
Abstract
Objective:
Serious videogames and virtual reality (VR) have gained increasing interest for treating attention deficit hyperactivity disorder (ADHD). “The Secret Trail of Moon” (TSTM) study is a clinical trial devoted to testing the efficacy of TSTM, a VR serious videogame developed to train in five major cognitive skills usually compromised in patients with ADHD. This study is a three-arm nonequality trial comparing TSTM to online chess training and a control group (CG). This study aims to demonstrate that augmentation with either TSTM or online chess is efficacious in clinically drug-stable patients with ADHD.
Materials and Methods:
This study is prospective, unicentric, and randomized with a CG. One hundred five patients with ADHD, ages 12–22 years old, and pharmacologically stable were enrolled. Patients were randomized into three groups: TSTM group, online chess group (therapeutic chess [TC]), and CG. Objective and subjective measures of the patient and parents are included. Patient visits differ for each group. TSTM group patients have 15 face-to-face visits: preinclusion visit, inclusion visit, 12 training visits, and final visit. TC and CG patients have 3 face-to-face visits (preinclusion, initial visit, and final visit) and 12 e-mail or phone communications during training (TC) or follow-up (CG group). This study was approved by the local Institutional Review Board (IRB).
Results:
Not applicable. This is a study protocol.
Conclusion:
This is the first study testing an augmentation strategy using either a serious videogame or chess in clinically drug-treated patients with ADHD. Using VR serious videogames present with several advantages over traditional videogames.
Trial Registration: NCT04355065.
Background
Attention deficit hyperactivity disorder (ADHD) is the most prevalent neurodevelopmental disorder, affecting 5% of children worldwide. 1 The treatment of choice is multimodal treatment (pharmacological treatment, cognitive-behavioral therapy [CBT], and/or psychoeducational guidelines for parents and teachers).2–5 We know that unmedicated children with ADHD had significantly smaller total cerebral and total white matter volumes and that medication may ameliorate this deficit. 6 Unfortunately, current multimodal treatment is necessary but insufficient for the full recovery of patients with ADHD. Therefore, ADHD symptoms may persist for years, despite these interventions, 6 and roughly 40% of patients with ADHD will still be diagnosed during adulthood. Accordingly, novel strategies targeting the cognitive rehabilitation and following augmentation strategies for patients with ADHD are warranted.7–9
CBT is the most recommended psychological treatment for ADHD. 10 CBT is aimed at improving attention span, memory, reflection, organization, planning, working memory, behavioral inhibition, and emotional control, among others. 11 But CBT has two major problems: first, it is expensive, thus preventing its generalized use within public health systems; and second, it can be boring for some children and adolescents with ADHD. 12 Therefore, it is not surprising to see the rising use of different gaming strategies, which are characterized as lower cost and more fun than CBT and other traditional psychotherapies used in ADHD patients.
For instance, traditional cognitive games such as chess 12 or the game of “Go,” 13 which use a universal “language” and are cheap, have gained some support for use in different mental disorders.14–17 Chess allows one to work on attention, concentration, memory, planning, organization, impulse control, coping, problem solving, and emotional intelligence, among others. 12 Furthermore, there is preliminary evidence suggesting that chess can help to improve core ADHD symptoms. 12
In addition to traditional cognitive games, serious videogames, either 2D18,19 or virtual reality (VR), 5 have begun to be used to treat children and adolescents with ADHD. The use of computer programs offers a better experience and motivation for them. 20 VR allows the generation of immersive experiences, thus facilitating their transference into daily life. 21 VR also provides greater flexibility in each session, creating a safe and effective environment. All these characteristics favor a greater sensation of well-being and adherence to treatment. 22
VR is useful for treating various mental disorders23,24 such as phobias and other anxiety disorders,25–27 adaptative disorders, 28 autism spectrum disorder,29,30 and ADHD.31,32 Indeed, a VR videogame demonstrated superiority over medication in commissions in a virtual classroom after therapy. However, methylphenidate was superior to either psychotherapy or cognitive remediation with the VR videogame. 33 Other studies have suggested that Neurofeedback plus VR videogames particularly enhanced inhibitory and attentional control in ADHD.34–36
All these studies provide the rationale for the present study following an add-on strategy.8,9 We compared the efficacy of two different cognitive tools in drug-treated, clinically stable ADHD patients: (1) online chess and (2) The Secret Trail of Moon (TSTM), a brand new VR serious videogame, specifically developed for the treatment of patients with ADHD. 37 The main aim of the TSTM study is to evaluate the nonequality of both online chess and TSTM versus a control group (CG) (no intervention) in the treatment of pharmacologically stable, previously optimally titrated patients with ADHD. The primary end point is the change from baseline to end of treatment in the parent-rated “Behavior Rating Inventory of Executive Function-2” (BRIEF-2). 38 We hypothesized that the decrease in the parent total score between baseline (inclusion visit) and end of treatment (final visit) would be superior in both the TSTM and chess groups compared to the CG.
