
Abstract
Objective:
To investigate the effect of motion-controlled videogames on pain, functionality, cardiopulmonary capacity, and quality of life in women with fibromyalgia.
Materials and Methods:
Forty women with fibromyalgia were randomized into virtual reality group (VRG) and conventional training group (CTG). The CTG performed aerobic exercise (cycling, 3 days per week, 20 minutes per day) and conventional exercises (muscle strengthening, balance, and flexibility, 3 days per week, 15 minutes per day) for 4 weeks. The VRG performed virtual reality exercise (volleyball, Microsoft Xbox Kinect®, 3 days per week, 15 minutes per day) together with cycling exercise for 4 weeks. After the exercise program, both groups received the same home exercise program for 4 weeks. All patients were evaluated at baseline, fourth, and eighth weeks. Primary outcome measure was Fibromyalgia Impact Questionnaire. Visual Analogue Scale (VAS), Hospital Anxiety and Depression Scale, Fatigue Severity Scale (FSS), Symptom Severity Scale, EuroQol-Five Dimensions İndex Scale/Visual Analogue Scale (EQ-5D-index/VAS) and Six Minute Walk Test (6MWT) were used as secondary outcome measures.
Results:
Thirty-four patients (17 VRG, 17 CTG) were evaluated at the eighth week. After 4 weeks, all outcome measures improved significantly in both groups (P < 0.05). However, there was no statistically significant difference in all outcome measures between fourth and eighth weeks. Group and time interactions for 6MWT (P = 0.043), FSS (P = 0.026), EQ-5D-İndex Scale (P = 0.014), and EQ-5D-VAS (P = 0.049) were significant only for the VRG. In addition, median individual's satisfaction was significantly higher in the VRG (P < 0.001).
Conclusion:
Virtual reality exercises along with aerobic exercise increase cardiopulmonary capacity and quality of life in fibromyalgia syndrome. In addition, they increase patient satisfaction and may improve patient compliance to exercise.
Introduction
Fibromyalgia Syndrome (FMS) is a clinical disease that includes chronic widespread pain, fatigue, sleep disturbance, mood alteration, and cognitive dysfunction. 1 The prevalence of FMS is in 0.2%–6.6% of the population. 2 FMS is more common in women and more painful.3,4
However, pathophysiology of FMS is not fully clear, one of the most prominent mechanisms is central sensitization. 5 Central sensitization is explained by disruption of the modulation of pain in the central nervous system and imbalance of inhibitory-excitatory neurotransmitter.6,7 Thus, patients with fibromyalgia compared with healthy people demonstrated an increased and prolonged pain.5–7 It is also reported that neuroendocrine and immunological abnormalities have a role in sleep disturbance, mood alteration, and cognitive dysfunction besides chronic diffuse pain. 7
The treatment of FMS is difficult due to clinical heterogeneity. Numerous treatment guidelines have been published for this purpose. These guidelines contain a wide range of evidence-based pharmacological and nonpharmacological treatment approaches. In all guidelines, the most important component of treatment is regular exercises.8–12 Among the exercise types, especially aerobic exercise is the foreground exercise.13,14 In FMS, there are many studies, reviews, or meta-analysis that show positive effect of aerobic exercise on physical function.13–16 Studies in aerobic exercises include cycling, treadmills, and swimming.14,15,17
In FMS, patients generally have compliance and motivation problems in the maintenance of exercises.16,17 In recent years, exercises, with fun and game components, have been prescribed to increase patient compliance.18–24 Motion-controlled videogames targeting virtual reality are examples of these exercises. When we searched the studies about virtual reality exercises that are used in rehabilitation of patients with fibromyalgia, it has been shown that virtual reality exercises reduce fear of falling and static balance problems, 21 improve autonomic balance, 25 reduce pain,26–29 increase healthy-related quality of life27–29 and exercise capacity,26,29 promote cardiovascular fitness,26,30 and decrease the impact of FMS and fatigue. 26 It was also stated that these exercises motivated patients, increased patient compliance and patient satisfaction, and promoted psychological process (general mood state, positive emotions, motivation, and self-efficacy) in the rehabilitation. 23
In light of all these studies, to measure the effect of virtual reality exercises with a different methodology, we designed two groups: (1) virtual reality exercises combined with aerobic exercise and (2) conventional exercises combined with aerobic exercise. The aim of this study is to investigate the effect of motion-controlled videogames on pain, functionality, cardiopulmonary capacity, and quality of life with randomized and controlled methods in women with fibromyalgia. Our hypothesis is that virtual reality exercises improve the health status and the quality of life by reducing pain and increasing cardiopulmonary capacity more than conventional exercises in women with fibromyalgia.
