
Abstract
Objective:
This article presents the results of a systematic review of the latest, state-of-the-art research on videogames designed for older adults (i.e., those aged 65 or older) and the health benefits derived from playing these games. Findings from each study that met the inclusion criteria were analyzed and summarized into emergent themes to determine the impact of digital games in promoting healthy behaviors and benefits among these older adults.
Materials and Methods:
Five databases (PubMed, ScienceDirect, IEEE Xplore, ACM Digital Library, and Google Scholar) were searched for studies that evaluated interventions of videogames for older adults aged 65 and older. The initial search yielded 806 articles. After evaluating them against the inclusion criteria, 23 studies remained.
Results:
Out of the 23 studies we reviewed, 20 reported the significant impact of videogame interventions on the elderly's physical health. In addition, 14 studies reported effects on the elderly's mental health. Exergame is the most popular type of game used in these videogame-based interventions. This review also includes the details of study design (e.g., type of intervention, length, frequency), population sample, and measurements used in the studies.
Conclusions:
This systematic review demonstrates that videogame-based interventions are helpful in promoting physical health (i.e., balance, mobility, strength, physical fitness, and walking performance/gait parameters) and mental health (i.e., balance confidence, executive functions, reaction time, and processing speed) among older adults. It can also be used by researchers in this field to inform their design decisions. We have listed guidelines that can be used to frame future research in the area and enhance its quality.
Introduction
With significant advances in health care and increased life expectancy in the past few decades, the population of older adults has been growing rapidly. According to the World Health Organization, the population of adults aged 65 or older in 2015 accounted for 8.5% of the world population. This number is expected to double by 2050, reaching 16.7% or 1565.8 million. 1
People are likely to experience some degree of age-related changes when they turn 65. Evidence suggests that age-related decline includes, but is not limited to, decrements in gait parameters, 2 motor control, 3 and cognition. 4 In addition, age-related illnesses (e.g., Alzheimer's disease) are another aspect that can contribute to the frailty of older adults. These age-related changes tend to affect their health-related quality of life (HRQOL), which includes the quality of physical, mental, and social functions of a person's life.5–7 Certain age-related changes and diseases could be slowed down or even reversed after specific training or interventions, whereas other age-related declines are consequences of unhealthy lifestyles (e.g., physical inactivity that could lead to type 2 diabetes), 8 which can be changed when there is early awareness, a suitable environment, and right motivation.
Various countermeasures have been set up to tackle these declines, foster healthy aging, improve HRQOL, and hence promote a healthy lifestyle. Mikus et al. 8 have shown that being physically more active by taking more steps could contribute to reducing the risk of developing type 2 diabetes. In addition, older adults who carry out physical activities can slow down their physical decline and decondition.9,10 Taking memory training exercises could help older adults to ameliorate memory loss and its associated issues 11 and equip them with strategies 12 to cope with situations in the event that loss of memory occurs.
Recently, there has been an increasing trend to convert these training programs into videogames, because research13–16 has shown their potential to improve physical ability (e.g., gait parameters) and cognitive performance (e.g., attention). Exergames, a type of game that requires physical activities, has become one of the most used game types for such game-based interventions. These games are aimed at helping to overcome several of the reported barriers for older users to do physical activities as they make them more appealing and can engage a broad audience across different age groups. 17
Contribution
The main contribution of this systematic review is to analyze the latest, state-of-the-art research on the use of videogames for promoting HRQOL (i.e., physical, mental, social health benefits) among the aging population. We have been able to extract key details of the study design, type of games used in the interventions, health measurements, and results from relevant papers. Although review papers with the same focus exist in the literature, the last one was published in 201118 (i.e., 9 years ago). Since then, there have been rapid advances in gaming technologies and, as such, it is important to explore what the latest research shows and where it is heading toward. Our review led to finding 21 articles published after 2011. In addition, this review differs from the previous one, 18 in that it only examined studies with participants older than 65. Studies with younger populations were excluded.
Materials and Methods
The structure and sequence of this review follows the PRISMA 19 guidelines.
Eligibility criteria
To be included in this systematic review, the publication was required to: (1) have used a videogame to promote an HRQOL (physical, mental, and/or social); (2) have been written in English and appeared in a professional peer-reviewed journal or conference; (3) have recruited participants that are 65 or older; (4) have involved both genders for analysis to reduce bias; and (5) have been rated at least to be of “moderate quality” based on the Quality Assessment Tool for Quantitative Studies. 20 No additional exclusionary criteria were employed.
