
Abstract
The aim was to systematically review the effects of gaming on pain-related fear, pain catastrophizing, anxiety, and depression in patients with chronic musculoskeletal pain. Databases (Medline, EMBASE, PsycInfo, CINAHL, Cochrane Central Register for Controlled Trials [CENTRAL], Web of Science, and SCOPUS) were searched from inception up to October 2021. Two reviewers independently selected randomized controlled trials that compared the effects of any gaming modality with other interventions or no treatment on pain-related fear, pain catastrophizing, anxiety, and depression. For data synthesis, Standardized Mean Differences (SMDs) and 95% confidence interval (CI) were calculated using a random-effects inverse variance model for meta-analysis according to the outcome of interest, comparison group, and follow-up period. The level of evidence was synthesized using Grading of Recommendations, Assessment, Development, and Evaluations (GRADE). Thirteen studies were included with a total sample of 680 patients. Gaming was superior to other treatments and no treatment on reducing pain-related fear (SMD: −1.23; 95% CI: −2.02 to −0.44) and anxiety (SMD: −0.55; 95% CI: −1.01 to −0.09), respectively. Gaming was not superior to other treatments on reducing pain catastrophizing, anxiety, and depression, and it was not superior to no treatment on reducing pain-related fear, pain catastrophizing, and depression. Those findings were based on very low or low-quality evidence. In a conclusion, gaming modalities may have positive effects on some mental health outcomes. However, there were conflicting results with low-quality evidence, which indicates that more high-quality randomized controlled trials are needed.
Introduction
Chronic musculoskeletal pain is the most prevalent debilitating condition in the general adult population, placing a heavy burden on society and health care systems with a significant economic impact. 1 According to the World Health Organization, ∼1.71 billion people worldwide have a persistent musculoskeletal condition. 2 Chronic musculoskeletal pain arises from different etiologies3,4 and is associated with impaired function, daily living activities, and health-related quality of life. 5
The management of musculoskeletal pain has been traditionally based on tissue damage. 4 Current evidence has shown that the painful symptoms and/or disability were not necessarily related to a specific tissue injury,3,6 and the psychological and social factors have an important role in health-related outcomes.6,7 The musculoskeletal conditions also negatively impact patients' mental health, associated with depression, anxiety, and other psychological or social-related impairments.6,8 Additionally, a large number of systematic reviews concluded that psychological factors play an important role in the onset and chronicity of musculoskeletal conditions, including pain-related fear, pain catastrophizing, anxiety, and depression.9–11
Previous systematic reviews indicated that videogames may have positive effects on biopsychosocial factors. They may decrease pain and improve function in patients with low back pain, 12 enhance cognition and lower depressive symptoms in older adults, 13 reduce fatigue, improve quality of life and balance in patients with multiple sclerosis, 14 and reduce stress and anxiety in other patients. 15 Exergames are a modality of videogames that require physical activity interaction, and are shown to be effective to counter sedentary lifestyles and are viable to treat patients with musculoskeletal conditions. 16 Virtual Reality is a goal-focused computer-simulated reality, acting on the user's experience of their perceived world through head-mounted displays, headphones, and motion tracking systems. 17
Virtual reality is a useful tool for the assessment and treatment of mental health conditions, 18 and has also been used in different clinical settings to ameliorate pain perception.19,20 Although gaming modalities may improve mental health-related outcomes in patients with musculoskeletal conditions, this topic has not been previously explored by a systematic review. Therefore, this review aims to summarize and analyze the current evidence regarding the use of games and virtual reality to improve mental health-related outcomes in patients with chronic musculoskeletal pain.
Methods
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement and checklist (Supplementary Data—Prisma Checklist). 21 The review protocol was registered in the international database PROSPERO (CRD42021285290).
Selection criteria for including studies
Study design
This review included randomized clinical trials. Preliminary reports, feasibility trials, or pilot studies were not included.
Patients
Studies were included if they assessed adults (older than 18 years) of either sex, with chronic musculoskeletal pain (e.g., back, neck, and shoulder pain; osteoarthritis; fibromyalgia).
Intervention
Studies that delivered digital gaming modalities and gaming technology as a treatment were included (e.g., casual games, serious games, gamification, virtual reality, exergames). Digital gaming modalities were defined as any sort of intervention using computerized and graphically manipulated images forming a game, 22 to improve health-related outcomes. 23 The duration of the interventions was defined as short term (≤6 months), intermediate term (between 6 months and 1 year), and long term (≥1 year).
Comparison
Studies were considered eligible if the control group was no treatment (waiting list, sham, or placebo) or other intervention. Studies that used any gaming modality in the comparison group were not included.