Materials and Methods
The study is a prospective, unicentric, randomized nonequality trial in 105 ADHD patients. All participants were drug titrated to become clinically stable before baseline. Subjects were randomized into three groups: TSTM group (Cognitive Training TSTM), therapeutic chess (TC, online cognitive training with chess), and CG (patients are called every week but there is no cognitive intervention). The allocation ratio has been equal in all three groups, 35 per branch.
Objectives
The main objective is to demonstrate the nonequality of both cognitive trainings over purely pharmacological treatment (CG) in children and adolescents with ADHD. Effectiveness is evaluated by the change produced between the baseline assessment (Day 0) and the final visit assessment (Day 90) in the improvement of cognitive functions, assessed with the parent BRIEF-2. 38
The secondary objectives are to research the effects on:
Attention-Deficit Hyperactivity Disorder Rating Scale-5 - (ADHD-RS-5) (Parents)1,39,40 Swanson, Nolan, and PelhamRating Scale [SNAP-IV] (Parents)41,42 Patient and Parents TEA Questionnaire for the Evaluation of ADHD and Executive Functions (ATENTO).46,47 Emotional Quotient Inventory: Youth Version (BarOn EQ-i:YV) (Patients).48,49 Patient's Conners Continuous Performance Test 3rd Edition (Conners CPT 3).50,51 Udvalg für Kliniske Undersolgelser (UKU) side effect questionnaire
52
(just in the TSTM group, at the end of each session). Clinical Global Impression (CGI) scale (both Severity, CGI-S; and Improvement, CGI-I) (Clinicians).
53
Subjects
This study includes patients of ages 12–22 years old, diagnosed with ADHD, and optimally titrated with any of the first-line ADHD drugs commercialized in Spain (methylphenidate, lisdexamfetamine, guanfacine, or atomoxetine).
Eligibility criteria
A patient is eligible if he/she meets all of the following criteria:
Adolescents and young adults (male and female) between ages 12 and 22 years old.
ADHD diagnosis (DSM-5 criteria).
Patients clinically stable (as measured by the CGI-S scale with a score ranging between 2-borderline mentally ill and 4-moderately mentally ill) on any ADHD drug.
Signature of informed consent by the patient and their parents (in all patients aged 12–17 years).
A patient is excluded if he/she meets any of the following criteria:
Comorbidity with either autism spectrum disorder or mental retardation.
Suffering from epilepsy or any other chronic severe medical illness such as severe cardiac disease based on clinical opinion.
Plans to move during the next 3 months.
Plans to begin any other psychological treatment, including cognitive-behavioral psychotherapy in the next 3 months.
Significant risk of suicidal behavior assessed by the clinician.
Study flow
All participants were recruited in the psychiatric outpatient clinics of the Puerta de Hierro University Hospital (Majadahonda, Spain) (Fig. 1). The first patient was enrolled on December 18, 2019, and the last patient was enrolled on November 16, 2020. The last evaluation was performed on February 6, 2021.