Information sources and search strategy
Articles were extracted in April 2018 by using five databases (PubMed, ScienceDirect, IEEE Xplore, ACM Digital Library, and Google Scholar). Keywords were identified based on previous reviews on the use of videogames to elicit health benefits.18,21,22
Keywords for Game were: “Digital,” “Video,” “Digital video,” “Computer,” “Virtual,” “Mobile,” “Arcade,” “Handheld,” “Casual,” “Serious,” “Virtual reality,” “Augmented Reality,” “Interactive,” “Health,” “Simulation,” “Online,” “Console,” “Persuasive,” “Action-adventure,” “Sports,” “Escape,” “First person shooter,” “Third person shooter,” “Role-playing,” “Real-time strategy,” “Medieval,” “Adventuring”; for Older adult were: “Older adult,” “Aged,” “Elderly,” “Senior,” “Aging,” “Aging,” “Aged people,” “Older people,” “Geriatrics”; and for health related were: “Fall,” “Balance,” “Cogniti*,” “Mental,” “Physical,” “Social,” “Psychological,” “Exercise,” “Anxiety,” “Depression,” “Social isolation,” “Rehabilitation,” “Musculoskeletal,” “Stroke,” “Movement disorder.”
The following combinations of keywords were used across the selected search engines: Digital or Video or Digital video or Computer or Virtual or Mobile or Arcade or Handheld or Casual or Serious or Virtual reality or Augmented Reality or Interactive or Health or Simulation or Online or Console or Persuasive or Action-adventure or Sports or Escape or First person shooter or Third person shooter or Role-playing or Real-time strategy or Medieval or Adventuring AND Gam* AND Older adult or Aged or Elderly or Senior or Aging or Aging or Aged people or Older people or Geriatrics AND Fall or Balance or Cognitive or Cognition or Mental or Physical or Social or Psychological or Exercise or Anxiety or Depression or Social isolation or Rehabilitation or Musculoskeletal or Stroke or Movement disorder.
Selection of studies
The selection was performed through four rounds. In the first round, duplications were identified and removed. A screening of their abstract was done in the second round where articles that did not meet the eligibility criteria (1–4) were removed. Eligibility criteria (1–4) were used again in the third round, where articles were assessed through reading the whole article. In the fourth round, a quality assessment for each article was conducted by using the Quality Assessment Tool for Quantitative Studies, 20 where articles rated below “moderate quality” were excluded.
Data items
Each row in Tables 1 and 2 refers to a different study. The studies were summarized based on first author, description of the study, year, research design (design, duration of intervention, frequency, duration of play, setting), sample-related (sample size, dropout rate, age, gender), type of game and platform used, gaming devices, measurements of the study relevant for health, and results (Table 1). The bias risks are summarized regarding selection bias, study design, confounders, blinding, data-collection method, withdrawals, and an overall rating (Table 2). The second author helped to re-assess all items.
Results of the Literature Survey on the Health Benefits of Videogames for the Aging Population
10-MWT, 10-meter Walk Test; 6-MWT, 6-minute walk test; ABC, activities-specific balance confidence scale; ACG, active control group; AG, active group; ANT, attentional network test; B/A, ratio score of B and A; BBS, berg balance scale; CG, control group; COP, center of pressure; COPE, centre of pressure excursion; CSRT, choice stepping reaction time; DSST, digital symbol substitution task; DT, dual tasks; EEG, electroencephalogram; ETGUG, extended timed get-up-and-go; FAB, Fullerton advanced balance; FES-I, falls efficacy scale international questionnaire; FPA, foot place accuracy; FRT, functional reach test; FSST, four square step test; FTSS, five times sit to stand; GDS, geriatric depression scale; HECG, healthy elderly control group; Icon-FES, iconographical fall-efficacy scale; IG, intervention group; IMVC, isometric maximal voluntary contraction; IPAQ, international physical activity questionnaire-short form; IRFD, isometric rate of force development; LOS, limits of stability; MemoryG, memory group; MFES, modified falls efficacy scale; MMSE, mini mental state examination; MoCA, montreal cognitive assessment; MT, movement time; NDG, neurodegenerative diseases group; PFC, prefrontal cortex; PHQ-9, patient health questionnaire; POMA, Tinetti performance-oriented mobility assessment; RCT, randomized controlled trial; RT, reaction time; SA, sway area; SAFFE, Survey of Activities and Fear of Falling in the Elderly; SCB, Short Cognitive Battery; SCWT, Stroop Color and Word Test; SF-36, 36-Item Short Form Survey; ShamG, Sham group; SPPB, short physical performance battery; ST, single task; SV, sway velocity; TAP, test battery for attentional performance; TMM, total muscle mass; TMT-A, trail making test part A; TMT-B, trail making test part B; TUG, time up and go; UST, unipedal stance test; VVC, visual-vestibular condition; WMS-R, Wechsler Memory Scale-Revised; XMSS, xavix measured step system.