Outcome measures
Studies were included if at least one of the following mental health-related outcomes was assessed: pain-related fear (e.g., kinesiophobia, fear avoidance), pain catastrophizing, anxiety, and depression. These outcomes are related to worse health-related outcomes in patients with chronic pain and are often assessed through patient self-reported outcome measures. 10
Search methods for identification of randomized controlled trials
Electronic searches
The databases, MEDLINE, Embase, PsycInfo, CINAHL, Cochrane Central Register for Controlled Trials (CENTRAL), Web of Science, and Scopus, were searched from their inception to October 2021. A search strategy was developed using relevant keywords, which were combined with Boolean terms. The detailed search strategy is described in Supplementary File S1.
Data collection and analysis
Study selection
Two independent reviewers (V.G. and H.R.F.F.) selected the studies and a third reviewer (G.M.B.) was consulted in case of any disagreement. The primary studies were initially assessed by title and abstract to exclude those that did not fit the eligibility criteria. Afterward, the full texts of the remaining studies were assessed. Reference lists from the included trials were screened for potential additional trials that fit the inclusion criteria.
Methodological quality assessment
The Physiotherapy Evidence-Based Database (PEDro) scale was used to assess the methodological quality. PEDro is considered a reliable critical appraisal tool for experimental studies in physical therapy, 24 contains 11 criteria to assess the methodological quality of clinical trials, and the final score ranges from 0 to 10. If a criterion was not described or was unclear, no point was awarded. The previously indexed studies in the PEDro database had their score maintained. The non-indexed studies were independently evaluated by two reviewers (V.G. and H.R.F.F.), and a third reviewer (G.M.B.) solved inconsistencies of the rating when necessary. Studies scored 5 or more were classified as having high methodological quality. 25
Data extraction and management
Two reviewers (V.G. and H.R.F.F.) independently extracted data according to the Cochrane data collection form, and a third reviewer (G.M.B.) checked data in case of discrepancies. Data regarding patients, interventions, trial methods, outcome measures, the dose of interventions, duration of follow-ups, loss to follow-ups, and results, were extracted. The authors of the primary studies with missing or unclear data were contacted if necessary. In case the contacted authors did not respond, the missing data were calculated from mean change, graphical data, standard error (SE), or baseline standard deviation (SD). 26
The studies were initially analyzed according to the outcome of interest (pain-related fear, pain catastrophizing, anxiety, and depression) and control group (non-treatment or other interventions). Subsequently, a subgroup analysis was performed according to the gaming modality used in the studies, such as virtual reality or exergame.
Data synthesis and analysis
Meta-analyses were conducted using RevMan (version 5.4.1; The Nordic Cochrane Center, Copenhagen, Denmark) to summarize the effects of gaming on mental health outcomes in patients with chronic musculoskeletal pain. Meta-analysis was conducted using means and SDs of the data after the intervention from each of the eligible trials. Standardized Mean Differences (SMDs) and 95% confidence intervals (CIs) were calculated using a random-effects inverse variance model for meta-analysis. Based on similar systematic reviews,27,28 subgroup analyses were used to verify differences between interventions (virtual reality or exergame) on the pooled treatment effect. I2 statistic was used to assess heterogeneity between trials. 26 SMDs were classified as small (<0.20), medium (between 0.21 and 0.80), and large (>0.80). 29
The evidence synthesis for each meta-analysis was performed using the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) approach, 30 according to the following domains.
Risk of bias: quality of the evidence was downgraded by one level if more than 25% of the patients were from trials with low methodological quality. It was downgraded by two levels if more than 50% of the patients were from studies with low methodological quality.
Inconsistency: quality of the evidence was downgraded by one level if significant heterogeneity was observed in the results (i.e., I2 > 50% and P < 0.05 on the heterogeneity test), minimal or no overlap of CIs, and wide variance of point estimates across studies. It was downgraded by two levels in case of serious inconsistency (heterogeneity in the I2 test >75%).
Indirectness: quality of the evidence was downgraded if patients, interventions, or outcome measures from included studies were essentially different. This domain was not downgraded by two levels.
Imprecision: quality of the evidence was downgraded by one level if (A) pooled sample was smaller than 400 patients in the comparison and/or a single study with less than 400 patients; (B) wide CIs (95% of CI crossed an effect size of SMD = 0.5 in either direction). This domain was downgraded by two levels duo to both (A) and (B).
Publication bias: quality of the evidence was downgraded if the funnel plot presented asymmetrical distribution (when 10 or more studies were available), small studies were sponsored, or the investigators stated conflict of interest (publication bias criteria).