Methods
Participants
Forty female subjects from the outpatient clinic of Gazi University Department of Physical Medicine and Rehabilitation participated in this single-blind randomized controlled trial. The following inclusion criteria were applied: diagnosed with FMS using the American College of Rheumatology 2010 classification criteria, 1 age between 18 and 65 years, at least 8 years of formal education and taking the same medication for FMS for at least 3 months. Exclusion criteria included secondary FMS, intellectual deficits, visual deficits, suffering from inflammatory rheumatic disease, and having any orthopedic surgery at least 6 months. The recruitment of the patients with fibromyalgia was done prospectively by a physical medicine and rehabilitation specialist. Each subject gave written informed consent before participating in the study. Ethical approval was obtained from Institutional Review Board at Gazi University that approved the study protocol and informed consent (77082166-604.01.02).
Measures
Demographic characteristics of participants such as age, height, weight, body mass index (BMI), education status, and symptom duration were recorded before treatment. Pain intensity, general health status, symptom severity for fatigue, sleep quality, cognitive symptoms, somatic symptoms and health-related quality of life, mood, and functional capacity were assessed and documented at baseline, fourth, and eighth weeks. Main outcome measure of study was Fibromyalgia Impact Questionnaire (FIQ). Secondary outcome measures were Visual Analogue Scale (VAS), Symptom Severity Scale (SSS), Fatigue Severity Scale (FSS), Six Minute Walk Test (6MWT), Hospital Anxiety and Depression Scale (HADS), and The Euro Quality of Life Five Dimension (EQ-5D).
The FIQ was used to assess function and health-related quality of life of patients. This self-administered questionnaire evaluates pain, tenderness, fatigue, stiffness, multidimensional function, and sleep. Final score ranges between 0 and 80. High scores indicate a major impact of FMS on functioning. The Turkish version of the FIQ was shown to be valid and reliable. 31
Pain intensities of the patients over the past week were assessed by using VAS. SSS was used to evaluate symptom severity for fatigue, sleep quality, cognitive symptoms, and somatic symptoms. The severity of these symptoms over the past week was rated on a scale from 0 to 3. 0 = no problem, 1 = slight or mild problems, 2 = moderate considerable problems, and 3 = severe pervasive continuous life-disturbing problems. The final SSS is the sum of the severity of these symptoms and ranges between 0 and 12. 1 Turkish version of the SSS for FMS was found as valid and reliable. 32
The FSS was used to evaluate symptom severity for fatigue. The scale contains nine items that measure the severity of fatigue symptoms of the subjects during the past week. Each item is scored from 1 to 7. “1” indicates strong disagreement with the statement, whereas “7” indicates strong agreement. Total score is calculated by deriving an arithmetic mean. A score of 4 or higher generally indicates severe fatigue. 33 Turkish version of FSS for FMS was found as valid and reliable. 34
Functional capacity of the patients was assessed by using the 6MWT. The 6MWT was performed in a plane corridor of 30 m in length, following the recommendations of the American Thoracic Society. 35
The HADS was used to assess the mood of patients. The HADS consists of 14 items, 7 evaluating cognitive and emotional aspects of anxiety (HADS-A) and 7 representing the cognitive and emotional aspects of depression (HADS-D). Each question is scored on a 4-point Likert scale, ranging from 0 to 3, where a higher score represents more severe depression or anxiety. 36 Turkish version of HADS was found as valid and reliable. 37