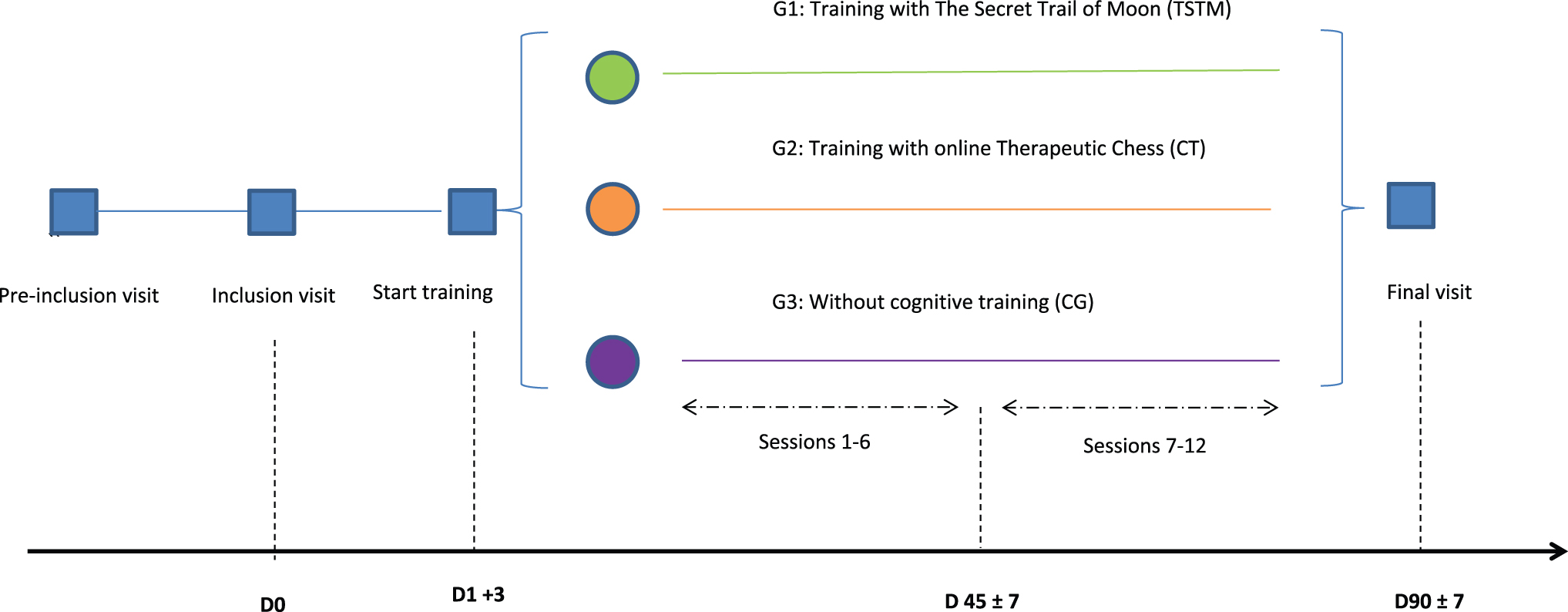
Flow chart study design. Color images are available online.
The number of visits is dependent on each intervention group:
The TSTM group has 15 face-to-face visits during the 3 months: preinclusion, inclusion visit (D0), 12 visits (1/week) of cognitive training using TSTM, and postevaluation visit (D90).
TC group and CG have 3 face-to-face visits and 12 remote visits through e-mail and/or telephone during the 3 months: preinclusion visit (face-to-face), inclusion visit (face-to-face) (D0), 12 communications (remote visits), and postevaluation visit (face-to-face) (D90).
Table 1 summarizes all visits. At preinclusion, the health staff explained the investigation to the patient and to his or her parents in those ages 12–17. If they gave their approval to participate, a date was set to begin the investigation (D0). At the initial inclusion visit (D0), all patients and their parents signed the informed consent. They were given an ad hoc questionnaire about their medical history. Patients were then examined and assessed for ADHD symptoms, executive functioning, and emotional intelligence. The severity of ADHD symptoms was assessed with the (ADHD-RS-5),1,39,40,54 CPRS scale (parents),43–45 SNAP-IV scale (parents),41,42 ATENTO scale (patient and parents),46,47 and CPT-3 (patient).50,51 The Behavior Rating Inventory of Executive Function (BRIEF-2) questionnaire (parents) measured executive functioning. 38 The BarOn EQ-i:YV questionnaire measured the patient's emotions.48,49
Description of Visits and Questionnaires
1 Only the TSTM group, after each cognitive training, will complete the “UKU” scale.
ADHD-RS, Attention Deficit Hyperactivity Disorder-Rating Scale; ATENTO, TEA Questionnaire for the Evaluation of ADHD and Executive Functions; BarOn EQ-I:YV, Emotional Quotient Inventory: Youth Version; BRIEF-2, Behavior Rating Inventory of Executive Function-2; CPRS, Conner's Parent Rating Scale; CGI, Clinical Global Impression; CPT-3, Continuous Performance Test 3rd Edition; TSTM, “The Secret Trail of Moon”; UKU, Udvalg für Kliniske Undersolgelser.
