause a reduction in the ability to perform daily life activities2 diminishing the health-related quality of life (HRQoL) of fibromyalgia patients. 3
Physical exercise is the therapy with the highest level of evidence to reduce fibromyalgia symptoms. 4 Among the large variety of physical exercise types, virtual reality (VR) interventions have emerged as a promising therapy in different populations.5–7 In this regard, exergames are a nonimmersive variation of VR that involve physical exercise. 8
A systematic review and meta-analysis on the effect of exergames in patients with musculoskeletal pain indicated that exergames may reduce pain levels after the interventions. 9 In addition, exergame interventions have been introduced in patients with fibromyalgia.10,11 Results from these studies indicated that an exergame program based on Zumba and other mobility and gait tasks significantly improved mobility skills, HRQoL, and pain. However, the duration of these interventions was only 8 weeks, thus some adaptations may not be achieved in that short period of time.
The benefits of exergames could be higher than those achieved through traditional physical exercise in chronic pain patients. Specifically, the participant's attention may be focused on the virtual environment instead of in the pain they are feeling while performing exercise.12,13 Furthermore, a previous study showed that exergames may lead to similar physiological demands but lower perceived exertion and higher motivation compared with traditional gym-based exercise in healthy adults. 14 However, effects of physical exercise may depend on the characteristics of the subjects and a recent article discussed the idea of “nonresponders” and whether that absence of adaptation is global or modality specific. 15 Thus, cluster analyses may be adequate to identify the patient's profile who achieved or did not derive improvements from a specific intervention program. 16
Therefore, the aims of the present study were: (1) to evaluate the effects of a 24-week exergame-based intervention in the HRQoL and pain in patients with fibromyalgia, and (2) to analyze the effectiveness of the exergame intervention in subgroups based on the changes in the main variables (those who responded and those who did not).
Methods
Trial design
The present study was a single-blinded, randomized controlled trial. The sample was randomly divided into two groups: the exercise group (EG) and the control group (CG). All procedures were approved by the University Research Ethics Committee (approval number: 62/2017). The trial was prospectively registered at the International Standard Randomized Controlled Trial Number Registry (ISRCTN65034180). The protocol is available on the following website: https://doi.org/10.1186/ISRCTN65034180. This protocol is entitled “Effects of VR physical exercise program in brain and motor aging in fibromyalgia” and also included variables related to neuroscience (electroencephalography and Magnetic Resonance Imaging) and physical function.
Participants
The fibromyalgia impact questionnaire score was used to calculate the sample size. 17 A reduction of 14% in this questionnaire is clinically important according to Bennett, Bushmakin. 18 Data from previous studies conducted in Spain indicated that a mean (standard deviation) of 70.5 (11.8) in the fibromyalgia impact questionnaire was expected for this population. 19 Sample size calculation revealed that a minimum of 26 participants per group was required to detect between-group differences higher than 14% with an α value 0.05 and 85% of statistical power.
A total of 56 participants fulfilled the following inclusion criteria: (1) female and ages between 30 and 75 years, (2) able to communicate with the research staff, (3) have read and signed the written informed consent, and (4) diagnosed with fibromyalgia by a rheumatologist according to the 2010 American College of Rheumatology criteria. 1 The medical record was corroborated by one of the researchers. In addition, participants were excluded if they: (1) changed their usual care therapies during the 24 weeks of the treatment, (2) had contraindications for physical exercise programs or (3) were pregnant.
Participants were assigned random numbers and then they were randomly allocated into one of the two groups (EG and CG) by one of the researchers who did not participate in the data acquisition or statistical analysis. Pre- and post-evaluations were performed by another researcher who was blinded to the grouping allocation. Participants were not blinded since they were informed of the procedures and purposes and also knew whether they participated in the exercise intervention or not.
Interventions
EG participants completed 24 weeks of exercise intervention, whereas the CG continued with their usual daily life, including medication for those who were taking. The exercise intervention consisted of two sessions per week (1 hour per session). The intervention was carried out in the university facilities, in groups of two participants for each session.