The EQ-5D is a generic instrument used for measuring health-related quality of life. 38 It comprises the EQ-5D index scale and the EQ-5D VAS. The EQ-5D index scale currently comprises a questionnaire with five dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression). Each dimension of the EQ-5D is divided into three degrees of severity as “no problem,” “some problems,” or “major problems” A single index score can be produced using information from these five dimensions. The EQ-5D index score ranges from −0.59 to 1 and includes a worse than death measure (negative score), outside the range of 0 (dead) to 1 (perfect health). The EQ-5D VAS is a 20-cm VAS where the respondent is asked to mark his or her own current state of health on a thermometer-like line calibrated from 0 to 100.39,40 Turkish version of EQ-5D was found as valid and reliable. 41
At the end of the exercises, patient satisfaction is evaluated by a 5-point Likert scale, ranging from 1 to 5 (1, not at all satisfied; 2, slightly satisfied; 3, moderately satisfied; 4, very satisfied; 5, completely satisfied) at both groups.
Randomization
Participants were randomly allocated into a virtual reality group (VRG) or conventional training group (CTG) using a computer-generated random number sequence constructed by a physiatrist. The same physiatrist who was not involved in the assessment of study outcome measures performed the randomization. The other physiatrist evaluated outcome measures of the study who was blinded to the treatment allocation. The exercise program was administered by a physiotherapist, who was blinded to outcome measures. All outcome assessments were repeated by the same blinded physiatrist at fourth and eighth weeks.
Treatment
All patients were informed about FMS such as following “It is a functional brain disorder in which symptoms and pain are treated differently, and the symptoms are not caused by an organic disease such as a disorder of the muscles or joints,” “The disease and symptoms are real,” “The complete disappearance of symptoms rarely occurs,” “The symptoms should not lead to disability and shorten of life,” “Most patients have been adapting to their symptoms over time,” and “Patients can correct symptoms and health-related quality of life with their own coping methods.”
Both groups performed an aerobic exercise program that comprised cycling activity for 20 minutes 3 days per week. Aerobic exercise intensity was adjusted to generate heart rates equivalent to 60%–70% of age-adjusted maximum heart rates (220—age in years). Heart rate monitoring was performed by using a pulse oximeter (Nonin Medical, Inc., MN). At the beginning and end of each session, mild stretches were performed for 5 minutes.
The CTG performed muscle strengthening, balance, and flexibility exercises for 15 minutes 3 days per week in addition to aerobic exercise. Strengthening exercises were performed in a single series containing 10 repetitions at an intensity of 40% of the estimated 1 repetitive maximum, including upper and lower extremity large muscle groups in standing and sitting positions, as a standard exercise protocol with moderate intensity.
The VRG performed virtual reality exercise in addition to aerobic exercise. Microsoft Xbox Kinect® was used for virtual reality exercises. Beach Volleyball, which was included in the “Kinect Sports” videogame, was chosen since it was thought to be more familiar and easy to perform. Beach Volleyball is a game that could be started by a user or computer. Users serve by making a tossing motion with one hand and a swinging motion with the other. Once the ball is in action, you get to bump, set, and spike it back and forth. Beach Volleyball is a real ceiling scratcher, getting users to move (stepping all sides, jumping, hitting, or blocking ball, etc.) his/her spine and appendicular skeletal system. Also the cardiopulmonary system is highly activated during the sport.42,43
The virtual reality application, which consists of a computer (LCD screen monitor, keyboard, mouse, and speaker) and an infrared camera (Xbox Kinect sensor), was a semi-immersive system. During virtual reality exercises, patients were placed 2 m away from an LCD screen (144 cm*81 cm and 1024*768 pixels) for detecting body movements by the infrared camera. They performed virtual reality exercise for 15 minutes 3 days per week under supervision after cycling activity.
