
Abstract
It is unclear whether virtual reality (VR)-based exercise can improve physical fitness in people with intellectual disability (ID). This systematic review therefore aimed to synthesize existing evidence regarding the efficacy of VR-based exercise on physical fitness in people with ID. Eligible articles were searched through six major electronic databases from inception until August 15, 2022. Returned studies were screened through predefined inclusion and exclusion criteria. Data from the included studies were then extracted and synthesized. A total of 13 randomized controlled trials were included and 12 of them were found to have good research quality. Different physical fitness outcomes were evaluated: (1) muscular fitness (d = 0.05–2.12; proportion of effect = 5/6), (2) cardiorespiratory fitness (d = 0.12–0.67; proportion of effect = 5/5), (3) flexibility (d = 0.81; proportion of effect = 1/2), (4) body composition (d = 0.10; proportion of effect = 2/3), (5) balance (d = 0.23–1.65; proportion of effect = 6/7), (6) coordination (d = 0.19–0.48; proportion of effect = 2/3), (7) speed and agility (d = 0.13–0.46; proportion of effect = 4/4), and (8) overall motor proficiency (d = 0.02–1.08; proportion of effect = 1/3). While there was some preliminary evidence showing that VR-based exercise could improve muscular fitness, cardiorespiratory fitness, balance, and speed and agility in individuals with ID, other outcomes showed less conclusive or limited positive evidence. Overall, additional studies are needed to understand the benefits of VR-based exercise on physical fitness in people with ID.
Introduction
Intellectual disability (ID) is one of the most common neurodevelopmental disabilities worldwide, with an incidence of 2%–3% of the general population.1,2 People with ID are characterized as with limited intellectual quotients and impaired adaptive behaviors. 3 An important health-related issue for this population is their low levels of physical fitness. 4
Physical fitness refers to one's ability to perform physical activity. 5 Physical fitness includes health-related fitness (HRF) such as body composition and muscular strength, and skill-related fitness (SRF) such as agility and balance. 6 Several studies have shown that 71%–91% of people with ID fail to meet the standards of cardiorespiratory fitness and muscular fitness, 7 and have lower levels of physical fitness than those without ID. 8 The lower fitness levels of people with ID may contribute to higher rates of cardiovascular disease, obesity, and other related problems.9–11 Data have indicated that nearly one-third of people with ID suffer from hypertension and obesity, and they are 1.54–1.80 times more likely to have these problems than those without ID.12–15
Participation in physical activity is critical for the improvement and maintenance of cardiovascular fitness, bone health, healthy body weight, and psychological well-being for people with ID.8,16–18 However, people with ID often exhibit low levels of physical activity. 4 Research shows that only 27% of people with ID can maintain regular, consistent physical activity. 19 This low physical activity participation level could be attributed to major barriers such as limited access to facilities and venues, bullying from others, financial constraints, poor motor coordination, gait abnormalities, and low exercise compliance.20–23
Virtual reality (VR)-based exercise or videogaming such as Nintendo Wii Fit and Wii Sports seems to be a feasible approach for increasing physical activity and physical fitness levels in people with ID. 24 This kind of exercise provides full-body physical activity through videogames that require a gross motor and visuospatial coordination, balance, and energy expenditure, which is comparable with moderate-intensity physical activity.25–27 VR-based exercise is affordable, easy to carry out, enjoyable, motivating, and highly adherent for people with ID.25,27–31 VR-based exercise is not limited by space or venue as participants can achieve the recommended aerobic exercise intensity and energy expenditure by practicing the exercise at home.32,33 This seems to address some of the aforementioned barriers to physical activity participation (e.g., limited access to exercise venues and low exercise compliance) and to increase physical fitness in people with ID.
Several studies have documented that VR-based exercise has the potential to improve motor ability, physical function, and cognition in children with neurological disorders such as autism spectrum disorder, Parkinson's disease, and cerebral palsy.34,35 Taken together, VR-based exercise may improve physical fitness in people with ID.