The exercise intervention was based on an exergame: the VirtualEx-FM. This tool has been created specifically by the research group to improve the ability to perform daily life activities in patients with fibromyalgia. This exergame was previously used and the main characteristics are published. 11 The VirtualEx-FM fulfilled the eight key points to consider it as an adequate VR rehabilitation therapy. 20 It was conceived as a tool to improve the aerobic fitness, strength, mobility, postural control, and coordination of the upper and lower limbs. 11
A typical session contained: (1) a warm-up, where participants have to perform joint movements guided by a video made by a kinesiologist; (2) an aerobic component based on dance steps marked by a dance teacher; (3) postural control and coordination games, where participants have to reach an apple that appears and disappears in different locations near them. The body part that participants have to use to reach the apple is indicated by the software and can be manually controlled by the kinesiologist, and (4) a walking training, where the participant must comprise a virtual trail of footprints. The interface allows the selection of different types of steps (normal, tiptoe, heel walking, raised heels, and raised knees). More details of the VirtualEx-FM are available in Collado-Mateo et al.10,11
Outcomes
The main outcome measures was the Euroqol-5 Dimensions-5 Levels (EQ-5D-5L), which was used to measure the HRQoL. 21 It is comprised of five dimensions (mobility, self-care, daily life activities, pain or discomfort, and anxiety or depression) and five levels per dimension. The EQ-5D-5L utility index was calculated before and after the intervention. The EQ-5D-5L also includes a visual analog scale (VAS), which evaluates the perceived health status from 0 (the worst health they can imagine) to 100 (the best health they can imagine).
As a secondary outcome, a VAS for pain (0–100), referring to the day they were evaluated, was used to measure the intensity of pain.
Statistical analyses
The SPSS statistical package (version 20.0; SPSS, Inc., Chicago, IL) was used to analyze the data.
Parametric tests were conducted since data followed a normal distribution based on the results of Shapiro–Wilk and Kolmogorov–Smirnov tests. Levene's test and t-test for independent measures were conducted to examine differences between groups at baseline. Repeated measures analysis of variance (ANOVA) tests, with Bonferroni corrections for multiple comparisons, were conducted to explore the effects of the intervention program in HRQoL, pain intensity, and subjective perception of health. In addition, the K-means clustering procedure was employed to group participants who similarly respond to the exergame intervention, using the Euclidean distance as a measure of proximity. The cluster analysis was conducted taking into account the differences between post and pre values of EQ-5D-5L, pain VAS and VAS-EQ which were previously standardized (Z-score). Two clusters were created to classify the participants according to their improvements in the exergame intervention (those who responded and those who did not). Repeated measures ANOVA tests, with Bonferroni corrections for multiple comparisons, were used to compare the cluster subgroups in the defined subgroups.
Data from all 55 initial participants were used to conduct the intention-to-treat analysis by multiple imputation (MI) of missing values following the Sterne, White 22 guidelines. Our missing data were classified as missing at random. The R software and Amelia II package 23 were used for MI of data.
Partial eta-squared effect size was reported for each statistical test. 24 According to Cohen, 25 effect sizes could be classified as small (0.01 ≤ η2 < 0.06), medium (0.06 ≤ η2 < 0.14), and large (η2 ≥ 0.14).
Results
Figure 1 represents the flow diagram of the participants. A total of 56 patients with fibromyalgia were screened for eligibility. One woman was excluded for not meeting with the inclusion criteria. Lastly, 55 women were randomized into two groups, EG and CG. Regarding the compliance with the treatment, three women allocated in the EG and two in the CG were lost to follow-up. In the EG, the causes were a surgery unrelated to the exercise intervention (n = 1) and the lack of time (n = 2). In the CG, two women were not able to attend the final evaluations. The intervention was considered as completed when the participant attended a minimum of 75% of the hours. Thus, considering this criterion, the final adherence was of 89.28%. No side effects, derived from the intervention, were detected.