Risk of Bias, Quality of Research Indicators of Each Study
, weak quality; **, moderate quality; ***, high quality.
Risk of bias in individual studies
This review includes a qualitative analysis for articles that passed the quantitative exclusion, which was performed by using the Quality Assessment Tool for Quantitative Studies. 20
The quality assessment comprised six components: (1) selection bias, (2) study design, (3) confounders, (4) blinding, (5) data-collection method, and (6) withdrawals and drop-outs. Each component was rated as weak, moderate, or strong, and a final rating was made for each study. A study was rated as “low quality” if it had received two or more weak ratings; “moderate quality” if it had received one weak rating; and “high quality” if it had not received any weak ratings. Any discrepancies in terms of rating were resolved between the two reviewers. The resulting studies can be found in Table 2.
It was not possible to conduct a meta-analysis, because the number of papers dealing with a specific outcome did not meet the theoretical minimum (i.e., 2). According to a previous study, 23 “in practice, 5 or more studies are needed to reasonably consistently achieve powers from random-effects meta-analyses that are greater than the studies that contribute to them.” The papers that were selected based on our review requirements did not meet this condition.
Results
Study selection
The systematic inclusion process included 806 papers (218 from PubMed, 113 from ScienceDirect, 269 from IEEE Xplore, 94 from ACM Digital Library, and 112 from Google Scholar). After distilling them through inclusion and exclusion criteria, 23 papers were included in the final review and summarized in Table 1. The study selection process is summarized in Figure 1. After removing the duplicates (N = 23), 783 articles were obtained. In the first round of screening the abstract, we excluded 660 papers because they were (1) not written in English (N = 14), (2) out of scope of current review (e.g., they were editorials, workshops, opinions, study protocols, reports, surveys, and reviews). In total, 123 articles were included after screening their titles and abstracts.
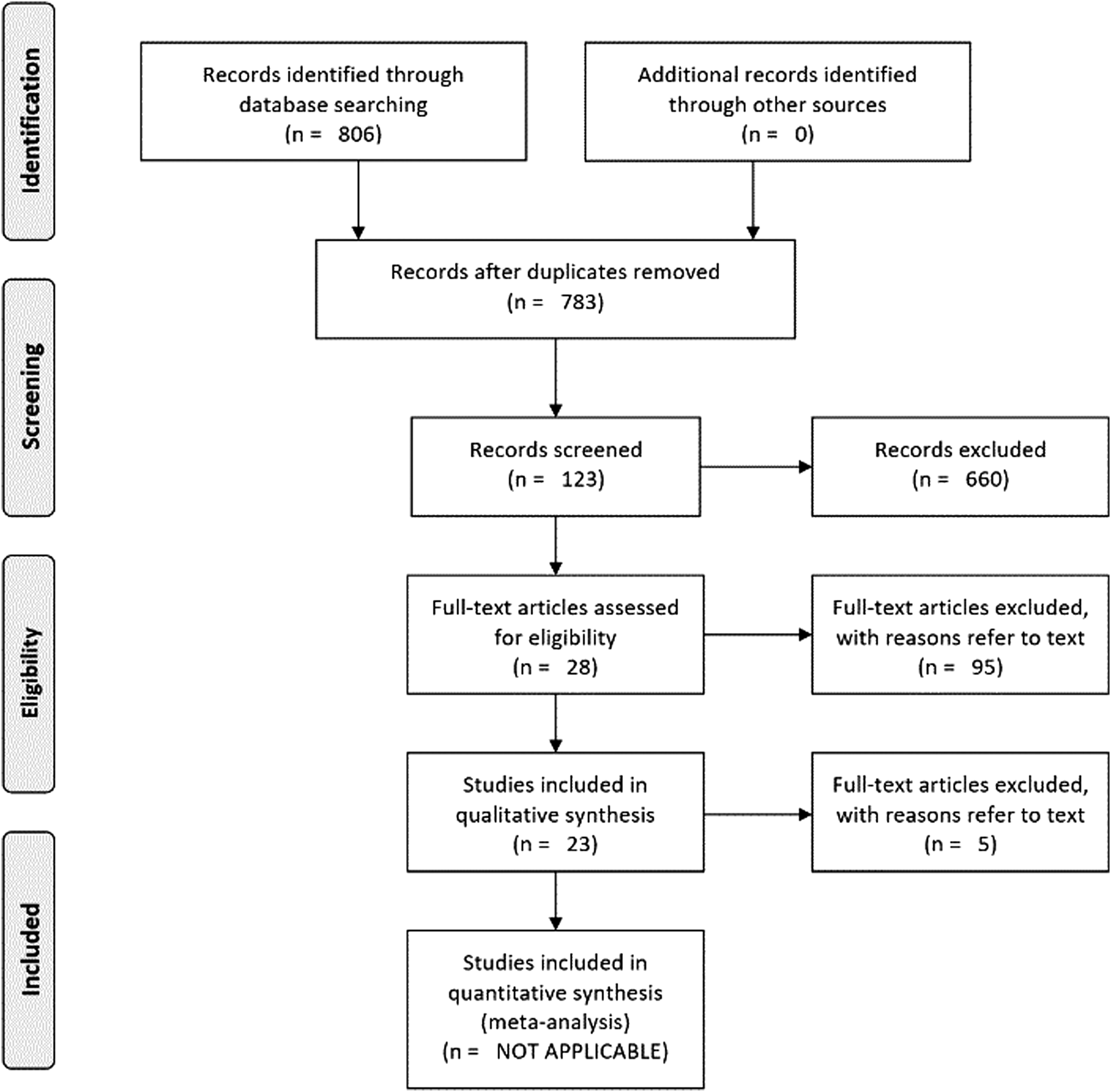
Flow diagram of the inclusion process of the studies.
Further exclusion included the removal of studies that (1) involved participants aged <65 (N = 49); (2) recruited participants of a single gender or did not mention gender in their study (N = 19); (3) failed to explicitly measure and report participants' health outcomes p > 0.05 or did not focus on health issues (N = 24); and (4) did not solely use digital videogames in their intervention (N = 3).
