
Abstract
Objective:
This study assessed the initial acceptability of SafeUse, a game-based opioid misuse prevention intervention for delivery via smartphone among adolescents. Evidence-based educational and refusal skills training materials were adapted, and game design elements were applied to clinically and scientifically informed scenarios in which opioids are typically introduced to adolescents using standard product development methods to create the SafeUse prototype.
Materials and Methods:
In a mixed-methods study, 14 adolescents were assessed on their knowledge and perceptions of opioids before and following 5–7 days of access to SafeUse. Participants provided feedback in focus groups on the acceptability, relevance, and understandability of SafeUse and made suggestions for its improvement. Feedback was coded and summarized as to playability, acceptability, appropriateness, content development, and knowledge transfer. Pre- and post-access quantitative data were analyzed using Wilcoxon matched pairs signed-rank tests.
Results:
Overall, participants liked SafeUse, its characters, graphics, and approach, finding it more appealing than lectures/reading materials and appropriate for school settings. They moderately to extremely “liked the game,” “would like to play more game modules,” “liked playing through the decisions,” thought the game was realistic/relevant and fun, and they learned new information about opioids. Participants reported increased confidence to refuse opioids and decreased likelihood of accepting opioids from someone they know. Knowledge about opioids increased (P < 0.006), and adolescent perception that prescription drugs are safer than illegal drugs decreased (P < 0.003) after playing SafeUse.
Conclusion:
Findings suggest that SafeUse is acceptable and likely educational to adolescents and worthy of further development and research.
Introduction
Adolescent prescription drug misuse (PDM), including stimulant, sedative, and opioid misuse (OM), is a significant and underresearched public health problem in the United States. An estimated 16.3 million individuals aged 12+ years reported nonmedical prescription drug (PD) use 1 and 14.6% of 12th graders reported lifetime PDM 2 in 2019. Of PDs used for nonmedical purposes by adolescents, opioids have been among the most prevalent. 3 Moreover, the increase in national opioid prescriptions (e.g., hydrocodone [Vicodin®], oxycodone [OxyContin®, Percocet®], and oxymorphone [Opana®]) from 2005 to 2010 was associated with an increase in adolescent opioid abuse as well as poison center calls. 4 Initiating PDM during adolescence has also been shown to be associated with a significantly higher risk of developing a subsequent substance-use disorder relative to PDM initiation during young adulthood. 5
Although PDM prevalence overall has been declining since 2010, drug overdose rates have continued to rise from 1999 through 2017, including among adolescents aged 15–24. 6 Indeed, drug-involved overdose deaths have increased from a rate of 3.5 per 100,000 persons aged 15–24 years in 1999 to 13.0 per 100,000 persons in 2017. 7 In addition, compared with 2002, there was a 37% increase in the probably of having a prescription opioid use disorder in the past year and a fourfold increase over time in the probability of heroin use among emerging adults with PDM in 2014. 8 Deaths from PD overdose among adolescents are increasing, with 4633 adolescents aged 15–24 dying from a drug-related overdose in 2015; 85% of these deaths involved opioids. 9
These disturbing trends highlight the need to develop and disseminate prescription OM prevention strategies that are easily accessible to and effectively engage and educate adolescents on the risks associated with PDM, particularly OM.
Although it is typically recommended that prevention strategies target all drugs, 10 the epidemiology of PDM has important differences from illicit drug abuse among adolescents. For instance, a high proportion of adolescents perceive that prescription medications are safe, even when used for nonmedical reasons. 11 Motivations to use PDs range widely and include self-medication (e.g., for pain, anxiety, and weight loss),12,13 getting high, performance enhancement, and experimentation. 14
Unlike those who abuse illicit drugs, adolescents using PDs for nonmedical reasons are more likely to be female13,15,16 and to obtain PDs from a friend or relative.17,18 Adolescents also report that their parents do not talk to them about the risks of PDs as much as they do about other substances of abuse and that, unlike other drugs, there are situations when parents think it is okay to give their children a PD that was not prescribed for them. 19
Several effective universal substance-use prevention approaches exist for adolescents20,21; however, they typically do not cover aspects of PDM that are unique to these classes of agents (see prior paragraph),12,17,18 particularly opioids, for which self-medication for pain is a common motivation for OM.12,13 Although at least one PDM-specific program does exist for high school students, 22 its efficacy is unclear. Furthermore, no intervention programs that specifically target PDM/OM among middle school students are generally available, to our knowledge, even though PDM is present among this age group.2,23
Given the evidence that younger age of PDM initiation is associated with increased risk of PD use disorder, 5 brief interventions can be effective when targeting a specific issue,24–27 and the epidemiology of PDM is unique; the development of PDM interventions that are developmentally appropriate for age groups younger than high school students and incorporate innovative strategies to enhance the efficiency, accessibility, and consistency of delivery is vital.