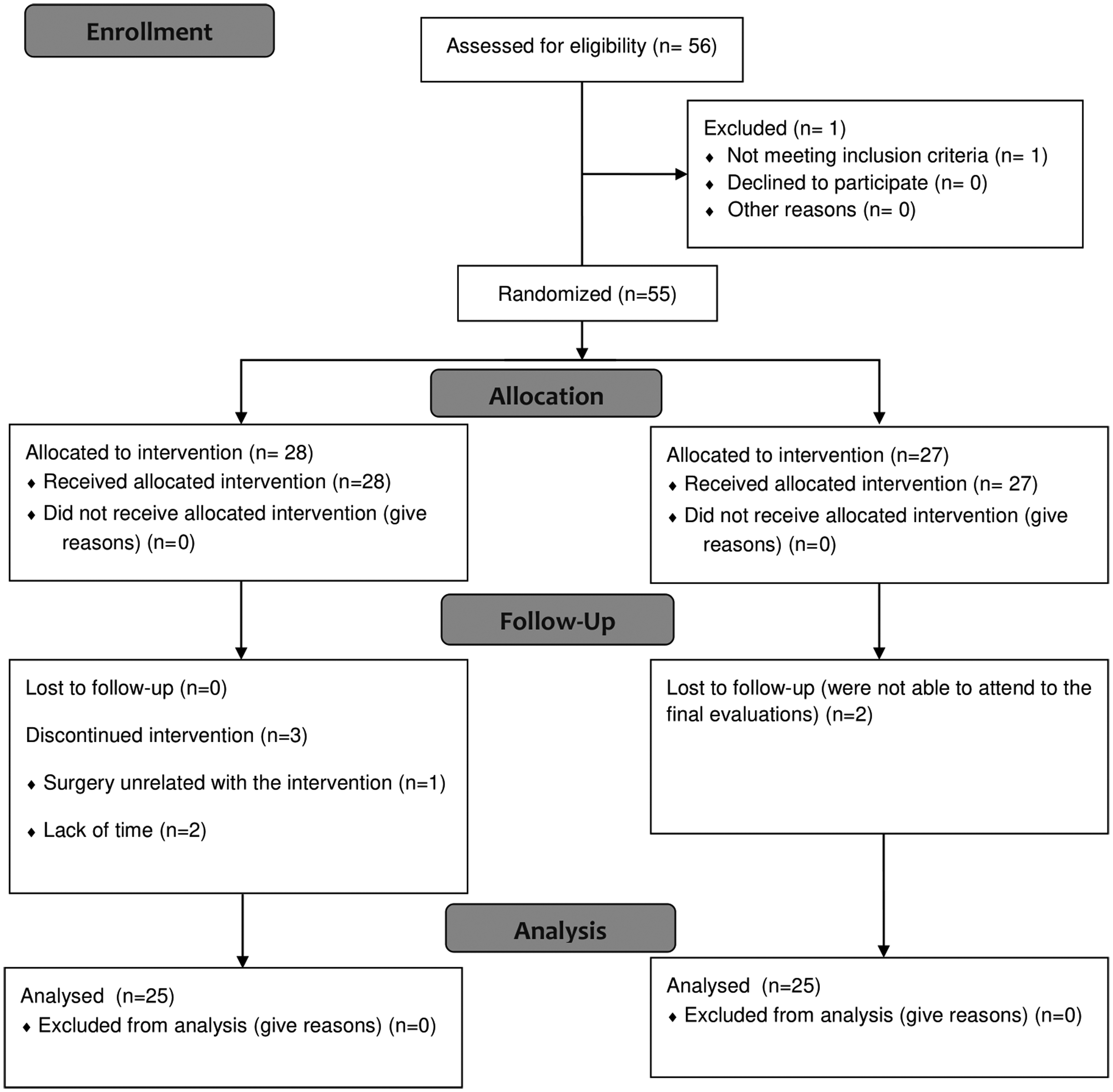
Flow diagram of the participants.
Table 1 summarizes the main characteristics of both groups at baseline. Significant differences were reported neither of age nor the main outcomes (EQ-5D-5L, VAS-pain and VAS-EQ).
Demographic Data and Differences Between Groups at Baseline of Fibromyalgia Patients
P-values of t-tests for independent sample to compare differences between groups at baseline.
EQ-5D-5L, Euroqol-5 Dimensions-5 Levels; SD, standard deviation; VAS, Visual analog scale.
Effects of the intervention programs and the intent-to-treat analysis are presented in Tables 2 and 3, respectively. Repeated measures ANOVA showed significant effects (P-value <0.05) in the health perception and pain intensity measured using VAS (both classified as medium according to its effect sizes). Regarding to the pain intensity (VAS), eight women (28.57%) of the EG reached a clinically relevant reduction of pain 26 (more than 20%), seven (25% of the EG participants) between 10% and 19%, and four (14.28%) between 0% and 9%. In the CG, only three participants (11.11%) were able to clinically reduce their pain level, two participants (7.41%) reduced their level between 10% and 19%, and seven (25.92%) between 0% and 9%. No significant effects were found for the HRQoL utility index.