After assessing all domains, the quality of evidence for each meta-analysis was classified as one of the following levels. 31
High quality: very confident that the true effect lies close to an estimate of effect;
Moderate quality: moderately confident that the true effect is likely to be close to an estimate of effect; but there is a possibility that it is substantially different;
Low quality: confidence in the effect estimate is limited and the true effect may be substantially different from an estimate of effect;
Very-low quality: little confidence in the estimate of effect and the true effect is likely to be substantially different from an estimate of effect;
Results
The electronic search retrieved 6530 studies. Twenty-five studies were considered in the full-text eligibility assessment and 12 were excluded. The detailed reasons for exclusion are described in Figure 1. After the full reviewing process, 13 articles were included for analysis.32–44
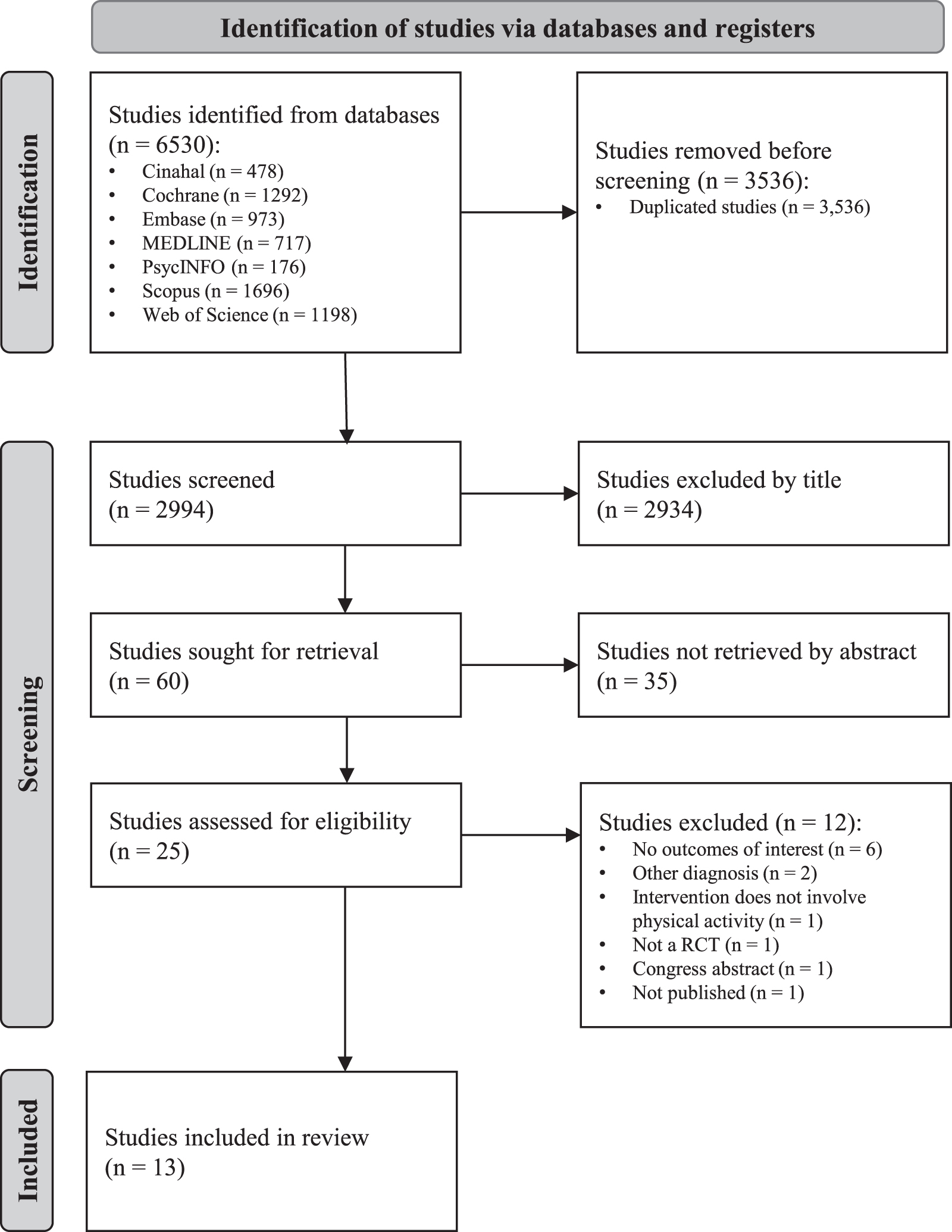
PRISMA flow diagram of search strategies and results. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RCT, randomized controlled trial.
Methodological quality
The scores from 11 studies were obtained in PEDro database, and scores from 2 other studies41,44 were assessed by the researchers. All 13 studies presented high methodological quality, with all studies satisfying the items related to random allocation, baseline comparison, and point estimates and variability (Table 1). The final PEDro score of the included studies ranged from 5 to 8 points.
Methodological Quality Evaluated According to the Physiotherapy Evidence-Based Database Scale
Eligibility criteria item does not contribute to the total score.
1, Eligibility criteria; 2, random allocation; 3, concealed allocation; 4, baseline comparability; 5, blinding of individuals; 6, blinding of therapists; 7, blinding of assessors; 8, adequate follow-up; 9, intention-to-treat analysis; 10, between-group comparisons; 11, point estimates and variability.
N, no; Y, yes.