Gamification is the application of game design elements into existing processes and services to engage and motivate players while simultaneously attempting to modify some aspects of their health behavior. 28 It incorporates game design techniques, game thinking, and game mechanics in nongame contexts, such as social situations, to promote attitude and behavior change. 29 Given that 95% of adolescents aged 13–17 have access to a smartphone, 45% use the internet almost constantly, 88% have computer access at home, 90% play computer, web, portable (e.g., cell phone), or console games, 30 and adolescent boys and girls play videogames on an average of ∼120 and 40 min/day, respectively, 31 game-based technology and communication patterns are having a major impact on the way in which risk and protective health-related behaviors are learned and perceived by adolescents.
Research suggests that games may motivate and engage targeted audiences32,33 by providing feelings of competence, mastery, being in control, achievement, autonomy, choice, and relatedness to others. 34 Electronic games are increasingly recognized as having promise to improve health outcomes 35 as well as potentially being more efficacious and the preferred delivery method to reach today's adolescents. 29 Furthermore, gamification increases the fidelity of prevention delivery by ensuring that prevention content is delivered in a consistent and unbiased manner to all adolescents. Thus, this pilot project aimed to develop “SafeUse,” a game-based intervention to prevent adolescent prescription OM, and evaluate its initial acceptability, relatability, and preliminary effectiveness among adolescents.
Materials and Methods
Stage 1: development of SafeUse
Conceptual frameworks
Two stylistically consistent and easily integrated theoretical frameworks guide the development of SafeUse. Social Cognitive Theory (SCT), developed from Social Learning Theory, serves as the overarching explanatory framework for understanding how to prevent adolescent OM.36–38 SCT proposes that individuals do not simply respond to environmental influences but rather actively seek and interpret information 39 ; behavior is viewed as a dynamic reciprocal interaction among the characteristics of a person, the behavior of that person, and the environment in which a behavior is performed. Behavior is influenced by outcome expectations that are acquired through direct experience, vicarious experiences, judgments by others, inferred knowledge from what is already known, and perceived competence to perform the behavior needed to influence outcomes. Behavior is also regulated by its consequences, but only as those consequences interpreted and understood by the individual.
According to the SCT, members of adolescent social networks (e.g., parents, friends, other peers, teachers, and counselors) serve as role models for adolescents and affect expectancies, evaluations, and self-efficacy related to OM. If adolescents see role models misuse opioids or other PDs with positive consequences, they are more likely to develop positive expectations of OM, which increases the likelihood that the adolescent will misuse such drugs. 40 Learning to avoid OM occurs in a similar manner when adolescents who observe negative consequences of misuse expect negative outcomes and are less likely to engage in OM. Self-efficacy to obtain and use or, alternately, to refuse substance use, may also be learned by observing a model and is key to behavior change.
Thus, SafeUse was designed to allow adolescents to engage in social scenarios related to OM and actively construct their own meaning of the new information by relating it to their experiences, attitudes, and beliefs in a safe learning environment that promotes self-exploration and self-evaluation.
The Information-Motivation-Behavioral Skills (IMB) model, which combines the theoretical constructs of the Health Belief Model, Self-Efficacy Model, and the Theory of Planned Behavior, provides the framework to examine causal mechanisms of behavior change.41,42 The IMB model posits three primary constructs needed to engage in a given health behavior: information (knowledge of preventive behavior); motivation (attitudes toward performing behavior); and behavioral skills (to successfully perform the behavior). Information and motivation interact to activate behavioral skills (e.g., self-efficacy) and, ultimately, enact prevention and risk reduction behaviors.