After the 4-week supervised exercise program, both groups received the same home exercise program for 4 weeks. Home exercise program included moderate-intensity aerobic physical activity for 30 minutes on 5 days each week, muscle strengthening and balance exercises 2 days a week, and flexibility exercises with stationary stretches every day for 4 weeks.
Statistical analysis
Before enrolling participants, we calculated 20 patients per group, to find 14% minimal clinical difference in FIQ with 80% power and 0.05 error rate (Type 1 error). 44 Intention-to-treat (ITT) analysis was performed for the patients who were initially randomized into one of the groups and completed a 4-week exercise part but who lost in the 4-week follow-up part by using the last observation carried forward method. All primary efficacy analyses were conducted on the ITT population by using SPSS version 25 (IBM, Armonk, NY). The variables were investigated using visual (histograms and probability plots) and analytical methods (Kolmogorov–Smirnov/Shapiro Wilk) to determine whether or not they are normally distributed. Descriptive analyses were presented using means and standard deviations for normally distributed variables and frequencies for categorical data.
Independent sample t-test and chi-square tests were used to test for difference between the VRG and the CTG at the baseline. Repeated measures analysis of variance (ANOVA) test was used in evaluation of intragroup efficiency of treatment between baseline, fourth week, and eighth week. Group and time interaction was evaluated by two-way ANOVA for all outcomes. Greenhouse–Geisser correction was used when the sphericity assumption was violated. Paired sample t-test was used to compare the measurements at three time points (baseline, fourth week, and eighth week) for all outcome variables. The percentage of change between pre- to post-tests was calculated using the following formula:
Percentage change pre- to post-tests = [(post-test score−pretest score)/pretest score] * 100