Patients
The characteristics of the patients from the included studies are listed in Table 2. The pooled sample was 680 patients and the dropout during the intervention period was 72 patients (10.58%). The number of patients in the included studies ranged from 20 to 90 (average sample size of 52.30 patients). The patients' mean age was 45.2 years (ranging from 21.4 to 68.8), and 393 patients were women (57.79%). The included studies investigated treatments for patients with chronic low back pain,35,36,39,41,42,44 chronic neck pain,32,34 fibromyalgia,33,37,38,43 and knee osteoarthritis. 40
Characteristics of the Studies
(A) Experimental group; (B) control group.
3D, three-dimensional; 6MWT, Six-Minute Walk Test; BIA, bioelectrical impedance analysis; COM, Conditioned Pain Modulation; EQ-5D, EuroQol-5 Dimensions; EQ-5D-5L, EuroQol-5 Dimensions-5 Levels; FABQ, Fear-Avoidance Beliefs Questionnaire; FIQ, Fibromyalgia Impact Questionnaire; FSS, Fatigue Severity Scale; GPE, global perceived effect; HADS, Hospital Anxiety and Depression Scale; IPAQ, International Physical Activity Questionnaire; IQR, interquartile range; MFI, Multidimensional Fatigue Inventory; MSOT, Modified Sensory Organization Test; ND, not defined; NDI, Neck Disability Index; NHP, Nottingham Health Profile; NSAID, nonsteroidal anti-inflammatory drug; ODI, Oswestry Low Back Pain Disability Index; PASS-20, Pain Anxiety Symptoms Scale—20-items version; PCS, Pain Catastrophizing Scale; PSEQ, Pain Self-Efficacy Questionnaire; PSFS, Patient-Specific Functional Scale; RDQ, Roland Morris Disability Questionnaire; SD, standard deviation; SF-36, Short Form 36; SSS, Symptom Severity Scale; TS, Temporal Summation; TSK, Tampa Scale of Kinesiophobia; TUG, Timed-up and go Test; VAS, Visual Analog Scale; WAI, Work Ability Index; WHOQOL-BREF, World Health Organization Quality of Life-Brief Vision; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Interventions
Characteristics of the interventions of each included study are described in Table 2. Gaming interventions used virtual reality,32,34,35,38,39,41,42 exergames through videogame consoles,33,36,37,43,44 or other gaming devices (a step-sensing platform). 40 In one study, the game intervention did not involve actual active movement by the patient. 35 Most of the included trials performed the experimental treatment sessions in the clinical setting, and only two trials prescribed gaming interventions at home.32,36 Gaming interventions often included some form of aerobic, mobility, or strengthening exercises. Adherence was similar between groups across all groups when reported. The gaming interventions were classified as “Virtual Reality” when treatments involved virtual reality immersion (e.g., Oculus Rift, Pro-Kin system) or “Exergame” when other hardware was used (e.g., Nintendo Wii, Xbox Kinect).