After the D0 evaluation, patients are randomized into one of the three groups: (1) TSTM (n = 35); (2) TC (n = 35); and (3) CG (n = 35). The final postevaluation visit (D90) is face-to-face for both patients and parents. The patients and parents are evaluated using the same battery of questionnaires deployed at D0.
Interventions
The Secret Trail of Moon
TSTM is a VR serious videogame developed for enhancing five main basic cognitive functions (attention, visuospatial capacity, planning, memory, and reasoning) and three secondary cognitive functions (inhibitory control, cognitive flexibility, and processing speed). Five mechanical operations were created and designed to train patients in each of the basic cognitive functions. Each of these mechanical operations is made up of different levels with increasing difficulty (Table 2).
Name of the Designed Applications, Main and Secondary Training Cognitive Areas, and Specification of the Progression Parameters of Each Mechanics
The technology is based on VR headset, an actual gaming console, and a stand-alone application. The software runs on a Playstation 4 test device, which supports VR and gaming features, such as movement tracking through camera and input detection. During the use of the application, the software collects data from the player (position, view, head movement, focus, velocity), from behavior during the current operation (hits, commission misses, omission misses, reaction time), and the behavior on free roaming mechanics (time spent in each room, distraction over specifically placed stimuli) and sends it to the application core (PSICOHUD), which transforms the data into a readable medium and displays it in a visual format (graphs, curves, and spreadsheets included) on the professional display. This application currently does not interpret data per se; it just interpolates data for a better understanding of the evolution of the training.
Training with TSTM consists of a 25-minute cognitive training divided into three blocks. Two blocks of ∼10 minutes each are for training with two mechanical applications (Smasher, Kuburi, Teka-Teki, or Enigma), and a third block of ∼5 minutes is devoted to the chess engine incorporated into TSTM. We counterbalanced the sessions by randomizing the order of the blocks. All patients followed the same sequence of training (Table 3).
Specification of the Order of Cognitive Training for Each Session
TSTM training took place once a week at the Puerta de Hierro University Hospital. The patient puts on the VR glasses and a pair of headphones and then is given the control of the console to play the game. In each session the predetermined operation is performed in advance. The patient always starts with level 1 (tutorial) in each of the applications. When a mechanical application is repeated, the patient continues at the level reached in the previous session of that application. At the end of each level, the patient receives feedback on their performance in the operation. If the patient's performance is satisfactory, he/she moves to the next level. If the performance is not good, the level must be repeated (see Table 2, which shows the data used to evaluate the progression in each application) (Supplementary Figs. S1–S3).
Therapeutic chess
Patients randomized to TC have 3 face-to-face visits: preinclusion visit, initial pretest evaluation (D0,) and final post-test evaluation (D90); and 12 communications either by telephone or e-mail with a psychologist.
At D0 the patients receive a pen drive with a 12-week chess training schedule. Each session is devoted to working different cognitive areas (see Table 4: detailed information about each session). The level of difficulty increases progressively every week. Each patient will have to do one session per week that takes ∼40 minutes per session. Each chess session has:
Summary of the Content of the Online Chess Group Sessions
A video tutorial: Weekly videos with chess lessons (n = 12, one per week, 15 minutes each) recorded by a psychologist from the team who is an expert on chess. Each week a chess concept is explained.
Traditional chess exercises: These exercises are related to the video tutorial of the week.
Therapeutic chess exercises: These exercises use the elements of chess (pieces and board). However, the exercises can be done without knowing how to play chess. These exercises are aimed at working on a specific cognitive area each week (attention or executive functions).
At the end of the week, each patient should send an e-mail with the completed exercises. In return he or she received a personalized e-mail about his or her performance.
Finally, patients in the chess group are encouraged to play a minimum of two online games per week on the chess platform chess24.es Each patient has an anonymous code so we can track the progress and time played by each patient.
Control group
CG patients have three face-to face visits: preinclusion visit, initial pretest evaluation (D0), and final post-test evaluation (D90); and 12 communications with the psychologist through telephone or e-mail. The 12 telephone communications consist in a short (5 minutes) call, one per week. During the clinical trial, patients in the CG should not undergo any psychological intervention.