An overall 5% type-1 error level was used to interstatistical significance. Line graphs were used to clarify group and time interaction of outcome measures.
Results
In total, 75 women with fibromyalgia were screened. Forty subjects were assessed for baseline because 13 did not meet inclusion criteria, 11 did not want to participate in the study, and 11 had other reasons (9 had exclusion criteria, 1 moved to another city, and 1 operated for orthopedic foot problem). Finally, 40 patients were randomized into the VRG (20) and the CTG (20), data from 40 patients were analyzed by ITT. All patients completed a 4-week exercise program. No adverse effect was noted about exercises. Three patients from both groups were lost to follow-up. Seventeen participants from each group completed the study protocol (Fig. 1).
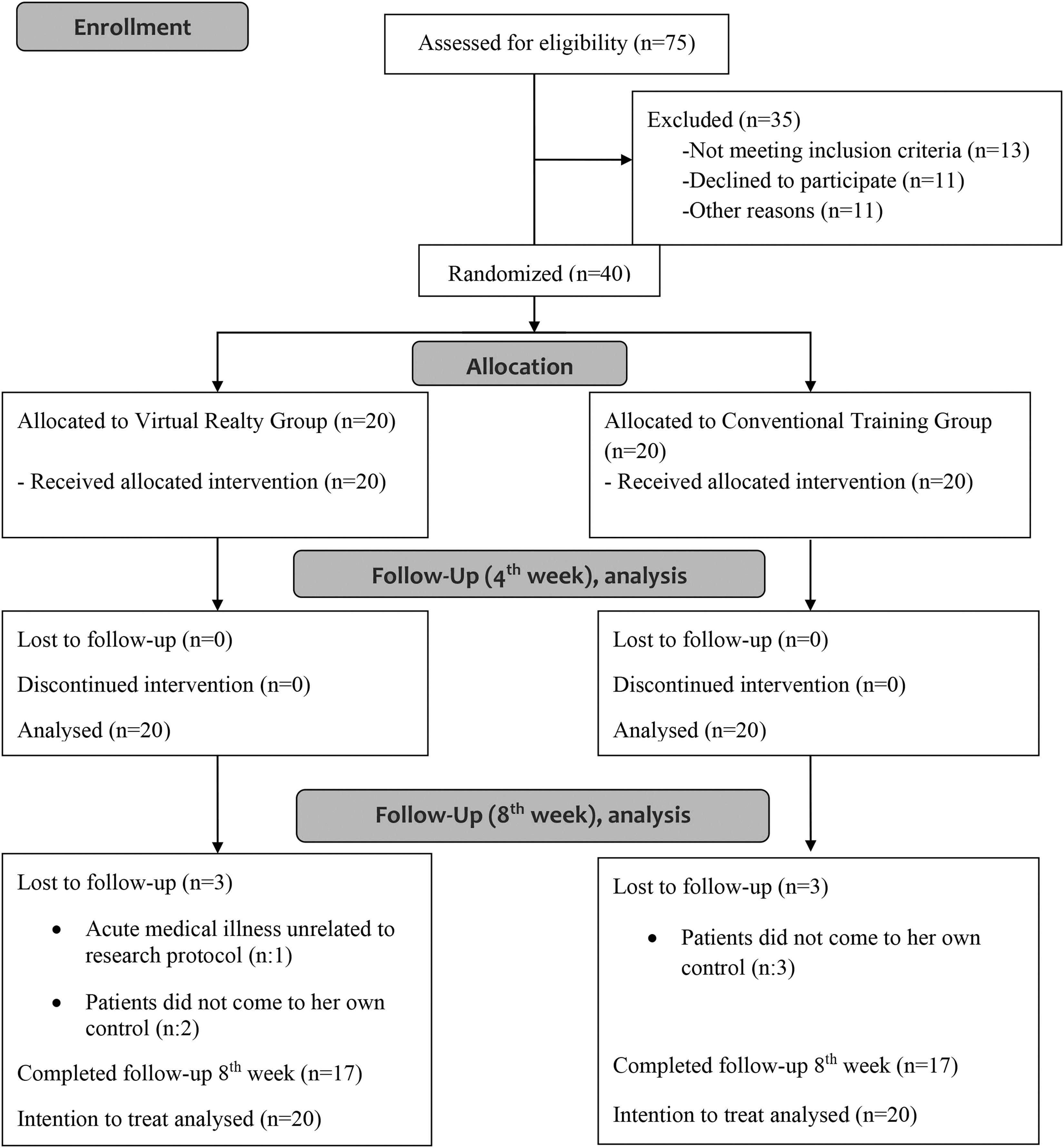
Study flow diagram.
Comparisons of baseline characteristics
Demographics and clinical characteristics are given in Table 1. Groups were not significantly different in terms of age, height, weight, BMI, and education level. Regarding clinical characteristics, mean time of diagnosis was similar in two groups (16.53 ± 4.1 months in the CTG, 18.2 ± 5.3 months in the VRG).
Baseline Characteristics of Patients
VRG, data calculated on ITT population.
cm, centimeter; kg, kilogram; m2, square meter.
BMI, body mass index; CTG, conventional training group; ITT, intention-to-treat; SD, standard derivation; VRG, virtual reality group.
Baseline outcome measures are given in Table 2. Comparison of all baseline outcome measures showed no significant difference between the groups (P > 0.05).
Baseline Outcome Measures of Patients
VRG, data calculated on ITT population.
6MWT, Six Minute Walk Test; EQ-5D-İndex/VAS, EuroQol-İndex Scale/Visual Analogue Scale; FIQ, Fibromyalgia Impact Questionnaire; FSS, Fatigue Severity Scale; HAD-A/HAD-D, Hospital Anxiety and Depression Scale; SD, standard derivation; SSS, Symptom Severity Scale; VAS, Visual Analogue Scale.