All studies verified the short-term effects of the interventions and the duration of experimental interventions ranged between 20 and 80 minutes per session, frequency of 1–5 times per week for 2–8 weeks, with a total of 8–24 sessions. Games were compared with exercise therapy (84.61%) or no intervention (15.38%). When exercise therapy was performed, aerobic, mobility, and strengthening exercises were included in a similar manner to the experimental group.
Outcome measures
Pain-related fear was assessed with the Tampa Kinesiophobia Scale32,34–36,38,41,42,44 and the Fear-Avoidance Beliefs Questionnaire.34,39 The Pain Catastrophizing Scale was used to assess pain catastrophizing34,44 and the Pain Anxiety Symptoms Scale was used to assess anxiety. 34 The Hospital Anxiety and Depression Scale39,43 and the Fibromyalgia Impact Questionnaire were used to assess both anxiety and depression.33,37
Effects of interventions
Effects of games on pain-related fear
Seven studies32,34,35,38,39,41,42 compared the effects of games (virtual reality) with other treatment on pain-related fear (Fig. 2). Very low-quality evidence (Supplementary File S2) indicated that the games were superior to other treatments (SMD: −1.23; 95% CI: −2.02 to −0.44). Two studies32,36 compared the effects of games (virtual reality and exergames) with no treatment on pain-related fear (Fig. 2). Very low-quality evidence indicated that games were not superior to no treatment (SMD: −0.33; 95% CI: −0.77 to 0.11). Subgroup analysis showed no significant difference (P = 0.25) between the effects of virtual reality 32 or exergames. 36
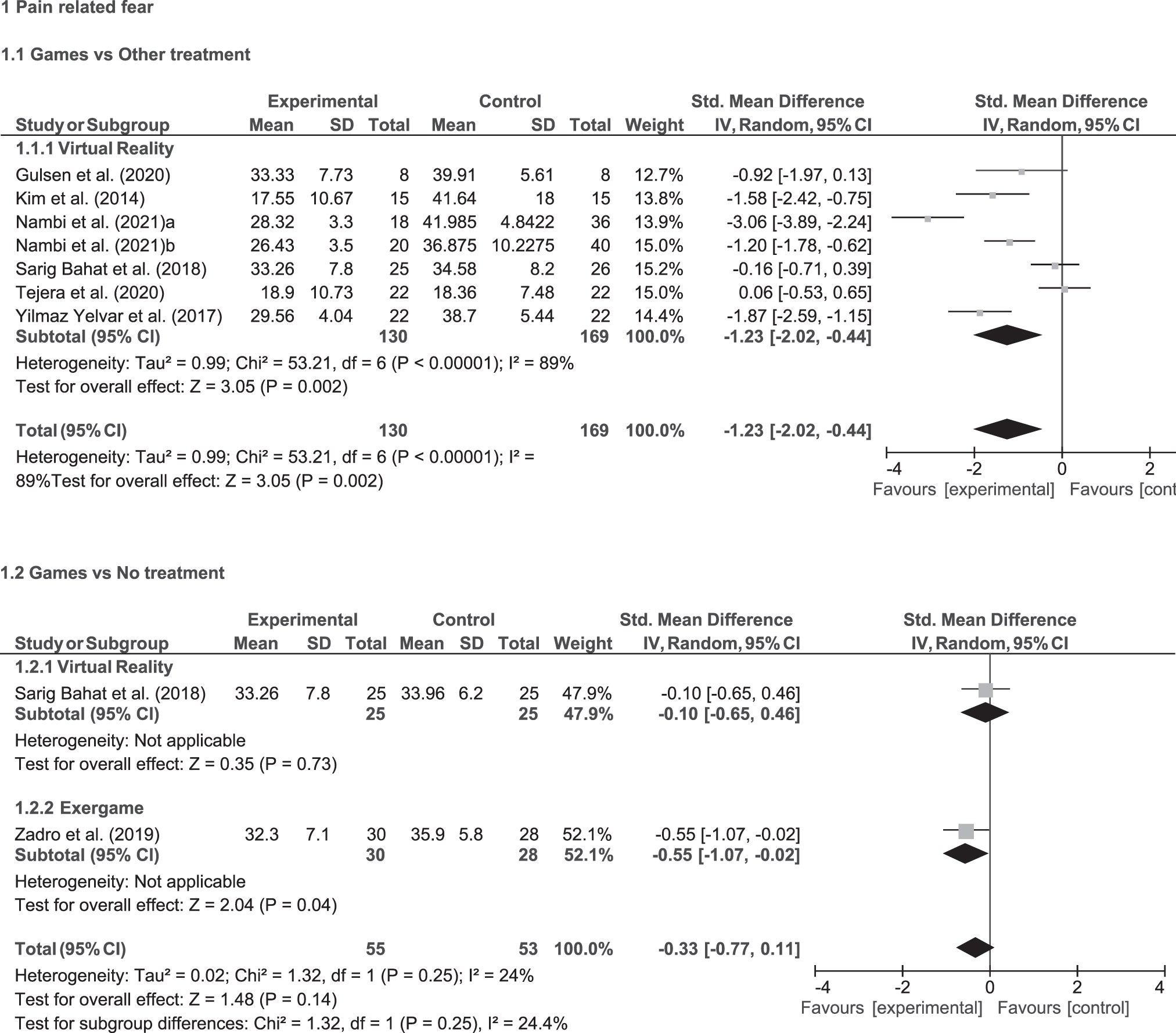
Forest plots of the overall effect of virtual reality and exergame on pain-related fear compared with other treatments or no treatment. Squares represent point estimates of treatment effect and the diamonds represent the pooled treatment effect.
Effects of games on catastrophizing
One study 34 compared the effects of games (virtual reality) with other treatments on pain catastrophizing (Fig. 3). Low-quality evidence indicated that the games were not superior to other treatments (SMD: 0.26; 95% CI: −0.34 to 0.85). Another study 44 compared the effects of games (exergames) with no treatment on pain catastrophizing (Fig. 3). Low-quality evidence indicated that games were not superior to no treatment on pain catastrophizing (SMD: −0.30; 95% CI: −0.92 to 0.33).