Two recent reviews examined the effectiveness of VR-based exercise on physical fitness in people with ID. Suarez-Iglesias et al 36 reported that VR-based exercise could improve physical health in this group. However, this study focused on examining a wide range of outcomes (e.g., cognitive function, mental and physical health) and only a few physical fitness elements were examined in their study. In other words, their study was not specifically conducted to examine the efficacy of VR-based exercise on physical fitness. Stander et al 37 concluded that there was some preliminary evidence showing that VR-based exercise could improve agility, strength and balance, and coordination in children with Down syndrome. Their study group was limited to the children with Down syndrome and only four quasi-experimental studies were included. Thus, it would be difficult to generalize their findings to the whole ID group and the validity is also limited.
As an extension to these two aforementioned reviews, the present study therefore aimed to systematically summarize randomized controlled trials (RCTs) that examine the effects of VR-based exercise on different types of HRF and SRF in individuals with ID. Findings of this review can guide future research and provide evidence for the development of VR-based exercise programs for individuals with ID.
Materials and Methods
This systematic review was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement and was registered in the PROSPERO database (CRD42022323533). 38
Eligibility criteria
Studies were included if they met the following criteria: (1) participants were with ID; (2) studies that used VR-based exercise as the primary intervention, such as Nintendo Wii or SeeMe Games system; (3) the comparison group received either non-VR-based exercise intervention or no treatment; (4) the outcome should include at least one HRF (e.g., body composition, muscular strength) or SRF (e.g., agility, balance); and (5) peer-reviewed studies reporting results from RCTs that examined the effects of VR-based exercise on at least one physical fitness outcome in participants with ID. Studies were excluded if: (1) their participants were without ID; (2) they did not provide outcomes of physical fitness; (3) they were not written in English; (4) they were not an RCT; or (5) they were conference abstracts, case reports, or reviews. 39
Search strategy
Six electronic databases including Embase, PubMed, Web of Science (all collections), Cochrane library, SPORTDiscus, and Scopus were systematically searched from inception to January 20, 2022. An updated search was conducted on August 15, 2022. Three groups of search terms were used for the search: (1) “intellectual disability*,” “ID,” “mental retardation,” “Down syndrome,” “autism” or “developmental disabilit*”; (2) “virtual reality,” “VR,” “virtual environment*,” “Nintendo Wii,” “Wii,” “video gam*,” “exergame*,” or “computer gam*”; and (3) “physical fitness,” “cardiorespiratory fitness,” “muscular strength,” “muscular endurance,” “body composition,” “flexibility,” “agility,” “balance,” “speed” or “coordination.” In addition, the reference lists of all eligible studies were reviewed to identify potentially eligible studies (Table S1).
Selection process
Search returns were exported to Endnote X9. Duplicate articles were removed, and obviously, irrelevant studies were identified and excluded through reading titles and abstracts. Full-texts were consulted to select the potentially relevant studies further. The screening processes were independently conducted by two reviewers (X.L., J.H.). If an agreement could not be reached, it was resolved through discussion with a third researcher (C.L.).
Data collection process and data items
Extracted data included the following information: first author, year of publication, participant characteristics (sample size, gender, mean age/age range, level of ID), interventions (type of VR, time, frequency, duration, intensity), outcomes, and related measures. Two researchers (X.L., J.H.) independently extracted the aforementioned information. Disagreements were resolved through consultation with a third researcher (C.L.).
Study risk-of-bias assessment
The Cochrane Risk-of-Bias Tool was used to evaluate the included studies for the risk of bias. 39 Two reviewers (X.L., J.H.) independently assessed the following domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other biases. The risk of bias of each domain was rated as low, high, or unclear (i.e., lack of information or uncertainty). Disagreements were resolved through consultation with a third researcher (C.L.). The finalized assessment results were tabulated using RevMan5.3 to generate the risk-of-bias graphs.
Results
Study selection
An initial search of the databases revealed a total of 1000 records, and 462 duplicate records were removed. From reviewing the titles and abstracts of the remaining 538 articles, 412 articles were excluded. The full texts of the remaining 126 articles were downloaded for detailed assessment. Ultimately, 13 studies were included in the present review (Fig. 1).