Assessments
Clinical protocol
The clinical protocol includes an ad hoc questionnaire that asks about biographical data and medical and clinical history of the patient and family members. Previous psychological interventions and concomitant medical treatments are also recorded.
Psychometric assessments
Behavior Rating Inventory Executive Function (parents)
The BRIEF-2 is a questionnaire designed for the evaluation of executive functions in children and adolescents. The BRIEF-2 has 63 items with three response options (never, sometimes, and frequently) providing information on four general indexes: emotional regulation, cognitive regulation, behavioral regulation, and global index of executive function. 38
Attention-Deficit Hyperactivity Disorder Rating Scale-5 (parents)
The ADHD-RS-5 is a tool providing information on 18 ADHD symptoms: 9 for inattention, 6 for hyperactivity, and 3 for impulsivity. Six or more attention deficit symptoms and/or six or more hyperactivity-impulsivity symptoms must be present to be diagnosed with ADHD. Depending on the symptoms met, the inattentive, hyperactive-impulsive, or combined profile is specified.1,39,40,54
The Swanson, Nolan, and Pelham Rating Scale (parents)
The SNAP-IV is a frequently used scale to evaluate the core symptoms of ADHD. The SNAP-IV has 18 items, each scored using a 4-point Likert scale ranging from 0 (not at all) to 3 (very much) (range 0–54). The cutoff points for attention deficit are 2.56 and 1.78 for teachers and parents, respectively, and for hyperactivity-impulsivity 1.78 and 1.44 for teachers and parents, respectively. For both components, the cutoff points are 2 and 1.67 for teachers and parents, respectively.41,42 The SNAP-IV is one of the most frequently used scales for monitoring the response to treatment and was used in the MTA study. 3
The Conners Abbreviated Symptom Questionnaire (parents)
The CPRS is a 10-item, 4-point Likert validated screening instrument for ADHD.43–45
Emotional Quotient Inventory: Youth Version (patients)
The BarOn EQ-i:YV is a 60-item Likert questionnaire developed by Bar-On and Parker to measure the social and emotional intelligence of young people. 55 The BarOn has four subscales that provide information on total emotional intelligence: intrapersonal, interpersonal, stress management, and adaptability.48,49
TEA Questionnaire for the Evaluation of ADHD and Executive Functions (ATENTO) (patients and parents)
The ATENTO is a yet nonvalidated questionnaire providing a more complete profile of ADHD than other instruments, as the ATENTO also includes information on executive and social domain functioning. The ATENTO questionnaire evaluates attention control, emotional regulation, behavioral regulation, planning and organization, flexibility, working memory, temporal orientation, behavioral problems, problems related to sleep, and the impact of symptoms on family, social, and school domains. 46 The ATENTO questionnaire uses a Likert scale in which 1 = Never or almost never, 2 = Rarely, 3 = Sometimes, 4 = Many times, and 5 = Always or almost always. 47
Conners CPT-3 (patients)
The Conners CPT-3 is a computerized, standardized, and validated attention and go/no go test measuring impulsivity and attention. The test consists of pressing a button each time a letter (target) appears on the screen, except for the letter X (nontarget), which should not be pressed. The CPT-3 takes around 14 minutes, and the presentation interval between letters is variable (1, 2, and 4 seconds). The test provides results on hits, error of omission (undetected target), and errors of commission (reacted nontarget), which are considered a measure of impulsivity. In addition, CPT-3 provides information on mean reaction time and reaction time variability of hits.50,51
Udvalg für Kliniske Undersolgelser
The UKU is a tool designed to evaluate possible secondary symptoms. The TSTM group will complete the scale after each cognitive training session.53,56
CGI scale (clinicians)
The CGI 53 is a clinician-administered tool giving a scoring of initial severity ranging between 1 (normal) and 7 (among the most extremely ill patients) (CGI-S). During follow-up visits, CGI-I 7-point scale is used to rate the patients' total improvement by comparing their baseline assessment ranging from 1 (very much improved) to 7 (very much worse).
Analysis
Sample-size calculation
The main objective is to change the score of the initial pretest visit (D0) and final post-test visit (D90) in the BRIEF-2 questionnaire. We hypothesized that the decrease in the BRIEF-2 total score between baseline and end of treatment is superior both in the TSTM and TC groups compared to the CG group (standard treatment). Patients were randomized to three groups, but comparisons will be TSTM versus CG and TC versus CG groups.