Virtual reality exercise versus conventional aerobic exercise
Table 3 gives the outcome measures for the VRG and the CTG at baseline (T1), fourth week (T2; at the end of exercise program), and eighth week (T3; 4-week follow-up). At the end of exercise program, all scores of outcome measures improved significantly in both groups [T1 vs. T2 (*P < 0.001)]. At the end of 4-week follow-up period, all scores of outcomes were higher than the baseline scores [T1 vs.T3 (*P < 0.001)]. However, we did not find any difference in outcome scores between fourth week and eighth week [T2 vs. T3 (*P < 0.001)].
Mean Outcome Measures of Conventional Training and Virtual Realty Groups at Baseline, Fourh Week, and Eighth Week
T, time; G, group; T1, baseline; T2, 4th week; T3, 8th week.
P < 0.001.
CTG, data calculated on ITT population.
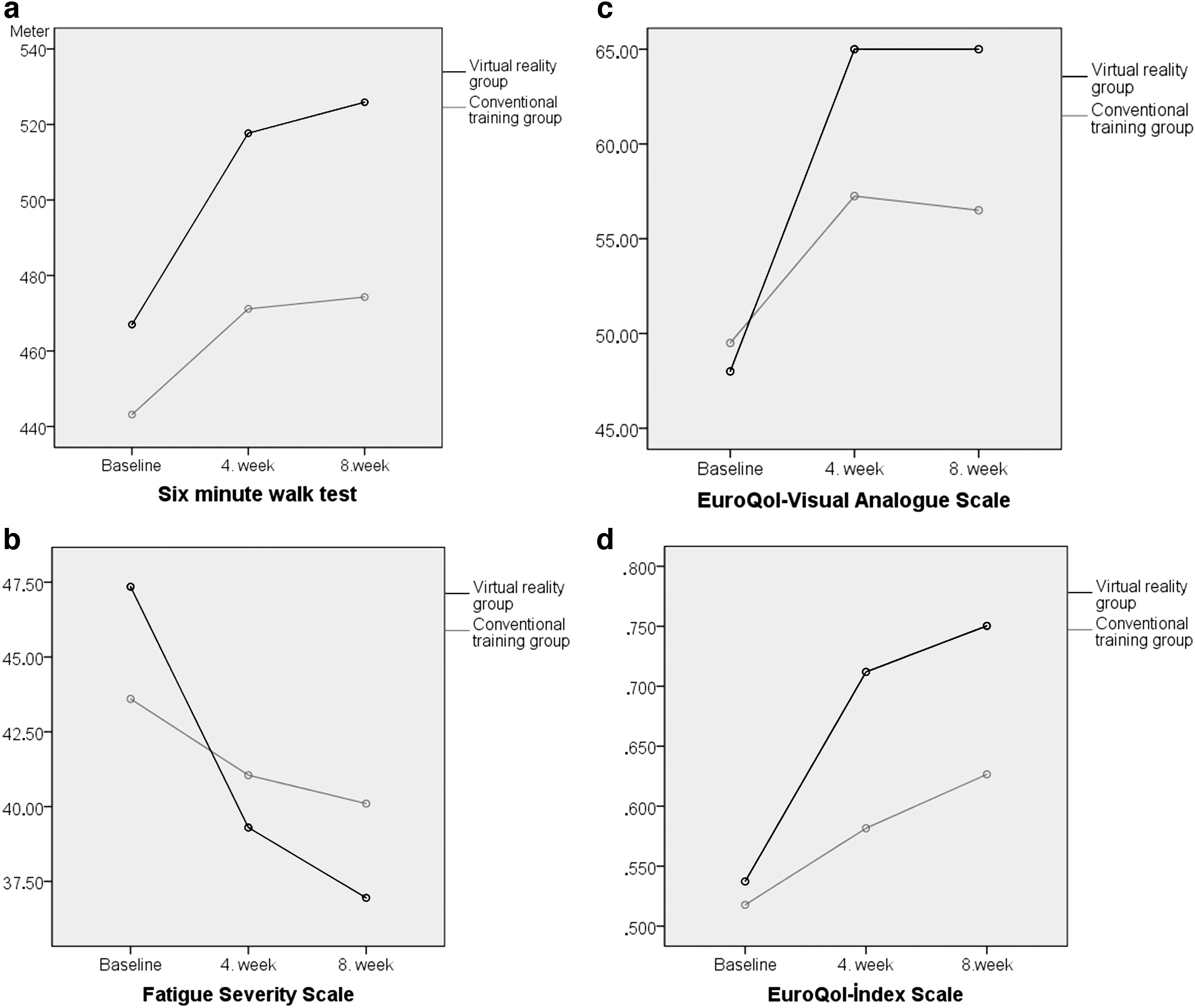
In the repeated measures ANOVA all outcome measures, independently of intergroup effect, showed statistical significant difference. In the two-way ANOVA, a statistically significant difference was determined in the treatment group x time (T*G) interaction in favour of VRG in 6MWT, [F(1.21, 46.33) = 4.04, P = 0.043], FSS [F(1.61, 61.24) = 4.21, P = 0.026], EQ-5D-Index Scale [F(2, 76) = 4.55, P = 0.014], and EQ-5D-VAS Scale [F(1.4, 53.55) = 3.59, P = 0.049] (Table 3 and Fig. 2a–d). No statistically significant difference was determined in the treatment group x time interaction in VAS, HAD-A, HAD-D, SSS, FIQ, respectively [F(1.74, 66.3) = 3.03 P = 0.06], [F(1.22, 46.8) = 0.08 P = 0.82] [F(1.78, 44.7) = 1.87 P = 0.17] [F(1.43, 54.5) = 3.17 P = 0.65] [F(1.26, 48.13) = 2.28 P = 0.13] (Table 3).
In addition, median satisfaction score was significantly higher in the VRG (CTG: 2 ± 1, VRG: 3 ± 1; P < 0.001).
Discussion
In this study, we aimed to investigate the effect of motion-controlled videogames on pain, functionality, cardiopulmonary capacity, and quality of life of women with fibromyalgia. All outcome measures improved significantly in both groups. Nevertheless, we did not find any significant differences in outcomes between fourth and eighth weeks in the two groups. When the treatment group × time interaction was evaluated, the improvement in 6MWT, FSS, EQ-5D-İndex, and EQ-5D-VAS Scale was determined to be significantly greater in the VRG. In other words, cardiovascular performance and quality of life were significantly increased and fatigue was reduced by virtual reality exercises added to aerobic training in this study. Besides, the satisfaction score was significantly higher in the VRG.