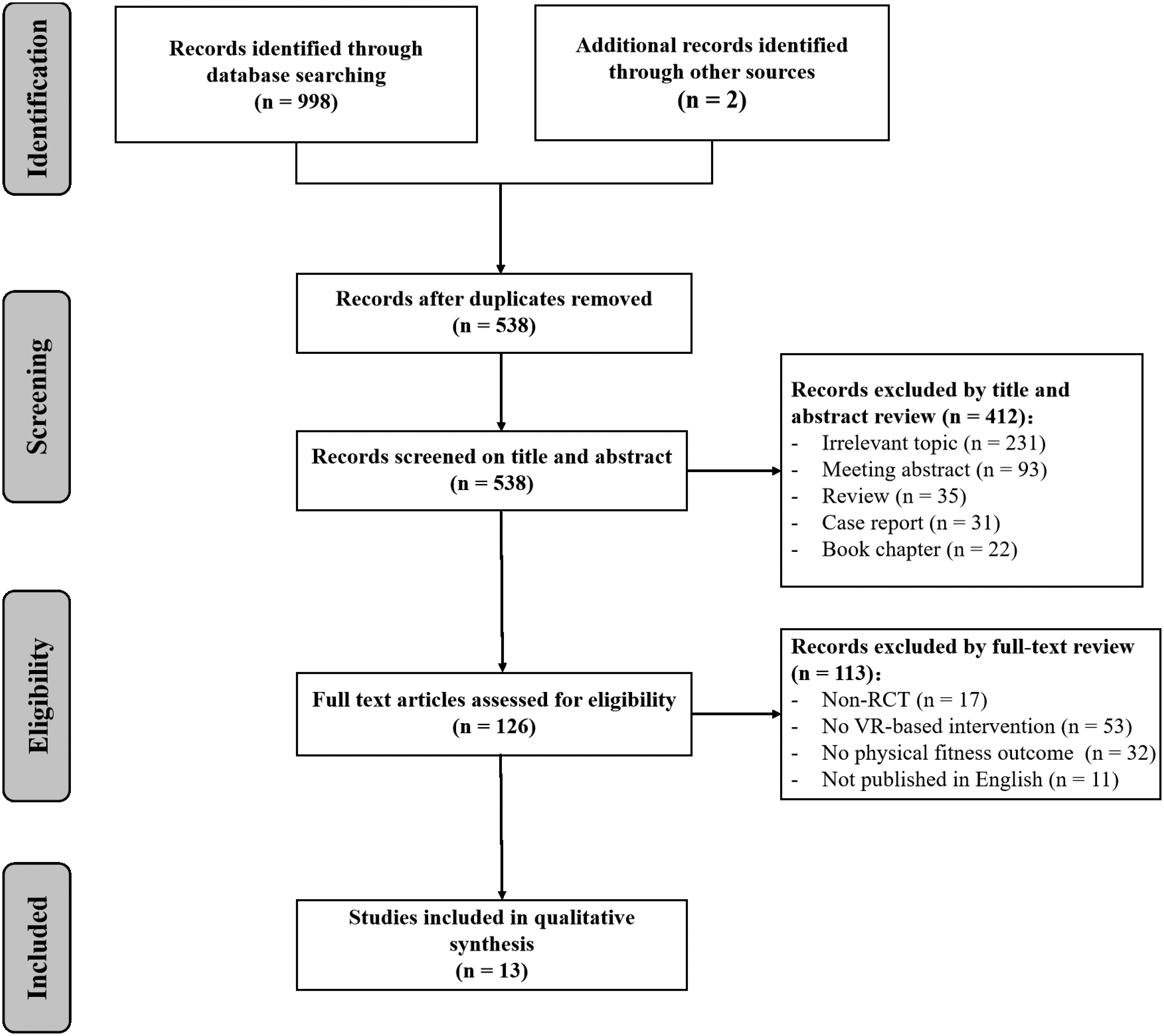
Flowchart of the selection process.
Study characteristics
Participant characteristics
The 13 included studies (RCTs) enrolled a total of 803 participants with ID (Table 1). The sample size of these studies ranged from 12 to 203. There were more male participants than females (male = 354, female = 217) across the eight studies that reported participants' gender. The participants' ages ranged from 5 to 77. Eight studies involved children and adolescents,31,40–46 and five studies included adults.27,47–50 Eight studies reported participants' severity levels of ID, which ranged from mild to severe.40,43–49
Study Characteristics of Included Studies (n = 13)
CG, control group; EG, experimental group; F, female; HRR, heart rate reserve; ID, intellectual disability; M, male; METs, methionines; MHR, maximum heart rate; NR, not reported; SD, standard deviation; SOT, standard occupational therapy; VR, virtual reality.