The upper limit of the confidence interval will be 95% (two sided) for the differences among the three groups. Nonequivalence of TSTM cognitive training and TC against CG will be assumed if there is a 20% reduction in the overall BRIEF-2 score between baseline and end of treatment. We considered a reference value of 72.1 ± 15 points (mean score ± joint standard deviation) on the BRIEF-2 scale at baseline. To achieve a power of 80.00% to detect differences in the contrast of the null hypothesis H0:μ1 = μ2 by means of a bilateral T-Student for two independent samples, taking into account that the level of statistical significance is 2.50% and assuming that the average of the CG is 72.1 points on the BRIEF-2 scale, the mean of the Experimental group (TSTM and Chess, respectively) is 60 points (a 20% reduction with respect to the CG) and the joint standard deviation is 15, with an estimated loss of 10%, and using a ratio of 1:1:1 it was necessary to include 35 patients in the CG, totaling 105 patients. To sum up, we expect to find a score <60 ± 15 points after training in both active treatments (TSTM and Chess groups). The 12-point difference is considered to be clinically acceptable.
The statistical package used is Stata/IV v.15.1 (StataCorp. 2017. Stata Statistical Software: Release 15; StataCorp LLC, College Station, TX, USA).
Study populations
Following similar studies, 33 three populations are defined:
Total population: All participants included in the study who signed the informed consent.
Population intention to treat (PIT): All participants who started the research and performed at least one type of intervention (TSTM, TC, or CG groups) but dropped out of the research.
Population per protocol (PP): All participants who completed 12 weeks without major deviations from the protocol.
Demographic and baseline characteristics
The results of the baseline will be computerized for the PIT and PP groups.
A descriptive analysis of the categorical variables will be performed using absolute and relative frequencies and, in the numerical variables, using the mean and standard deviation or median and 25th and 75th percentiles, according to compliance with the assumption of normality.
The analysis of the main variable (score on the BRIEF-2 scale) in the TSTM versus CG, and TC versus CG, will be carried out by contrasting the difference of the means between pre- and postmeasures with the one-way ANOVA and post hoc analysis or Kruskal–Wallis test and then posterior Mann–Whitney U tests if the corresponding assumptions cannot be met. To avoid accumulation of Type I errors through multiple comparisons, the significance level is adjusted by the Bonferroni correction.
The effect size will be estimated with the d of Cohen, which will be interpreted according to the Cohen and Sawilowsky's categorization (<0.01: very small; 0.01–0.2: small; 0.5: medium; and 0.8 or higher: large effect).57,58
Primary end point analysis
The main objective of the study is to assess whether there is a change from the baseline (inclusion visit, D0) to the end of treatment (postevaluation visit, D90) in the total score of the BRIEF-2 scale. The upper limit of the 95% confidence interval on both sides (significance level of 0.025 on one side) will be calculated for the differences among the three groups in the primary end point [TSTM: D90-D0] − [GC: D90-D0] Y [TC: D90-D0] − [GC: D90-D0]. Nonequivalence of cognitive training with either TSTM or TC will be declared if the upper limit is greater than 12 points between group comparisons on the BRIEF-2 scale.
If no homogeneity is observed among the three groups, a linear regression will be performed to adjust for those variables that are observed to be unbalanced among the three groups.
Secondary end point analysis
All analyses of the secondary efficacy end points (CPRS, ADHD-RS-5, SNAP-IV, ATENTO, BarOn EQ-i:YV, and CPT-3) will be carried out on the PP population whenever the studied end point is available at both D0 and D90. The groups will be compared by means of a contrast of means with the Student t or Mann–Whitney U test if the corresponding assumptions cannot be met. To avoid accumulation of Type 1 error by multiple comparisons, the significance level will be adjusted by the Bonferroni method. The analyses will use a statistical significance level of 5% (with two sides).
Safety and adherence analysis
All adverse events in each group will be described. For the TSTM group, we will use the UKU adverse event scale, whereas for the TC and CG we will just ask by telephone about putative adverse events taking place during each week. In addition, the use of concomitant medications will be summarized by therapeutic class using descriptive statistics. The concomitant drugs will be those that the patient has taken while in the study.
Adherence will be described in each group during the treatment period using:
The number of sessions completed in the two cognitive training groups (TSTM and chess).