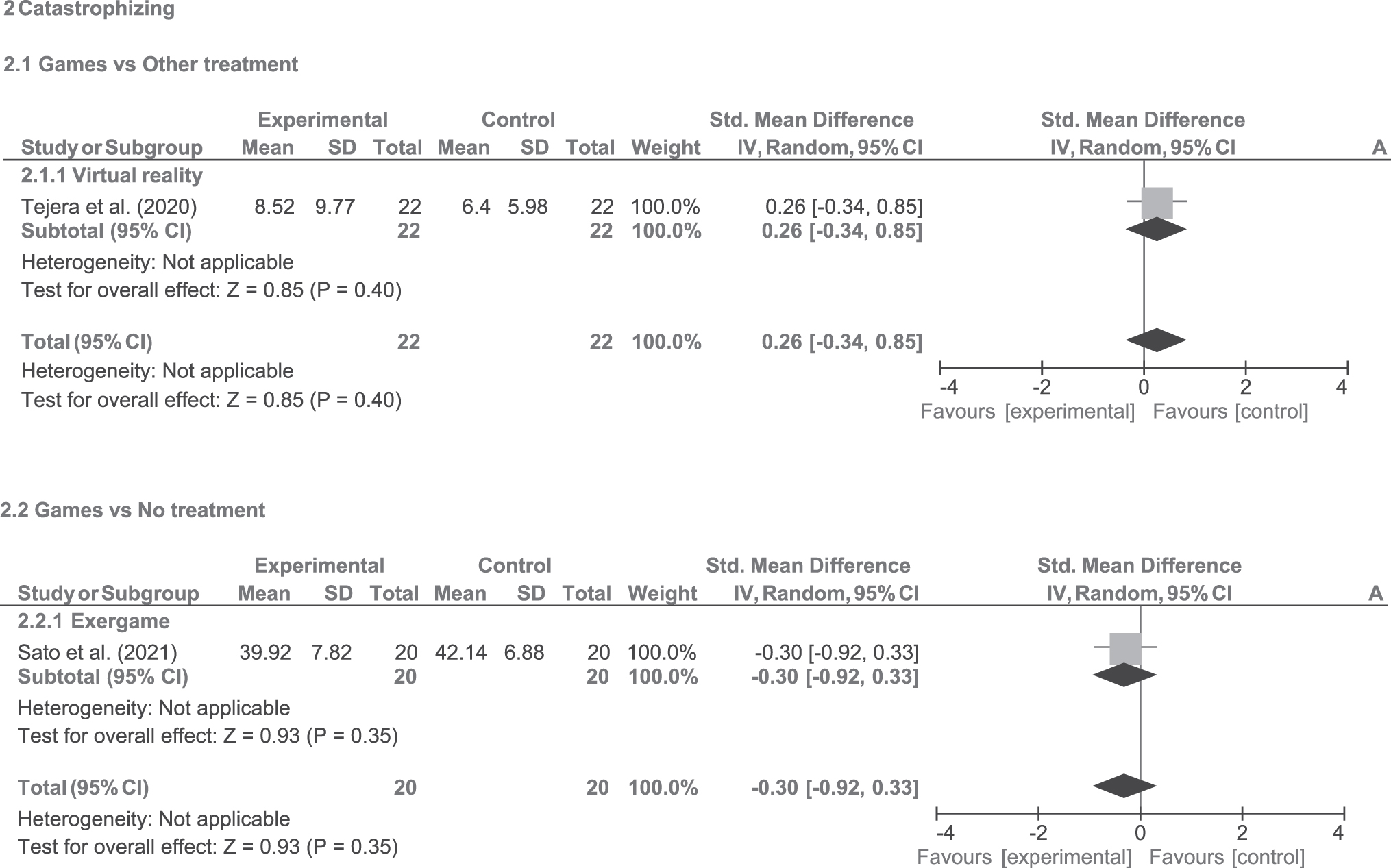
Forest plots of the overall effect of virtual reality or exergame on catastrophizing compared with other treatments or no treatment. Squares represent point estimates of treatment effect and the diamonds represent the pooled treatment effect.
Effects of games on anxiety
Four studies33,34,40,43 compared the effects of games with other treatments on anxiety (Fig. 4). Low-quality evidence suggests no difference between interventions (SMD: −0.10; 95% CI: −0.44 to 0.23). Subgroup analysis showed no significant difference between the effects of virtual reality34,43 or exergame33,40 (P = 0.40; I2 = 0%). One study 37 compared the effects of games (exergames) with no treatment on anxiety (Fig. 4). Low-quality evidence indicated that games were superior to no treatment (SMD: −0.55; 95% CI: −1.01 to −0.09).

Forest plots of the overall effect of virtual reality and exergame on anxiety compared with other treatments or no treatment. Squares represent point estimates of treatment effect and the diamonds represent the pooled treatment effect.
Effects of games on depression
Three studies33,40,43 compared the effects of games with other treatments on depression (Fig. 5). Very low-quality evidence indicated that games were not superior to other treatments on depression (SMD: −0.41; 95% CI: −1.05 to 0.22). Subgroup analysis showed no significant difference between the effects of virtual reality 43 or exergames33,40 (P = 0.83; I2: 0%). One study 37 compared the effects of games (exergames) with no treatment on depression (Fig. 5). Low-quality evidence indicated no difference between interventions (SMD: −0.38; 95% CI: −0.84 to 0.07).