In the last round, we excluded five articles that were rated “low quality” by the Quality Assessment Tool for Quantitative Studies. 20
Study characteristics and risk of bias within studies
The first article identified was published in 1997, with the number of articles increased significantly to 23 since 2010 when interactive technologies such as Kinect and Nintendo® Wii™ became popular.
The quality of research bias of individual trials was rated either “moderate quality” or “high quality,” where 9 of them were rated “high quality” and 14 of them “moderate quality.” The results are summarized in Table 2.
Studies selected
The number of studies that reported having physical and mental health outcomes after an intervention was 20 and 18, respectively. We did not find any studies reporting social benefits or outcomes based on our inclusion criteria. We next separated the benefits into physical and mental, and then further divided them into sub-sections. For each sub-section, we reported how many studies successfully outlined the corresponding outcome, length of the intervention, and most used assessment/device for such outcome. In addition, we included the studies showing that a videogame-based intervention was superior to an alternative active training program (e.g., physical training program) at the end of each outcome.
Physical functioning benefits
Physical functioning benefits were elicited in all studies that measured physical health. Results of the physical benefits of playing videogame are summarized next.
Balance
There were nine studies24–32 (intervention length: 4–12 hours; M = 6.78) that found that playing videogames could improve the balance (both static and dynamic) of elderly users. The Berg balance scale (N = 3) and functional reach test (FRT) (N = 3) were the most used assessor-led clinical tests for assessing balance performance in these studies.
Physical fitness/functional fitness/frailty
Four studies33–36 (intervention length: 3–24 hours; M = 12.25) have found improvements in physical fitness among older adults after playing videogames. Short Physical Performance Battery 37 (SPPB), which comprises a balance test, a 4-meter Walk test, and a five Chair-Rises tests, was the most used assessment test for physical fitness (N = 4). The SPPB is also a validated measurement in detecting frailty of these users. 38
Strength
The outcome of improved strength (upper limb strength, lower limb strength, leg strength and endurance, muscle power) was supported in four studies24,29,39,40 (intervention length: 6–12 hours; M = 9.89). Strength was commonly assessed by some external devices such as force plates, dynamometers, and press devices. Lower limb strength was reported the most among these studies (N = 2).