Effects of Exergame Intervention in Patients with Fibromyalgia in Health Perception, EQ-5D-5L Utility Score, and Pain
P-values of repeated measures ANOVA to compare differences between groups after a 24-week exergame intervention.
ANOVA, analysis of variance.
Intent-to-Treat Analysis of the Effects of Exergame Intervention in Patients with Fibromyalgia in Health Perception, EQ-5D-5L Utility Score, and Pain
P-values of repeated measures ANOVA to compare differences between groups after a 24-week exergame intervention.
Results of the clustering procedure revealed two groups: responded (n = 12) and did not respond (n = 16). Table 4 showed the characteristics at baseline in these subgroups. Participants who responded to the intervention had significantly lower EQ-5D-5L score at baseline compared with the did not respond group (Table 4). Repeated measures ANOVA showed differences (classified as large according to its effect sizes) in the effects of the intervention between groups in pain (VAS), VAS EQ-5D, and EQ-5D-5L (Table 5). Mean values, at baseline, indicate that the effectiveness of the exergame intervention is greater in those women with fibromyalgia with worse HRQoL, health perception, and pain at baseline (Table 5).
Differences Between Groups at Baseline of Fibromyalgia Patients Who Responded or Did Not to the Exergame Intervention
P-values of t-tests for independent sample to compare differences between groups at baseline.
FIQ, Fibromyalgia Impact Questionnaire.
Effects of the Intervention in Two Groups of Participants (Responded vs. Did Not Respond) After K-Means Clustering Procedure
P-values of repeated measures ANOVA to compare differences between groups after a 24-week exergame intervention.
Discussion
The present study is the first randomized controlled trial with a duration of 24 weeks, which examined the effects of an exergame intervention in the HRQoL and pain intensity. Overall, the program was effective at improving perceived health status and pain. In addition, the response to the intervention seemed to be greater in those patients which present worse values of HRQol at baseline.
Results indicated that VirtualEx-FM improved the perceived health status measured by the EQ-5D-5L VAS. This is in line with the results obtained by Collado-Mateo et al. 11 in a previous 8 weeks randomized controlled trial using exergames. They reported improvements in the EQ-5D-5L health utility, perceived health status using VAS, and three dimensions of the EQ-5D-5L (mobility, pain and discomfort, anxiety and depression). Moreover, other intervention based on aquatic training, 27 dance, 28 or stretching intervention 29 have reported increments in the HRQoL. However, improvement in utility index of the EQ-5D-5L was not detected in our intervention, which might point out that exergame effects take place during the first weeks of the program but, after that, there could be a reduction in the motivation that might lead to a maintenance or even to a worsening of the effects. Although hypothetical, results from the current study and the previous using the same program 11 might indicate that the dimensions of “self-care” and “usual activities” are not improved after the intervention regardless of the levels of pain and problems at baseline. This could partially explain why significant improvements were observed in the health VAS and not in the EQ-5D-5L utility index, which is calculated considering those two unchanged dimensions. Furthermore, it must be noted that significant differences in health VAS are mainly due to the decrease in the CG (22%). This reduction is similar to the one observed by Andrade and Zamuner 30 on the wellbeing and pain VAS. This decrease could be related to the absence of a placebo. In this regard, women in the CG knew that they belong to that group and also they knew that some of their colleagues from the association were participating in the program. Although hypothetically, this could be a limitation of the current study, and may make that results must be taken with caution.
In line with the results mentioned above, a significant effect in pain intensity measured using VAS was found after the intervention. Since pain is the main symptom of fibromyalgia, the obtained result is remarkable. Collado-Mateo et al. 11 reported a significant reduction of pain after an 8-week intervention based on VR in fibromyalgia. In that study, the effect size achieved in the pain dimension of the EQ-5D-5L was 0.059, which is low according to Cohen 25 The effect size observed in the current study analyzing the whole sample was also low. However, the subgroup analysis revealed that in the respond group, the reduction of pain was large (partial eta squared higher than 0.14). Therefore, the improvements in pain seemed to be low in the 8- and 24-week studies, but results from the subgroup analysis may reveal a potentially large improvement when patients suffer from high levels of pain at baseline.