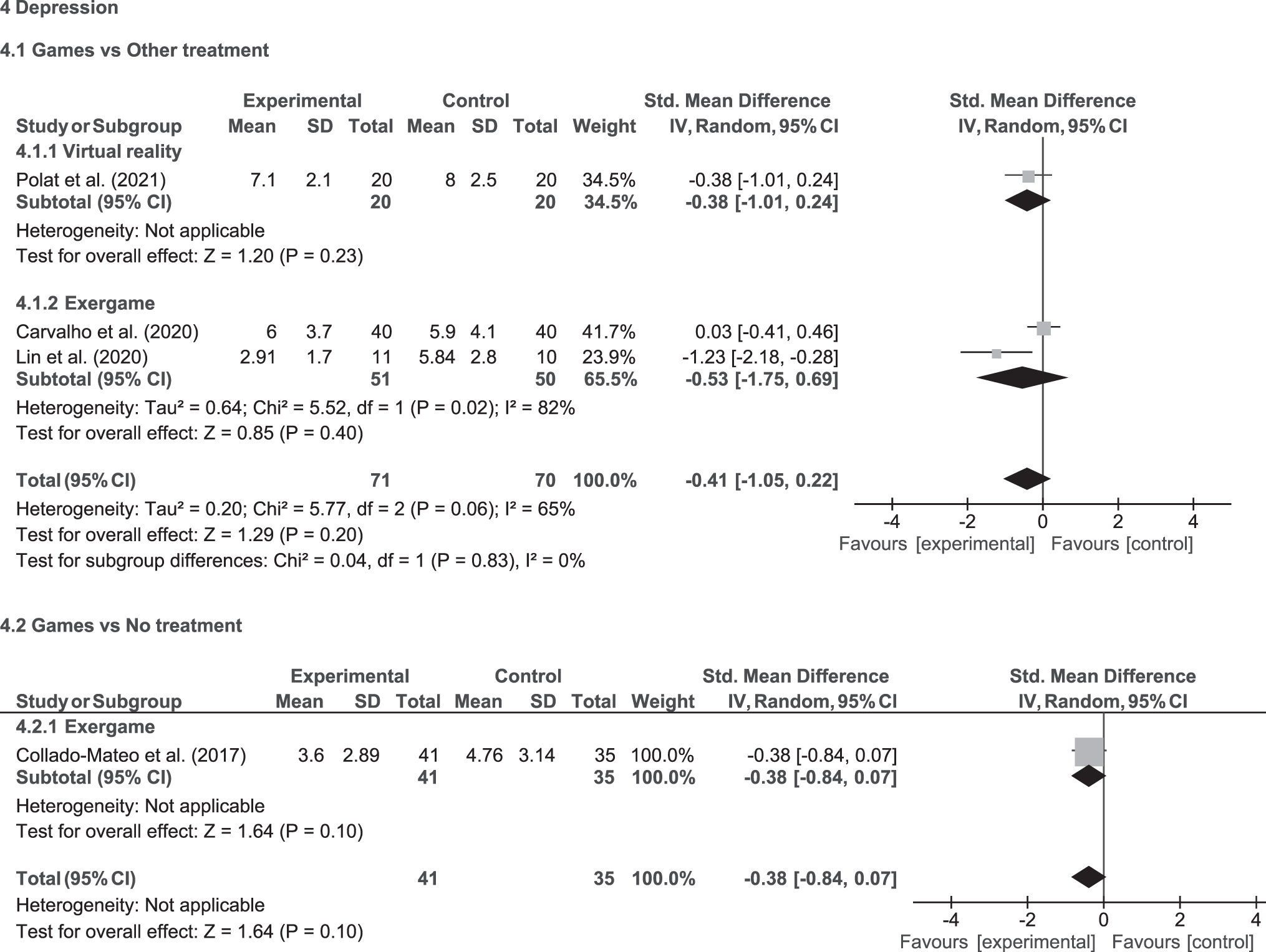
Forest plots of the overall effect of virtual reality and exergame on depression compared with other treatments or no treatment. Squares represent point estimates of treatment effect and the diamonds represent the pooled treatment effect.
Discussion
This review aimed to summarize the current evidence regarding the effects of games on mental health, including pain-related fear, pain catastrophizing, anxiety, and depression in patients with chronic musculoskeletal pain. Low and very-low quality evidence suggested that games are superior to other treatments to improve pain-related fear, and superior to no treatment to improve anxiety. Very low and low evidence suggests no difference between games and other treatments or no treatment for the other outcomes. Previous systematic reviews showed positive effects of gaming interventions on emotions and mental health in individuals with a variety of conditions,45–47 but to our knowledge, this is the first systematic review that analyzed the effects of gaming in patients with chronic musculoskeletal pain.
Chronic musculoskeletal pain negatively impacts patients' physical health, as well as psychological and social aspects, with a consequent poor quality of life.6,7,48 The effects of interventions on mental health may provide important information to assist clinicians in planning treatments for patients with musculoskeletal pain disorders. Therefore, future studies should assess these outcome measures to examine the effects of different treatments on those behavioral and psychological constructs. In our study, virtual reality interventions were superior to other treatments (e.g., exercise therapy) to improve pain-related fear in short term. Although the large effect size indicated clinically relevant results, those findings should be interpreted cautiously due to the very low quality of evidence. Additionally, gaming interventions (virtual reality and exergames) were not superior to no treatment, based on two studies32,36 that provided very-low quality evidence. Those findings indicated that more studies are necessary to strengthen the evidence.