Gait parameters and walking mobility
Improvements in gait mobility (e.g., gait speed, stepping accuracy, narrow walk time, velocity, stride time, step length, step time variability under dual tasks [DT] condition) were reported in 10 studies,16,24,27,31,35,39,41–44 with the length of intervention ranging from 9 to 24 hours (M = 15.4). The timed up and go (TUG) assessment was most frequently used (N = 2). The GAITRite was the most widely used device for analysis of gait parameters. We found that videogame-based interventions were superior to physical training programs regarding gait velocity and single support time of fast walking under DT conditions, 16 stride time under DT conditions, 42 and DT costs of step time variability at fast walking. 35
Mental health benefits
Mental health benefits were reported in 14 out of 18 papers. Results of mental health benefits of playing videogames are summarized next.
Balance confidence/fear of falling
Eight studies25–27,29,31,39,42,43 (interventions length: 5–20 hours; M = 9.83) have reported increased confidence in body balance or decreased fear of falling. The activities-specific balance confidence 45 scale was the most used questionnaire for measuring balance confidence (N = 2), and the Modified Falls Efficacy Scale 46 was the most used questionnaire for measuring the fear of falling (N = 2). Duque et al. 26 and de Bruin et al. 42 have found that videogame-based interventions were superior to physical training programs regarding reducing the fear of falling.
Executive functions
In total, there were six papers that focused on executive functions.
Inhibition
Four studies33,41,47,48 (intervention length: 12–25 hours; M = 16.25) have reported improvements in inhibition. The Stroop Word and Color Interference Test 49 was the most used task for inhibition (N = 2).
Set-shifting
The outcome of set-shifting was included in four studies33,36,41,50 (interventions length: 10–48 hours; M = 9.83). The Trail Making Test 51 (TMT) part B (TMT-B) was the most used task for set-shifting (N = 3). Eggenberger et al. 50 found that their videogame-based intervention led to higher improvements in set-shifting than a physical training program.
Working memory
The outcome of working memory was concluded in two studies41,50 (intervention length: 12–48 hours; M = 30). They used a test battery for attentional performance 52 (TAP) and executive control task for assessing working memory, respectively. Eggenberger et al. 50 found that their videogame-based intervention achieved a better working memory improvement than other types of memory training programs.
Divided attention
Two studies41,48 (intervention length: 12–16 hours; M = 14) have reported improvements in divided attention. They used TUG and TAP to assess divided attention, respectively.
Reaction time
Improvements in reaction time was supported by two studies47,48 (intervention length: 16–25 hours; M = 20.5). They used choice stepping reaction time test and the Sternberg test for measuring reaction time, respectively.
Processing speed
Improvements in processing speed were concluded by two studies36,50 (intervention length: 10–48 hours; M = 29). The TMT part A (TMT-A) was the most used task for accessing processing speed (N = 2).
Other measured outcomes
General cognition
Eggenberger et al. 33 have found that general cognition, which was evaluated by the Montreal cognitive assessment, improved after 12 hours of a videogame-based intervention.
Emotional well-being
Goldstein et al. 47 have reported that emotional well-being, which was assessed by a Dutch version of the well-being questionnaire, 47 improved after 25 hours of a videogame-based intervention.
SF-36 mental health questionnaire
The overall score of the 36-item short-form health survey (SF-36) 53 mental health questionnaire, which measures vitality, social functioning, emotional role, and mental health, significantly increased after 12 hours of intervention. 43
Other memory-related mental health outcomes
Eggenberger et al. 50 have found that 48 hours of a videogame-based intervention could improve long-term visual memory (paired-associates learning task), 54 long-term verbal memory (Wechsler Memory Scale—Revised), 55 and short-term verbal memory (Wechsler Memory Scale—Revised).
Synthesis of results
Experiment details
Fourteen studies applied a randomized controlled trial (RCT). The following experiment designs were also used: two-group design without randomly assigning participants (N = 3), one-group design (N = 3), crossover design (N = 2), and quasi-experimental single-group design (N = 1). Nine of the reviewed articles applied a single-blinded design, where all of them blinded their participants to the outcome. All 23 articles used validated and reliable instruments for measuring health outcomes. All articles involved pre-/post-test design.