This study suggests that virtual reality exercises added to aerobic training are useful for treatment of fatigue (evaluated by using FSS) in the women with fibromyalgia. Fatigue is one of the prominent symptoms in FMS that prevents work and social life. Carvalho MS et al. showed that the exergames have the potential to reduce fatigue of lower limbs. 26 Studies also showed the improvement of symptoms, based on the FIQ, including the fatigue domain too.26,27 Our study also showed that reduction of impact of fibromyalgia is the same in both groups, but differences of changes in FIQ are not significant. This study has shown that another benefit of virtual reality exercises added to aerobic training is improving health-related quality of life (EQ-5D-index scale). Similarly, two randomized controlled trials showed a significant improvement in the quality of life with exergames in FMS.27,28
We found that improvement in physical performance was significantly higher in the VRG than in the CTG. In the literature, there are studies reporting improvement in cardiovascular fitness,21,30 adaptation, 25 and mobility. 24 It is necessary to emphasize the reasons why physical performance increases significantly with virtual reality training. In one study, although physical activity levels of FMS patients were the same as those of healthy subjects, decreased physical performance in the 6MWT was explained by psychosocial adaptation to life conditions and deterioration in pain perception. 45
In our study, virtual reality exercise added to aerobic training might decrease the perception of pain and increase psychosocial compliance; therefore, it improved physical performance and quality of life in the VRG. At the same time, the patients in the VRG were performing aerobic exercise with their upper extremities in addition to lower extremities during the Beach Volleyball game, which is used as virtual reality exercise. Also, aerobic activity duration in the VRG (15 minutes per day virtual reality exercise plus 20 minutes per day cycling) was longer than the CTG (only 20 minutes per day cycling). Increase in cardiovascular performance that is more prominent in the VRG might also be related to these conditions.