Pain-related fear is a common behavior in patients with chronic musculoskeletal pain, associated with maladaptive learning, activity avoidance, and modified perception of pain, 17 which has a debilitating role in pain experiences.49,50 Patients with painful motion tend to adopt avoidance behaviors, which might consequently have a negative impact on functionality, quality of life, and willingness to participate in rehabilitation.51,52 Passive interventions are not effective to reduce psychological factors, including pain-related fear in patients with musculoskeletal pain.53,54 However, therapeutic exercises (which are prone to be active interventions) may have positive effects on these outcomes.54,55 Moreover, pain neuroscience education may have larger effects when associated with movement-based therapies. 56 Interestingly, our results showed that virtual reality may be superior to exercises, but the effects of virtual reality associated with pain neuroscience education, for example, are still unknown.
The theoretical mechanisms of virtual reality to improve psychological factors include distraction and graded exposure.17,18 Distraction is the redirection of an individual's attention away from pain toward other sensations, including visual, auditory, and tactile stimuli, which reduce cognitive capacity to process pain and avoidance behaviors.17,18 The graded exposure encourages a confrontation response by exposing patients to specific situations or providing graded movement exposure within simulations of real-life activities or based on the individual's personal needs. 17 It was expected that these strategies may reduce fear avoidance and kinesiophobia in patients with pain during movement, which is confirmed by our results.
Virtual reality has been used as part of the treatment for psychiatric disorders, including anxiety, 57 being able to reduce anxiety symptoms, 58 and demonstrating similar efficacy compared with traditional exposure interventions, because it has a powerful real-life impact, and demonstrates good stability of results over time. 59 Because our patients did not necessarily present psychiatric disorders, our results indicated that exergames may have a positive effect on anxiety, but both virtual reality and exergames were not superior to other interventions to reduce anxiety in short term.
Although gaming has been extensively used with therapeutic purposes with children, chronic musculoskeletal pain is more prevalent in adults than in children, 60 so this review focused on the effects of gaming in the adult population. However, the results could be different in children, depending on their previous experience with games.
Although the gaming interventions are a promising rehabilitation approach for patients experiencing pain, the current evidence does not support it to improve pain catastrophizing and depression at short-term follow-up. Nevertheless, the effects of gaming in the intermediate and the long terms are still unknown, and studies46,61 have suggested that interventions with a longer duration might provide superior outcomes on self-perceived depression and anxiety. Future gaming design focused on patients with chronic musculoskeletal pain can take into consideration their psychosocial aspects related to pain. 10 More high-quality randomized controlled trials are needed to strengthen the evidence on the effects of gaming on mental health-related outcomes.
Strengths of the review
To the best of our knowledge, this is the first systematic review that verified the effects of gaming interventions on mental health in patients with chronic musculoskeletal pain. This review provides updated evidence regarding gaming given our consideration of PRISMA, comprehensive search strategy, meta-analysis, and evaluation of the quality of the evidence according to GRADE. The results of this study can assist clinicians in making decisions regarding managing patients with musculoskeletal pain following an evidence-based practice.
Limitations
Even though studies were indicating positive effects of gaming on mental health, the results of this review should be interpreted with caution due to very low or low quality of evidence. Few studies investigated short-term effects and follow-up, and there was heterogeneity of the sample and interventions. Furthermore, publication bias was not assessed using funnel plots due to the limited number of included studies. Future randomized clinical trials with concealed allocation, blinded assessor, intention-to-treat analysis, and appropriate sample size should be performed to provide clearer evidence about the effects of different types of gaming, associated or not with other therapeutic approaches, and compared with no treatment or therapeutic exercises. We limited our population to adults only, and choosing an appropriate gaming intervention must take into consideration the playability and user experience of this specific population. 62
Conclusion
The results indicated that gaming modalities are superior to other treatments to improve pain-related fear, and superior to no treatment to improve anxiety. However, gaming was not superior to no treatment to improve pain-related fear and it was not superior to other treatments or no treatment for improving pain catastrophizing, anxiety, and depression. Those findings were based on very low and low-quality evidence, and more studies are necessary to strengthen the evidence.
Footnotes
Authors' Contributions
All persons who meet authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing, or revision of the article. Concept and research design: V.G., H.R.F.F., G.M.B., L.B.C., and D.H.K. Search strategy: V.G., H.R.F.F., G.M.B., L.B.C., and D.H.K. Data analysis: V.G. and H.R.F.F. Writing: V.G., H.R.F.F., G.M.B., L.B.C., and D.H.K.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by grant 2020/01449-5 from São Paulo Research Foundation (FAPESP) and by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES). The funding source was not involved in the design, interpretation, or writing of this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.