SafeUse provides information directly relevant to OM, an initial prerequisite of risk behavior changes, in the first scenario (i.e., school assembly on OM) and throughout the game-based intervention (e.g., fun facts and myth busters). SafeUse is designed to motivate adolescents to engage in preventive behaviors by allowing/encouraging them to experience a myriad of outcomes related to OM (or not), evaluate their attitudes toward the performance of OM preventive acts, and the influence of social norms regarding their performance of such acts, and to increase the awareness of their personal vulnerability for OM. Behavioral skills for performing specific OM preventive acts (e.g., opioid refusal skills, accepting but not ingesting opioid, and talking with parents or school counselor) are modeled throughout SafeUse (as are consequences of not performing such) to instill and reinforce self-efficacy and, subsequently, encourage OM preventive behaviors.
Approach
SafeUse is a branching narrative game with weighted randomized outcomes. The prototype takes 3–4 hours to play through all possible content and endings. The majority of gameplay consists of players responding to contextual dialogue choices offered in the fictitious social world of a teenager. These dialogue choices exist in 3D-modeled scenes with a single camera point of view, representing the player's embodied presence in the scene (Fig. 1A, B). Dialogue is also shown through a phone text interface (Fig. 1C). This model of gameplay is represented widely in contemporary videogames.
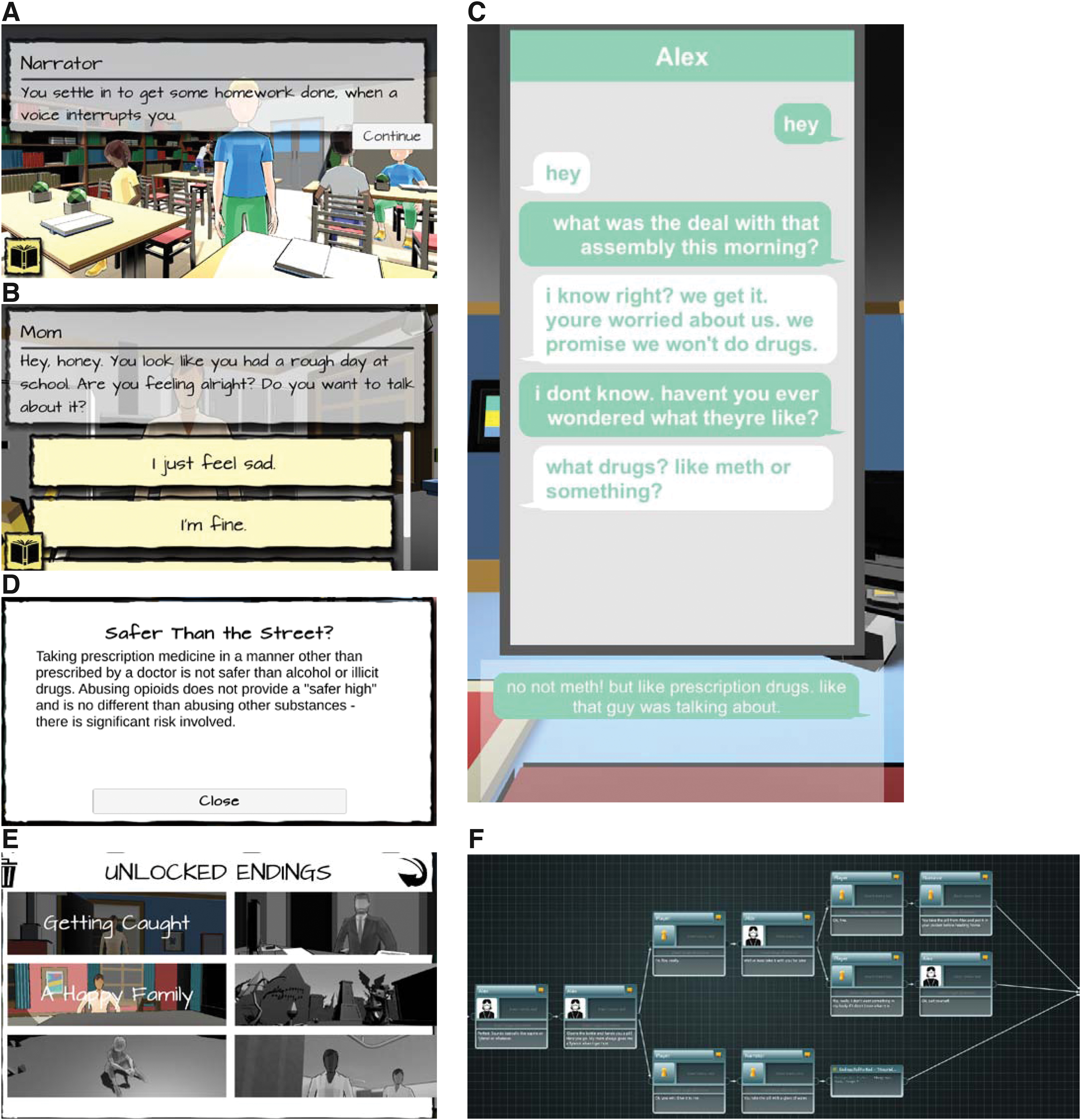
Examples of screenshots of the game and game flow with player choice points:
The specific subgenre used in SafeUse is the “visual novel” game. 43 Using this style, SafeUse incorporates three key elements of game-based engagement: narrative engagement, meaningful choice, and random reinforcement, along with several other secondary elements common to generalized videogame play (Table 1). The game also includes two mechanics that straddle the education/play boundary: fact cards (Fig. 1D) that are triggered by specific events in the narrative, and unlockable endings (Fig. 1E) that allow replay of the game to unlock multiple health outcomes.