Intervention details
The duration of interventions ranged from 3 to 24 weeks (M = 9.35 weeks, SD = 5.73). A month was considered 4 weeks long if the paper reported duration to be month-based. The average number of sessions of each article was 22.36 (SD = 12.49), which ranged from 9 to 48 sessions. The average duration of each study was 13.58 hours (SD = 10.31), ranging from 3 to 25 hours. Ten studies were performed at the participants' residence place, at either a facility specializing in elderly care or their actual home. Seven were conducted in a place that required participants to travel, with six in a clinic and hospital setting and one in a research lab setting.
Sample details
All studies included participants of both genders, where the average percentage of the females in each study is 64.69% (SD = 18.86%). The number of participants in each study ranged from 18 to 90 participants (M = 44.30, SD = 23.67). The mean age of participants in each study in the selected research literature is 79.27 years old (SD = 4.77). The average dropout rate is 11.73% (SD = 12.06%).
Game and platform details
Exergames (N = 22) were the most frequently used type of games that mainly investigated physical aspects (i.e., balance, strength, mobility) with a potential to improve balance confidence/fear of falling. Exergames could also help to improve other mental health aspects when they contained cognitive tasks/elements. Besides exergames, casual games (N = 1) were also used in the interventions. Eight articles used a dance pad/platform in their intervention. The Nintendo Wii Fit™ balance board (N = 4) and Kinect (N = 4) were the second most used types of equipment. Among these, only Kinect is capable of full-body motion tracking.
Meta-analysis
Previous research 23 has suggested that “in practice, 5 or more studies are needed to reasonably consistently achieve powers from random-effects meta-analyses that are greater than the studies that contribute to them. Not only is statistical inference under the random-effects model challenging when there are very few studies but also less worthwhile in such cases.” Therefore, it was not feasible to perform a meta-analysis on balance (FRT, N = 3), physical fitness (N = 3), strength (N = 2), gait parameters (N = 2), confidence of balance (N = 2), and fear of falling (N = 2). The low number of papers examining a specific outcome (N = 1) made a meta-analysis impossible for (1) general cognition, (2) emotional well-being, (3) SF-36 mental health questionnaire, and (4) other memory-related mental health outcomes.
In addition, different metrics used for the same outcome have likewise led to a low number of papers (N = 1) for outcomes such as working memory, divided attention, reaction time, and processing speed. As such, it was not feasible to conduct a meta-analysis.
Discussion
Summary of the evidence
This article has summarized and analyzed the findings of 23 research articles, with 9 rated as “high quality” and 14 rated as “moderate quality” based on the Quality Assessment Tool for Quantitative Studies. 20 Because they did not use single- or double-blinded experiment design, 14 articles were rated as “moderate quality.” We recommend blinding the participants instead of investigators—it is more difficult to blind the investigators, as they often supervise and conduct the training and assessments.16,33,44,50
Regarding physical health outcomes, our review has found that playing videogames could result in improvements in users' balance24–32 (N = 9), functional mobility24,27,31,39,44 (N = 5), gait parameters16,35,41–43 (N = 5), physical fitness33–36 (N = 4), and body strength24,29,39,40 (N = 4). Among these studies, we have found that videogame-based interventions could lead to significantly greater improvements than traditional physical training programs when it comes to gait velocity and single support time of fast walking under DT conditions, 16 stride time under DT conditions, 42 and DT costs of step time variability at fast walking. 35
Regarding mental health outcomes, our review has found that game-based interventions have the potential to improve balance confidence (or decrease fear of falling)25–27,29,31,39,42,43 (N = 8), executive functions [inhibition33,41,47,48 (N = 4), set-shifting33,36,41,50 (N = 4), working memory41,50 (N = 2), divided attention41,48 (N = 2), reaction time47,48 (N = 2), and processing speed36,50 (N = 2)]. Other outcomes are general cognition, 33 emotional well-being, 47 overall SF-36 mental health, 53 long-term visual memory, long-term verbal memory, and short-term verbal memory. 50 In addition, we found that videogame-based interventions could lead to significantly greater improvements in balance confidence26,42 and set-shifting 50 than a physical training program. The former also outperformed a memory training program in improving the working memory of elderly users. 50
This review has not found enough evidence to conclude that there are effects of a videogame-based intervention on social inclusion or interaction for the aging population, because no studies met the inclusion criteria. There are two possible reasons: (1) The setup of these type of studies is not as easy as that of those targeting physical and mental outcomes, because measuring social inclusion would require some type of long-term investigation with at least two older adults playing a game together; and (2) there might have been a lack of using keywords that are related to social well-being in the literature.