Intervention characteristics
Regarding the use of VR platform for exercise intervention, eight studies used Nintendo Wii such as Wii Sports, Wii Fit, and Wii software Mario.27,31,40,41,43,45,46,50 In addition to the exclusive use of VR-based exercise intervention, two studies combined VR-based exercise with either treadmill training or traditional therapy.45,46
While most studies (n = 9) used a blank control group, two studies used physical education,40,43 one study used standard occupational theory, 31 and one study used traditional physical therapy as an active control group. 46 The duration of the intervention program ranged from 4 weeks to 1 year. The weekly intervention frequency was between two and four times, and most studies offered two times (n = 7). The training duration for each session was between 15 and 60 minutes (Table 1). Only three studies reported the training intensity and all of them used a moderate intensity.44,45,50
Risk of bias
All the included studies were rated as having an unclear risk of bias for the allocation concealment, blinding of participants and personnel, incomplete outcome data, and free selective reporting. Only two studies reported adequate sequence generation.31,47 Five studies were rated with a low risk of bias that reported using blinded outcome assessors.27,31,44,47,49 Finally, a high risk of other biases, significant differences at baseline, was identified in a study. 44 In addition, an unclear risk of other biases was rated in another study (Fig. 2). 49

Risk of bias in included studies. Color images are available online.
Effects of VR-based exercise on physical fitness
Various physical fitness measures were used across the 13 included studies, and the Bruininks–Oseretsky test of motor proficiency was the most popular one (n = 3). Nine studies analyzed the effects of VR-based exercise on HRF outcomes. Meanwhile, 10 studies reported SRF outcomes. To quantify the intervention effects, effect sizes (Cohen's d) were calculated to determine the standardized mean difference between the two groups at posttest:
Results Reported for Outcomes of Included Studies (n = 13)
P < 0.05; bP < 0.01.
BMI, body mass index; BOT-2, Bruininks–Oseretsky Test of Motor Proficiency-Second Edition; BOTMP, Bruininks–Oseretsky Test of Motor Proficiency; KTK, Korperkoordinationstest fur Kinder; NA, not available; PBS, Pediatric Balance Scale; TGMD-2, Test of Gross Motor Development-Second Edition; TUG, Timed Up and Go Test.
Health-related fitness
Three studies assessed the effect of VR-based exercise on body composition,27,40,44 and two of which reported a significant treatment effect on body weight favoring the VR-based exercise group (d = 0.10/not available [NA]; proportion of effect = 2/3).27,40
Six studies examined the intervention effects on muscular strength and/or endurance.27,31,40,43,45,50 They generally reported significant improvements in the VR-based exercise group over the control group (d = 0.05–2.12; proportion of effect = 5/6).27,31,40,43,50 However, Silva et al 27 reported no significant between-group difference in muscular endurance as measured by the bent arm hang test (d = 0.54). Of note, Hsu 43 reported that the VR-based exercise group outperformed the sedentary activity group, but not the physical education group on muscular strength (d = NA). Furthermore, Wuang et al 31 reported that the VR-based exercise group outperformed both the standard occupational therapy group and blank control group on muscular strength and endurance (d = 0.10–0.37).
Five studies reported that VR-based exercise effectively improved cardiorespiratory fitness compared with the control groups (d = 0.12–0.67; proportion of effect = 5/5).27,40,48–50 Of note, Lotan et al 48 displayed no significant improvement in cardiorespiratory fitness used the Total Heart Beat Index (d = 0.01), while there was a significant improvement used the Energy Expenditure Index (d = 0.12). Lotan et al 49 described no significant improvement in cardiorespiratory fitness utilizing the change pulse at rest test (d = 0.09).
Two studies examined flexibility outcomes. One study reported that the VR-based exercise significantly improved flexibility (d = 0.81; proportion of effect = 1/2). 27 Another study reported that the VR-based exercise group did not significantly improve flexibility (d = NA). 40
Skill-related fitness
Seven studies evaluated the effects of VR-based exercise on balance.27,31,42,43,46,47,50 Except for the study by Lotan and Weiss 47 that reported a nonsignificant improvement (d = 0.59), other studies revealed a significant improvement on balance favoring VR-based exercise groups (d = 0.23–1.65; proportion of effect = 6/7). It is worthy to note that Silva et al 27 displayed no significant improvement in balance as measured by the Flamingo Balance Test (d = 0.84), while a significant improvement was detected through the Time Up and Go Test (d = 0.57). Furthermore, Hsu 43 reported that the VR-based exercise group outperformed both the physical education group and the sedentary activity group on balance (d = NA).