A Brief Overview of Major Design Concepts (and Key Sources That Analyze Them) That Were Used to Inform Game Elements in SafeUse
The development process for the game began with drafting of a branching script, created in the specialized scripting software Articy Draft. 44 This software is designed for writing branching narrative using a visual editor (Fig. 1F), which allows writers to access various scenes and dialogues quickly, while still affording an overview of the entire branching story. Once the interactive script was drafted, it went through several rounds of revisions, as the research team offered suggestions to game designers about the medical, social, emotional, and behavioral content of the scenes. The research team also helped categorize the various story threads in the game to balance the number and variety of situations that might precipitate OM. Evidence-based materials regarding prescription OM from the BeMedWise website (e.g., https://www.bemedwise.org/prevent-kid-drug-abuse/, https://www.bemedwise.org/prevent-prescription-medicine-abuse-toolkits/not-worth-the-risk-even-if-its-legal/, etc.) and the National Institute on Drug Abuse45,46 were incorporated during this process.
Once the script was finalized, the game design team constructed 3D-modeled scenes and recorded sound effects and voiceover lines with professional actors to increase the emotional engagement of the experience. The game designers also added game logic to many of the scenes, adding random weighted chances for particular outcomes. This was particularly useful for offering specific chances of overdose, and increasing those chances with each playthrough, so that at some point players are guaranteed to experience one of the “overdose endings” the game includes. The designers also built a user interface (UI) for the game, specifically for use on iOS and Android phones. Once the prototype was complete, it was tested internally, and ongoingly adapted, fixing bugs that arose for users during the pilot study.
All stages of SafeUse's design, from content development and script writing to game and UI design, were based on a collaborative process of exploration between game designers and the research team using agile development procedures.47,48 Game design elements were applied to the educational content and storylines to engage and motivate players while simultaneously attempting to promote attitude and health behavior change.28,29
Stage 2: initial evaluation of SafeUse acceptability and applicability
Overview
A mixed-methods study was conducted to examine the acceptability and applicability of SafeUse among adolescents in the 8th and 11th grades. These grades were targeted with the intent to uncover any potential developmental differences in the game's acceptability and relatedness. Following consent/assent procedures with the adolescents and their parent/caregiver, adolescent participants completed assessments before playing SafeUse; completed postintervention assessments 5–7 days afterward; and participated in a semistructured focus group to provide feedback on SafeUse design (e.g., ease of use, level of engagement, and knowledge transfer). The University of Arkansas Institutional Review Board approved this study protocol under expedited procedures under category 7.
Approach
Adolescents were initially recruited via e-mail announcements and flyers to 8th and 11th grade students from a superintendent-selected middle and high school in central Arkansas; however, due to lower than anticipated response rates, students were also recruited from around the state via advertisements on social media and flyer distribution. To be included in the study, adolescents were required to be enrolled in the 8th or 11th grade; identify as female or male gender; and have access to a smartphone with headphones. Parents were asked to call a recruitment line and a member of the research team discussed the study with them and their child. If they and their child were interested in participating, they were given a link to access the consent/assent forms in REDCap and the research staff member performed informed consent and assent over the telephone.