In addition, perceiving and directing to the coming target in the space, and performing the task (hitting the approaching ball at different speeds and positions) during the volleyball game can be designated as motor coordination exercise. With this approach, virtual reality exercises may be a method used in the treatment of spatial learning disorder due to hippocampal system involvement in FMS, as stated by Cánovas et al. 46 Another study showed that the patients with fibromyalgia showed significant relationships between peak oxygen consumption and the left and right regions of the hippocampus and the left and right regions of the amygdala after 24 weeks of exergame program. 47 Also a study has just shown a deficit in predicted sensory feedback (sensory-motor conflict) in FMS. 48
In this study, after 4 weeks of exercise, patient satisfaction was significantly higher in the VRG than in the CTG. We can speculate that higher satisfaction levels during virtual reality exercise added to aerobic training might increase the motivation of the patients. There are studies in the literature that patients are more motivated and enjoyed during virtual reality exercise.19,23 The reason for this might be that game-based exercises stimulate many sensory systems (visual, auditory, and somatosensory) to give the person a more active and concentrated exercise.
In addition, patients who performed virtual reality exercises combined with aerobic training had improved mood/anxiety (HAD-A), disease severity (SSS), and functionality (FIQ) measure, but these improvements were not significantly different from the CTG. This result that supports the literature26–30 shows that combining virtual reality exercise and aerobic training is as effective as combining conventional exercise and aerobic training. Also these favorable results continued for 4 weeks after the end of exercise treatment (eighth week control) in both groups.
In a clinical trial published by Villafaina et al., exergame protocol took 24 weeks, and then patients were evaluated at the end of protocol. 28 In another study, patients received an 8-week intervention based on exergames, then they were evaluated before and after the intervention. 21 Recently, in another study, patients with fibromyalgia performed exergame treatments for a period of 7 weeks with three 1-hour sessions weekly and were re-evaluated after the 10th and the 20th sessions. 26 To sum up, these clinical studies20,21,23,24,26–28 that performed virtual reality exercises at different durations (from 4 to 24 weeks), improvement of these domains continued in the short–medium term. In the literature, since its long-term effects are still uncertain, further studies would contribute.
There are several limitations in our study. First limitation is that the participants consisted only of female patients. Second limitation is that these results have emerged with Beach Volleyball, which was chosen as a virtual reality exercise. So results cannot be generalized to all of the many virtual reality-based videogames for exercise. Another limitation of the study is that the aerobic activity durations of both groups were different. However, while evaluating this limitation, it should be kept in mind that moderate level of strengthening exercises also contributes to aerobic performance. 49 In addition, another point is the fact that virtual reality exercises are not only aerobic activities, but also enjoyable motor coordination exercises that provide multisensory inputs.23,46,48 The last limitation of study is that the follow-up period was 8 weeks. Therefore, studies that have included male patients, longer follow-up and different types of videogames are needed to attribute the results to the general population.
Conclusion
Virtual reality exercises along with aerobic exercise increase cardiopulmonary capacity and quality of life in FMS. In addition, they increase patient satisfaction and may improve patient compliance to exercise. Future studies should aim to develop targeted and analytical rehabilitation programs by applying specific virtual reality exercises according to the specific pathology of FMS.
Footnotes
Acknowledgments
The authors wish to thank the patients with fibromyalgia from the Department of Physical Medicine and Rehabilitation at Gazi University Hospital who participated in this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
There is no funding for this study.