Percentage of drug adherence: number of pills taken/number of pills that should have been taken during the treatment period.
Discussion
ADHD is the most common neurodevelopmental disorder in children and adolescents worldwide. 1 Multimodal treatment of ADHD is necessary but not sufficient for halting the progression of ADHD in some patients, and around 40% of children and adolescents continue to meet ADHD criteria in adulthood. 59 The basis of multimodal treatment of ADHD is the combination of either stimulant or nonstimulant drugs and psychotherapy. Unfortunately, psychotherapies for ADHD in children and adolescents are: (1) sometimes perceived as boring, (2) time consuming, and (3) expensive. Accordingly, we need efficient treatments that are fun, less time consuming, and cheaper than current approaches. 12
This article presents the protocol and design of a prospective, unicentric randomized study with three lines of intervention for patients diagnosed with ADHD and clinically stable under ADHD drug medication treatment. The most innovative aspect of the study is the use of a VR serious videogame and online chess as cognitive training tools that may be considered new psychotherapeutic approaches.
The VR serious videogame presented here (TSTM) has several advantages over other treatments: (1) the feeling of immersion in the scenarios; (2) the variety of mechanics, each devoted to the treatment of a specific ADHD problematic area; (3) customization (personalized medicine); and (4) the gaming strategy. First, the immersive aspect of each treatment scenario makes the patient better able to focus his attention on execution, thus avoiding distraction from irrelevant elements.22. In addition, VR immersion facilitates the transference of training to daily life.21,60 Second, TSTM has six different operations for treating six critical areas for patients with ADHD (attention, memory, visuospatial capacity, reasoning, impulse control, and planning)61,62 plus three secondary cognitive areas: inhibitory control, cognitive flexibility, and processing speed. Third, the personalization of training 22 allows for a gradient increase in difficulty of execution according to the performance of each patient. Accordingly, we expect to find greater cognitive enhancement in the specific defective area of each patient. In turn, the patient can be motivated by his/her own sense of progression and improvement by reasoning about their own metacognition. 63 Finally, the playful aspect is a crucial factor.64–67 Training with videogames promote greater adherence to cognitive training.56–59
This is particularly relevant because patients with ADHD tend to get out of tasks quickly.1,61 Furthermore, we have tested the usability of TSTM in a sample of 37 children and adolescents with ADHD aged 12 or older, and 86.1% reported that they liked TSTM and 83.3% would like to continue using it. 37 Another strong point of the study is that we are using different cognitive training strategies (VR serious videogame and therapeutic chess) against a CG that does not get any type of intervention. In other words, we used a CG. In addition, this will allow us to investigate whether cognitive training through new technologies is superior to training with chess. Traditional games such as chess 12 or the Game “Go” 13 allow training in cognitive functions through a playful means. The playful aspect can also mean greater therapeutic adherence compared to some other “pencil and paper” treatment.
The current study has some limitations. First, clinicians and evaluators are not blinded to group assignment. Evaluation of patients in an unblinded situation is difficult. Indeed, we only included information provided by patients, parents, and clinicians, as the study was not designed to include information by teachers which was unfortunate, because when rating ADHD children, their ratings are considered to be more “blinded.” 68 Furthermore, in the case of clinicians, we did not use the ADHD-RS, but just used the CGI scale to evaluate the clinical improvement operated within the three groups. However, to surpass this limitation, we used some objective measures such as CPT-3.
Another limitation is the small sample size. However, we calculated sample size in advance to achieve our main objective, and the figures used were sufficient to get enough power to find statistically significant differences. Furthermore, we were able to recruit all patients under very difficult times (COVID-19 pandemic). Even more importantly, we have already finished treatments and we had less than 10% of the expected missing patients, thus reducing a compromise of our statistical analyses.
Furthermore, our results cannot be generalized to ADHD patients aged 11 or less, as we included young patients aged 12 or older. Moreover, we followed the official recommendation of the Play Station company advice against the continued use of VR videogames by children under 12 and patients suffering from epilepsy (http://legaldoc.dl.playstation.net/ps3-eula/psn/e/e_health_es.html). Furthermore, we included patients aged between 12 and 22 years old, thus including adolescent and young adult patients, which can sound awkward. Our research decision was based mainly on two reasons: (1) A neurodevelopment reason: there is increasing evidence that brain maturity is reached into the 20s 69 ; and (2) A clinical and organizational reason: patients seen by clinicians in the Child and Adolescent Mental Health Services (CAMHS) are progressively referred to be followed up in Adult Mental Health Services (AMHS). Thus, some patients are already followed up in the CAMHS at the age of 20 years, but occasionally this period can be extended up to ∼22 years of age. In any case, we took care of all legal issues regarding age-related issues, and our protocol was approved by the local ethics committee.