Once consent and assent forms were electronically signed, printouts of the signed forms were mailed to the participant's home. Typically, once at least two to five students in a particular grade signed informed consent, focus groups were scheduled. About 5–7 days before the scheduled session, participants completed the preassessment forms and were instructed to download the SafeUse from the app store and interact with the game for about 1 h/day. Twenty-five participants signed informed consent, of which 10 (mostly 11th graders) did not enter the study due to school workload and/or extracurricular activities (Fig. 3). One participant did not show up to the scheduled focus group session and was lost to follow-up.
Semistructured focus groups (Fig. 2) were facilitated with a sample of 14 adolescents (aged 13–17 years; eleven 8th graders and three 11th graders) to receive feedback on the design and development of SafeUse, including whether it is usable, engaging, and effective. Before and following access to SafeUse, adolescents completed a questionnaire about their perceptions about opioids. They also completed a postaccess questionnaire about their demographics and experience with the game. Qualitative data obtained during the focus groups explored the norms, phenomenological life-worlds (i.e., the world as immediately or directly experienced in the subjectivity of everyday life) and experiences of adolescents at each grade level determined the actual range of behaviors and ideas that were valid indicators of feasibility. 49

Subject flow during the course of the study. FG, focus group.
Focus group questions centered on adolescents' context-specific experiences, risk behaviors, normative pressures, and barriers related to opioid use and gaming. Specific questions included the following: “Do you think you would play SafeUse (or a game like it), why? Tell me more”; “What do you think about the current name of the game: Safe Use? What do you like or not like about it? What would you call it?” “What do you think we need to consider when further developing Safe Use?” “How effective do you think SafeUse would be if made available for students, why?” “What would motivate you to continue playing Safe Use, if it were made available?” “What would discourage you from playing SafeUse, if it were made available?” “What specific recommendations do you have for further developing SafeUse, in terms of instructions, opening graphics, choice of scenarios, types of decisions offered; number of decisions offered; realistic outcomes of use; adequate information provided; and playability?” “Is there anything else about what we have discussed that you would like to add?”
Focus groups were segmented by grade, 50 lasted 1–1.5 hours and initially conducted in-person at a time convenient for adolescents and their parents; however, due to the rise of COVID-19, focus groups were shifted to a virtual format using the Zoom platform. Parents were not present in focus groups to enhance adolescent willingness to share personal experiences. Before participating in the focus group, adolescents signed a confidentiality agreement stating that they pledged to maintain the confidential nature of the group.
For in-person focus groups, adolescents were gathered in a conference room to start the focus group session after a quick snack. If focus groups were conducted via Zoom, study staff instructed participants to ensure they were in a private space behind a closed door where the conversations could not be overheard (as was the case for study staff). For both Zoom and in-person groups, the recorder was turned on and participants were asked a series of questions regarding the intervention (see second paragraph above, starting “Focus group questions”). At the end of the focus group, participants were given or mailed (for those participating virtual groups) $50 gift cards for their time. Two in-person focus groups were held at the University of Arkansas for Medical Sciences and three virtual focus groups were conducted online.
Focus groups were digitally recorded, deidentified, and transcribed. Conventional content analyses were conducted to create preliminary themes by which to sort adolescent quotes. 51 A preliminary codebook consisting of top and sublevel codes were developed after reading one to two transcripts. 52 The first transcript was independently coded by all members of the study team and results were compared to define and refine the codebook as well as ensure inter-rater reliability.
Two coders independently coded the remaining transcripts to enhance rigor in analysis, and findings were discussed to determine the final themes. The rigorous and accelerated data reduction (RADaR) technique was used 53 to code and summarize focus group feedback under five major domains (playability, acceptability, appropriateness, content development, and knowledge transfer). These terms and definitions for program fit were obtained from the California Evidenced-Based Clearinghouse (CEBC) for Child Welfare website (https://www.cebc4cw.org) and Weiner et al. 54 Additional game-related terms and definitions (e.g., for screenplay/scenarios, technical/knowledge transmission, gameplay/playability, music and sound) were selected from Ak. 55
Pre-and post-access questionnaires were designed to measure adolescent knowledge and perceptions about prescription opioid use and misuse, including legality, safety, and side effects. Adolescents indicated the degree to which they agreed with each statement on a 6-point scale from strongly agree to strongly disagree. The post-access questionnaire included visual analog questions about SafeUse rated on a scale from 0 (not at all) to 10 (extremely), including the degree to which the adolescent understood the material; liked the game; learned something new about prescription pain killers; was likely to refuse an opioid if offered; was confident in being able to refuse a prescription pain killer if offered; and would like to play another module of the game.