In addition to the findings cited, our review has pointed out two additional issues. First, we observed that existing studies do not report follow-up studies/results. Several studies56,57 have shown that the health benefits that were obtained from videogame interventions, just like other training programs, would vanish if there was no further follow-up training after a certain period. Conducting follow-up experiments and reporting their results could benefit the field and help design improved interventions and gaming experiences.
Second, Ben-Sadoun et al. 36 have reported that older adults with cognitive impairment had lower improvements in physical fitness and cognitive function tests compared with healthy older adults. Therefore, it may be important to pre-screen participants before assigning them to an experimental group. It is also useful for researchers to conduct and publish this type of comparison studies to help developers and designers to better understand the similarities and differences when designing and testing games for unhealthy and healthy older adults.
Regarding the gaming platforms and devices, we found an increasing trend in using the Kinect (N = 4) to assist and promote health benefits compared with previous reviews. 18 There are several advantages of using the Kinect, as opposed to other similar devices, such as the Nintendo Wii. For example, one Kinect can track multiple players, 58 and can also be used to check for possible falls, 59 and in seated-based exergames (e.g., wheelchair-based), 60 which could allow users to perform exercises at home without the need to be standing and, in the case of weaker elderly users, without any external assistance.
Guidelines for future research
In this section, we provide some key guidelines for researchers in this field, which could help make the interventions more effective.
Enriching the study quality
The quality of studies can be improved by (1) applying an RCT with an active control group, reporting the randomization procedures; (2) blinding participants to the expected study outcome; (3) using validated and reliable health measurements as non-validated/customized measurements could weaken the study; (4) using a larger sample size (a power analysis should be performed before recruiting participants and if possible, we suggest to have an additional 11% of the desired sample size because this is the average dropout rate based on our review); and (5) reporting age, dropout rates, and gender details of the participants whenever possible.
Getting the desired outcome(s)
(1) Exergames should be the preferred option, followed by casual games. The data seem to support the use of an exergame consisting of cognitive elements/tasks that not only improve physical well-being but can also enhance physiological-related health. (2) The included protocols on average consist of two to three 30–40 minute sessions per week for ∼9 weeks. Data obtained from our investigation showed that the intervention should last at least 22 sessions and 13.5 hours of training. This finding may provide recommendations with respect to duration of a single session, frequency of sessions, and period of the intervention. However, the total duration of training for each intervention may differ from one to another depending on the target health outcomes (e.g., 6.8 hours for balance improvement whereas 10 hours for improving balance confidence).
Other guidelines
The following guidelines are useful to follow: (1) Considering the potential difficulties for older adults to travel from their place to an external experimental venue, the data seem to indicate that it is more ideal/efficient for researchers to visit the participants in their natural place of residence to conduct any experiments; (2) screen participants to gather their health situation before randomly assigning them to the intervention groups; and (3) perform follow-up studies several weeks/months after the intervention.
Limitations
This review has two limitations. First, there could have been some publication and language bias, given that we considered only interventions described in published studies and restricted our search to English language publications available in the main research databases. Second, there is a potential that our selected keywords and inclusion criteria may have limited the number of studies, though we attempted to be as encompassing as possible.
Conclusion
This review demonstrates that using videogame-based interventions can help promote HRQOL, physical and motor skills (i.e., balance, mobility, strength, physical fitness, and walking performance/gait parameters), and mental health (i.e., balance confidence, executive functions, reaction time, processing speed, and other physiological aspects). Among the 23 articles included in our review, 20 of them had reported at least one physical outcome, whereas 14 of them had described at least one mental health outcome.
We have also found that videogame-based interventions could outperform traditional training programs regarding walking performance/gait parameter, balance confidence/fear of falling, and executive functions (i.e., set-shifting, working memory). However, our review could not find any articles that reported direct social health outcomes. Given the importance of social aspects in the elderly's health, social outcomes should be an important part of future research in videogame-based interventions. Overall, there have been a lot of articles published since the previous review conducted in this field in 2011 and there has been considerable development in using videogames and gameplay activities to promote the physical and mental health conditions of elderly adults.
Footnotes
Acknowledgment
The authors would like to thank the reviewers for their valuable comments and helpful suggestions.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported in part by Xi'an Jiaotong-Liverpool University Key Program Special Fund (No. KSF-A-03), and XJTLU Research Development Fund.