The protocol of the current study involved dancing movements (Zumba). In this regard, a recent systematic review and meta-analysis evaluated the research on the effects of dance interventions on pain and observed that artistic and creative dance programs may be useful to reduce pain. 31 However, that review did not include those interventions based on the repetition of rhythmic movements such as Zumba. Therefore, the current study supports the potential benefits of dance interventions not only when movements are creative or artistic, but also when the simple repetition of dance movements is required. Future studies might explore the potential of artistic intervention conducted on VR environments.
Regarding VR and exergames, the potential of these interventions has been reported in other population with chronic pain after exercise interventions based on VR.32–34 Furthermore, it must be noted that the current study and also the previous one involving an intervention of 8 weeks reported an excellent adherence in terms of the proportion of participants completing the intervention. However, the adherence in the 24-week intervention was reduced from 98% to 89%, which might indicate that the motivation of participants was not fully maintained when the duration of the intervention was increased. This is only hypothetical since motivation was not measured in the current study. However, this variable is known to be crucial in women with fibromyalgia since the adherence to physical exercise is often poor.35,36 Although the current study achieved good levels of adherence, future studies should also explore whether motivation to practice can be maintained for several months in exergame interventions.
Fibromyalgia is a heterogeneous disease with different subgroups of patients suffering from different impacts of the disease. 37 This is the main reason why the study of subgroups is strongly recommended in fibromyalgia.37,38 Thus, Estévez-López, and Segura-Jiménez 38 considered it important to know whether the effectiveness of the intervention is different across different patient's profiles. Following the future directions of the previous research, 38 we studied the effects of exergame intervention in patients with different levels of pain level. Two subgroups of participants were created by the K-means clustering procedure, taking into account the effects in EQ-5D-5L, pain VAS, and VAS-EQ. Interestingly, it seemed that those participants with worse values of HRQoL (P < 0.05), pain (P = 0.096), and health perception (P = 0.066) at baseline are those who obtained greater effects in this exergame intervention. Therefore, depending on the initial score of HRQoL, we could expect one effect or another derived from the exergame intervention. Probably, this exergame tool would be more effective in those participants with higher values of pain and lower health perception since there was a high presence of mobility, postural control, and coordination of the upper and lower limbs in the exergame tool 11 and improvements in these variables are closely related with HRQoL. Future studies may also include other variables to incorporate subgroups according to other physical and psychological variables. In this regard, a previous study showed that high levels of physical fitness along with positive affect may be associated with lower levels of fatigue. 39 Thus, this would be of interest in studies aimed to evaluate the effects of physical exercise interventions.
However, the present study has some limitations and strengths that should be mentioned. First, in this study, only women participated, so we cannot generalize the results to male fibromyalgia patients. Second, the lack of a group who performed a traditional exercise training (not based on VR) makes that the effects of VR intervention should been taken with caution. Third, the relatively small sample size may affect the comparisons and might have caused that only great differences have reached the statistical significance level. However, this is the first study with a long intervention (6 months), which evaluates the effects of an innovative tool, the exergames, on the HRQoL and pain in women with fibromyalgia. Moreover, for the first time, the effectiveness of exergames was compared in subgroups of women with fibromyalgia who responded or did not respond to the exergame program.
Conclusions
VirtualEx-FM may be an effective tool to improve HRQoL perception as well as to reduce the pain intensity in women with fibromyalgia. Subgroup analyses showed that those women with fibromyalgia with worse values of HRQoL at baseline were those who respond to the exergame intervention.
Footnotes
Acknowledgments
Th authors acknowledge the Extremadura Association of Fibromyalgia (AFIBROEX) in Cáceres (Spain) for helping to recruit the participants for this study.
Funding
This study was co-funded by the Spanish Ministry of Economy and Competitiveness (reference no DEP2015-70356) in the framework of the Spanish National R+D+i Plan. This study was also funded by the Research Grant for Groups (GR18155) funded by Junta de Extremadura (Regional Government of Extremadura) and European Regional Development Fund (ERDF/FEDER) “a way of doing Europe”.
Author Disclosure Statement
The author S.V. was supported by a grant from the regional department of economy and infrastructure of the Government of Extremadura and the European Social Fund (PD16008). The funders played no role in the study design, the data collection and analysis, the decision to publish, or the preparation of the article.