Descriptive statistics were used to describe subject characteristics. Selected data from the postaccess questionnaire were graphed to show distribution of feedback regarding SafeUse. Data for each continuous measure from the pre- and postaccess questionnaires were entered into Wilcoxon matched pairs signed-rank tests and means and standard deviations were calculated. For all analyses, a P-value of ≤0.05 was used to infer statistical significance.
Results
Participants were 14.1 ± 1.1 years on average, 57.1% female, 57.1% white, 35.7% black, 7.1% Asian, and 14.2% Hispanic. Adolescents reported being an A or A/B (64.3%), B or B/C (14.3%), or C (21.4%) student. About 71% of participants reported having experience playing electronic games, including smartphones (50%), computers (21.4%), and/or televisions (42.9%).
Participants reported playing SafeUse for 4.7 ± 0.9 days and 42.7 ± 20.6 min/day on average. They also reported unlocking a mean of 3.0 ± 1.71 out of six endings. The two endings with the lowest completion rate (21.4% of participants) were (i) attending the funeral of a friend who died of an opioid overdose and (ii) dying from an opioid overdose. Otherwise, more than half of the participants completed the other four endings (57.1%–71.4%). After access to SafeUse, adolescents reported that they moderately to extremely “liked the game,” “would like to play more game modules,” “liked playing through the decisions,” thought the game was realistic/relevant, that the game was fun, and they learned new information about opioids (Fig. 3). Adolescents showed high levels of agreement that the material increased confidence to refuse opioids and low likelihood of taking an opioid from someone they knew. They did report low to moderate agreement that the game was boring (Fig. 3).
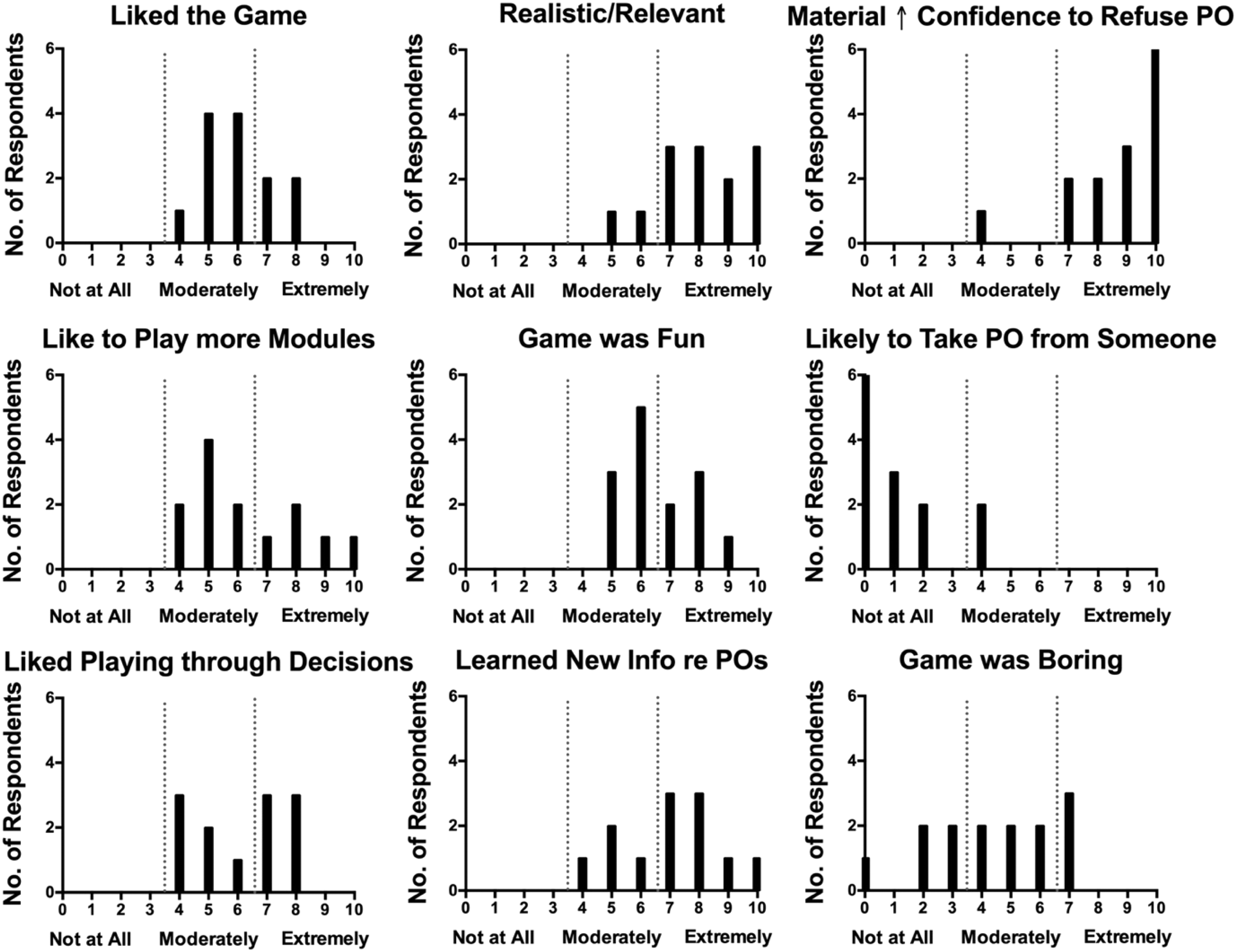
Degree of respondent agreement with selected statements on the post-SafeUse access questionnaire on a scale from not at all (0) to extremely (10). The number of respondents is plotted as a function of score.
A summary of focus group feedback is shown in Table 2. Adolescents generally liked SafeUse, its characters, graphics, and approach. They stated that the game was a more appealing way to learn than lectures/reading materials and that they learned a lot. They also reported technical glitches they would like addressed. They saw SafeUse as appropriate for school settings, but not having mass appeal, and suggested a wider targeted age range, inclusion of other substances, and plainer language. Many suggestions for building out content, including relevant scenarios and additional information regarding fun facts, resources, and longer term effects of OM, were also provided.