Three studies evaluated the coordination outcome.27,31,42 Of which, two studies reported that VR-based exercise could significantly improve coordination (d = 0.19–0.48; proportion of effect = 2/3).27,31 In particular, Wuang et al 31 indicated that the VR-based exercise group outperformed the standard occupational therapy group and blank control group on coordination (d = 0.09–0.19). However, Gouveia et al 42 found that the VR-based exercise group did not significantly improve coordination (d = 0.03).
Four studies reported that VR-based exercise significantly improved speed and agility (d = 0.13–0.46; proportion of effect = 4/4).27,31,40,45 Wuang et al 31 found that the VR-based exercise group outperformed the standard occupational therapy group and blank control group on speed and agility (d = 0.13–0.38).
Three studies measured the overall motor proficiency outcomes,27,41,44 and only one of which showed a significant improvement favoring the intervention group (d = 1.08; proportion of effect = 1/3). 41 Lau et al 44 and Silva et al 27 found that VR-based exercise did not significantly improve motor proficiency (d = 0.02–0.12).
Discussion
This is the first research, to our best knowledge, to systematically summarize RCTs that examine the effects of VR-based exercise on different types of HRF and SRF in individuals with ID. In general, the included 13 studies provided some preliminary evidence that participation in VR-based exercise could benefit several types of HRF and SRF, such as muscular fitness, cardiorespiratory fitness, and balance in people with ID.
Health-related fitness
Muscular fitness is critical to the physical health and daily life of people with ID, and muscular weakness may lead to limited mobility and gait imbalance.52–55 Six included studies reported that VR-based exercise significantly improved muscular strength and endurance of upper and lower limbs in individuals with ID.27,31,40,43,45,50 Despite poor exercise economy such as gait dynamics and kinematic disturbances in the ID population that may contribute to their ineffectiveness of lower extremity muscle training, we found that VR-based exercise led to moderate-to-large improvements in lower extremity muscular strength and endurance (d = 0.54–1.22).27,40,43 These findings suggest that VR-based exercise may be an effective way to improve the whole-body muscular fitness of people with ID.
Cardiorespiratory fitness is strongly associated with the all-cause mortality rate and quality of life among individuals with ID. 10 In the present review, five included studies generally reported that VR-based exercise significantly improved cardiorespiratory fitness in individuals with ID (d = 0.12–0.67).27,40,48–50 This finding is consistent with a recent systematic review, in which the VR-based exercise group was shown to have better cardiorespiratory fitness than the control group in children and adolescents without disabilities. 56 As we know, cardiovascular and respiratory function can be improved through regular participation in cardio training. However, traditional cardio training methods involve high training loads and significant time investments, which may thus be less appealing. As a result, traditional cardio training methods often fail to produce desirable treatment effects in cardiorespiratory fitness, 57 particularly in people with ID. 36
Compared with the traditional training methods, VR-based exercise can be completed more quickly and make similar or even more significant improvements in cardiorespiratory fitness. 45 Our findings further elucidate that VR-based exercise may be an effective way to improve cardiorespiratory fitness in individuals with ID. It is important to note that none of the included studies assessed cardiopulmonary function with the recommended golden approach, that is, maximum oxygen consumption. 58 The feasibility to use this recommended test may be low given the time and other resource constraints. In addition, individuals with severe ID may have difficulty understanding and completing the test. 49
The obesity rate of people with ID is higher than that of people without disabilities. 11 Of the three included studies that examined the body composition outcome, two showed that the use of 180 minutes of VR-based exercise per week and 45 minutes per week of VR-based exercise significantly improved body composition than the control group.27,40 The other included study reported that 60 minutes per week of VR-based exercise did not significantly improve body composition. 44 This divergence could be due to the use of different treatment doses. For example, meta-analytic research showed that 80 minutes per week of VR-based exercise is the shortest time to improve body composition in people with developmental coordination disorder. 59
Interestingly, the weekly training dose used in the study by Dickinson and Place 40 is smaller than that used by Lau et al. 44 This means, in addition to the training dose, training duration of VR-base exercise may be another factor affecting body composition (1 academic year vs. 12 weeks). Therefore, more research is warranted to explore how much and how long VR-based exercise training will be needed to improve body composition in people with ID. More research is also needed for the flexibility outcome as it was only assessed in two included studies of the present review and their findings are inconsistent.