Finally, we used a yet unvalidated, brand-new questionnaire only available in Spanish for evaluating the severity of ADHD (ATENTO). We used the ATENTO questionnaire because this questionnaire evaluates not only the core ADHD clinical symptoms but also executive functions and the impact of ADHD symptoms in several domains, including the social area. However, we also retrieved information regarding severity of ADHD with other ADHD scales such as the SNAP-IV. Finally, another limitation is the lack of long-term follow-up of patients to determine whether the possible therapeutic effects are maintained over time.
In conclusion, this trial is a prospective, randomized single-center study that aims to demonstrate how cognitive training with a videogame of VR added to drug treatment reduces the symptoms of patients diagnosed with ADHD.
Footnotes
Authors' Contributions
M.R.-Y., M.M.-M., C.G.-T., and H.B.-F. have designed the videogame. M.R.-Y., M.M.-M., and H.B.-F. carried out the research. M.R.-Y., A.M.-G., and H.B.-F created the databases and incorporated the data. A.R., M.R.-Y., and H.B.-F. will analyze data. All authors have read and approved the latest article.
Acknowledgments
The authors thank all the staff involved in the research and the Company Gammera Nest. The authors also thank TEA ediciones and especially Fernando Sánchez for providing some of the evaluation questionnaires (i.e., ATENTO). The authors thank all the children, adolescents, and parents for their participation in this study. Finally, the authors thank Lorraine Maw, MA, for her editorial assistance.
Ethics Approval and Consent to Participate
This Project: “Randomized study of personalized cognitive training with Virtual Reality technology (The Secret Trail of Moon) versus online therapeutic chess cognitive training versus usual treatment (TAU) in Attention Deficit Hyperactivity Disorder (ADHD): a clinical trial” was approved by the Ethics Committee at Puerta de Hierro University Hospital in Majadahonda on November, 26, 2019; PI 187/19. All participants in this study were duly informed of the intervention. Both parents and patients were informed that they could leave the study at any time they wish. The data will always be treated anonymously and exclusively in the HUPHM environment.
Consent for Publication
Consent was obtained from all participants.
Author Disclosure Statement
In the last 24 months, H.B.-F. received lecture fees from Shire. He is Principal Investigator (PI) of an iPFIS research contract (![]() ; IFI16/00039) and co-PI of a MINECO research grant (RTI2018-101857-B-I00); recipient of: (1) a FIPSE Grant, and (2) an IDIPHIPSA intensification grant; involved in two clinical trials (MENSIA KOALA, NEWROFEED Study; ESKETSUI2002); member of the Advisory Board of ITA Salud Mental. Maria Rodrigo-Yanguas is the recipient of an iPFIS research contract (www.isciii.es; IFI16/00039). Marina Martin-Moratinos is the recipient of a CDTI grant (FEDER funded; IDI-20180701, file 00107278). The remaining authors do not have any conflict of interest regarding the publication of this article.
; IFI16/00039) and co-PI of a MINECO research grant (RTI2018-101857-B-I00); recipient of: (1) a FIPSE Grant, and (2) an IDIPHIPSA intensification grant; involved in two clinical trials (MENSIA KOALA, NEWROFEED Study; ESKETSUI2002); member of the Advisory Board of ITA Salud Mental. Maria Rodrigo-Yanguas is the recipient of an iPFIS research contract (www.isciii.es; IFI16/00039). Marina Martin-Moratinos is the recipient of a CDTI grant (FEDER funded; IDI-20180701, file 00107278). The remaining authors do not have any conflict of interest regarding the publication of this article.
Funding Information
This research was partially funded by: the Spanish National Project (Grant number RTI2018-101857-B-I00 (H.-B.-F.)), FIPSE (H.B.-F.), CDTI (M.M.-M.), and ISCIII (i-PFIS contract, M.R.Y. and H.-B.-F.).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.