Summary of Focus Group Feedback Among Students Across Five Major Domains: Playability, Acceptability, Appropriateness, Content Development, and Knowledge Transfer
Before access to SafeUse, respondents indicated strong agreement about being knowledgeable about opioids, their dangers, and physical effects, and comfortable refusing opioids if offered (Table 3). The extent to which participants agreed that they were knowledgeable about opioids significantly increased and that PDs are safer than illegal drugs significantly decreased after access to SafeUse. In contrast, their knowledge about Narcan or overdoses showed minimal, if any, changes.
Summary of Responses to General Knowledge About Opioids Before (Pre) and After (Post) Access to the Gamified Intervention
Bold indicates a statistically significant change.
Participants rated the degree to which they agreed with each question on a scale of 1 (strongly agree) to 6 (strongly disagree).
Mean (standard deviation of the sample).
Wilcoxon matched pairs signed-rank test statistic.
Discussion
This article describes the development of SafeUse, a new game-based prescription opioid prevention intervention for adolescents. The methods used to develop this intervention were to (i) incorporate evidence-based materials into the creation of SafeUse, using standard development processes, allowing players to experience the consequences of different choices regarding prescription opioid use, learn the facts that dispel myths about PDs, and offer examples of how to easily refuse drugs when offered; and (ii) to obtain stakeholder feedback on its initial acceptability through a mixed-methods study.
SafeUse was generally acceptable to participants, with postaccess questionnaires and/or focus group feedback indicating that the game was fun to play, was educational, and increased confidence in refusal skills. Although the approach, design, and graphics were also liked as a rule, there was moderate agreement that the game was boring. However, this seemed tied mainly to technical glitches that created redundancies, not allowing participants to complete certain endings, and the inflexibility in having to repeat certain parts of the game multiple times. At the same time, adolescents did generally report that they were unlikely to play the game if accessible outside of the school setting, suggesting that the game would not have mass appeal outside the school setting in its present form.