Skill-related fitness
People with ID had a fall rate of 39%, 60 which is twice that of people without ID. 61 Indeed, adequate balance ability is an essential factor in the prevention of falls. However, many exercise training modalities such as Swiss ball exercise and walking exercise failed to improve balance in adolescents with ID. 62 Interestingly, six included studies of the present review reported that VR-based exercise positively improved the balance of people with ID (d = 0.23–1.65).27,31,42,43,46,50 This finding shows that VR-based exercise may be an effective exercise modality to improve the balance of people with ID. One possible explanation is that the VR-based exercise training is task driven and requires problem solving, which provides combined practice of balance with vision and attention direct at the exercise, and subsequently stimulating the proprioceptive-vestibular system. 63
Coordination requires sensory and motor functions to execute fast and smooth movements with accuracy. Studies have found that Tai Chi can improve the coordination of upper and lower limbs in children and adolescents with ID. 64 In line with this finding, two out of the three included studies in the present review reported that VR-based exercise improved coordination in people with ID (d = 0.19–0.48).27,31 The included study by Gouveia et al 42 did not reveal a significant improvement in coordination through VR-based exercise training. The study had a smaller sample size and a lower training dose than the other two included studies, which could contribute to the inconsistent findings.
All the four included studies confirmed that VR-based exercise could improve the speed and agility of people with ID (d = 0.13–0.46).27,31,40,45 This result is consistent with a previous review, where similar findings have been obtained in people with Down syndrome. 37 Of note, Lin and Wuang 45 found that compared with the treadmill exercise, the intervention that combined both treadmill exercise and VR-based exercise led to a greater improvement of agility in adolescents with ID. Thus, future research may explore whether interventions that combine VR-based exercise with one of the traditional approaches (e.g., treadmill exercise) could have a better training effect than those interventions that simply apply a traditional approach. It is worthy to note that VR-based exercise may have better acceptability and compliance than traditional exercise modalities in people with ID. 65
Limitations and future directions
Although the present systematic review provides some evidence that VR-based exercise may benefit HRF and SRF outcomes in people with ID, it was limited by the exclusion of non-English journal articles. In addition, given the small number of studies included and their heterogeneity (i.e., participant characteristics, physical fitness measures), a meta-analysis could not be conducted. Despite the limitations, implications for future research can be derived from the present review. Overall, more studies are needed to understand the benefits of VR-based exercise on physical fitness in people with ID. Particularly, quality RCTs that detail participant characteristics (e.g., age, gender, severity of ID), specify training programs (e.g., type of games, training duration, training intensity), and assess understudied fitness outcomes (e.g., flexibility, body composition, motor proficiency) are needed.
Conclusion
The present review provides some preliminary evidence in that VR-based exercise improves muscular fitness, cardiorespiratory fitness, balance, and speed and agility in individuals with ID. On the contrary, evidence regarding the efficacy of VR-based exercise on body composition, flexibility, and coordination in people with ID is limited. We hope that this review will serve as a reference tool for practitioners when developing and implementing VR-based exercise programs for people with ID. We also hope that this review will proliferate future research in this field.
Footnotes
Acknowledgments
The authors would like to thank the reviewers for their valuable comments and helpful suggestions.
Authors' Contributions
X.L.: Conceptualization; data curation; formal analysis; funding acquisition; and writing—original draft. J.H.: Conceptualization; data curation; formal analysis; and writing—original draft. Z.K.: Methodology and writing—review and editing. F.S.: Methodology and writing—review and editing. C.H.P.S.: Methodology and writing—review and editing. C.L.: Conceptualization; supervision; formal analysis; funding acquisition; and writing—review and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
X.L. is partially supported by the Golden Seed Fund in South China Normal University (22TKKA03). C.L. is partially supported by the National Social Science Fund in China (20BTY027; 22BTY062).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.