Participants did offer many suggestions for improving the game (Table 2), such as targeting a wider age range (potentially with different developmentally appropriate levels of the game), inclusion of other substances beyond just opioids, having more flexibility in skipping parts that they had already experienced, more user controls, and plainer language. Many suggestions for building out content were also provided. For instance, participants suggested adding other scenarios, including being at a party, socializing with friends on school grounds outside the building, more social media interactions, having a family member with a drug problem, physical abuse in the home, watching the drug effects experienced by another user, and adding a father (not just mother) character.
Participants wanted to see additional information regarding “fun facts,” resources, and longer term effects. They also suggested having more minigames within scenarios to engage and entertain players and some sort of incentive (e.g., points, grade, and credit) to motivate players. These suggestions are quite feasible and likely would enhance the effectiveness of SafeUse in preventing PDM.
The few studies that have assessed the fidelity of school-based drug prevention programs implemented by teachers under real-world conditions have revealed that there is a noticeable deficit in the fidelity of program delivery that is achieved. 56 Rigorous field trials of drug abuse prevention curricula have been done where considerable effort is made to get teachers and others to deliver the curriculum exactly as intended. However, even under these circumstances, there is tremendous variability in how consistently various teachers present program material.56,57 Thus, SafeUse would likely be appropriate and effective for delivery with high fidelity in school settings.
Interestingly, before accessing the game, participants already appeared to perceive a strong knowledge of opioids, but this perception still significantly increased after access to the game. In addition, the perception that prescription opioids are relatively safe compared with illegal substances significantly decreased after game access. This, along with postgame ratings showing increased confidence to refuse drugs if offered as well as low likelihood of taking PDs from someone if offered, suggests that the game may have some initial efficacy to enhance certain protective factors and reduce particular risk factors. Meanwhile, the lack of change in knowledge about opioid overdoses may be due to the fact that, because of technical glitches that were not caught initially, many adolescents could not access the overdose scenario and so did not access the material on this topic.
Thus, whether the material enhances adolescent understanding of opioid overdoses is unclear at this time. Otherwise, ratings generally shifted in the desired direction after game access, even though the changes were not statistically significant, suggesting that this approach may be effective in altering knowledge and attitudes about OM.
Several limitations of the study need to be noted. First, although the prototype was developed by content experts and game developers experienced in producing serious games, students and other stakeholders did not provide initial input into the game. Reasons for not involving stakeholders in initial decision-making included a very limited amount of pilot funds, a 1-year duration of award, the expertise of collaborators, including child and adolescent psychiatrists, the intended focus on opioids with an already available evidence base to draw from, and the desire to produce a prototype with which students could provide feedback. That some participants likened the prototype to the “Oregon Trail” (see Charsky and Barbour 58 ) educational game suggests that our approach was built on similar proven successful designs.
Second, although our intention was to examine potential developmental differences between 8th and 11th graders, we were unable to recruit and retain enough 11th grade participants to make formal comparisons of their feedback with that of the 8th graders. Third, our sample size of 14 overall was small. Thus, whether the lack of significant differences in pre- and postgame access scores was due to the lack of power or due to the lack of efficacy is unclear. Fourth, players nevertheless, the findings of this study overall suggest that further development and evaluation of this prototype are warranted.
Future plans include obtaining stakeholder (parent and school staff) feedback on proposed changes to the game based the findings of this study, findings from a subsequent usability evaluation of the revised game among middle school students (6th–8th grade), and optimal strategies for evaluating the efficacy of this product in school settings, all in preparation for a school-based prevention trial of SafeUse. Ultimately, this intervention has the potential to fill a developmental gap in PD prevention efforts that could help delay and/or reduce PDM and the subsequent development of substance-use disorder among middle school students.
Conclusions
SafeUse is acceptable and likely educational to adolescents and has the potential to reduce risk and strengthen protective factors related to OM, thus warranting further research and development.
Declarations
A preliminary report of this work was presented virtually at the Annual Meeting of the College on Problems of Drug Dependence on June 23, 2020.
Ethical Approval
This study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards and approved by the University of Arkansas for Medical Sciences Institutional Review Board under expedited procedures (11/08/2018; IRB#228817).
Consent to Participate
Freely given informed consent and assent to participate in the study were obtained from all parents and adolescent participants and a statement to this effect appears in the article.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the University of Arkansas for Medical Sciences Translational Research Institute, grant number UL1 TR003107, through the National Center for Advancing Translational Sciences of the National Institutes of Health.