
Abstract
Background:
Virtual reality (VR)-enhanced indoor hybrid cycling in people with spinal cord injury (SCI) can be comparable to outdoor hybrid cycling.
Method:
Eight individuals with chronic thoracic-lesion SCI performed voluntary arm and electrically assisted leg cycling on a hybrid recumbent tricycle. Exercises were conducted outdoors and indoors incorporating VR technology in which the outdoor environment was simulated on a large flat screen monitor. Electrical stimulation was applied bilaterally to the leg muscle groups. Oxygen uptake (VO2), heart rate, energy expenditures, and Ratings of Perceived Exertion were measured over a 30-minute outdoor test course that was also VR-simulated indoors. Immediately after each exercise, participants completed questionnaires to document their perceptual-psychological responses.
Results:
Mean 30-minute VO2 was higher for indoor VR exercise (average VO2−indoor VR-exercise: 1316 ± mL/min vs. outdoor cycling: 1255 ± 53 mL/min; highest VO2–indoor VR-exercise: 1615 ± 67 mL/min vs. outdoor cycling: 1725 ± 67 mL/min). Arm and leg activity counts were significantly higher during indoor VR-assisted hybrid functional electrical stimulation (FES) cycling than outdoors; 42% greater for the arms and 23% higher for the legs (P < 0.05). Similar responses were reported for exercise effort and perceptual-psychological outcomes during both modes.
Conclusion:
This study proposes that combining FES and VR technology provides new opportunities for physical activity promotion or exercise rehabilitation in the SCI population, since these modes have similar “dose-potency” and self-perceived effort.
Human Research Ethics Committee of the University of Sydney Ref. No. 01-2010/12385.
Introduction
People with spinal cord injury (SCI) are at risk of developing many SCI-related complications and negative secondary sequelae. In addition, the enforced sedentary lifestyle as a result of wheelchair confinement, environmental barriers, and on-going psychosocial issues may further complicate the consequences of SCI leading to poor physical fitness and health outcomes. 1
There is good evidence that exercise is effective for improving physical fitness and health in the SCI population.2–4 Technological advancements have allowed functional electrical stimulation (FES) to enable leg exercise for people with SCI. FES-assisted exercise can be deployed as static muscle contractions, dynamic knee extensions, rhythmic cycling exercise, or upright stepping.5–7 Previous studies have demonstrated greater oxygen uptake (VO2), cardiorespiratory demands, and enhanced venous return when FES leg cycling is combined with arm exercise.8–10
This arm+FES-leg “hybrid” exercise results in increased activation of muscle mass, augmentation of sympathetic outflow, reduced venous pooling in the legs, higher cardiac outputs, and elevated VO2, thereby providing improved whole-body exercise “dose-potency.”11,12 In recent years, FES-integrated hybrid recumbent tricycles that can be used indoors and outdoors have become commercially available. Exercise training using these hybrid FES-cycles has resulted in improvements of physical fitness after only 4 weeks of training. 13
High-intensity and high-volume exercise programs often provide superior health and fitness benefits but may cause compliance issues in some users. Hettinga and Andrews suggested some strategies to simulate training compliance, which includes virtual reality (VR) exercise. 5 In previous studies, the implementation of FES and VR as complementary tools in post-stroke rehabilitation therapies has been shown to improve the range of motion, maximum angles, and angular velocity that can be integrated into this SCI study.14,15
Though VR has shown countless successes in rehabilitation, the collaboration with FES is yet to be ventured. A non-immersive VR model was chosen instead of a highly immersive VR model, which usually stimulates more extreme graphics that has less susceptible application in SCI subjects. 16 The hybrid model also permits an enhanced exercise capacity and concentration of the user without focusing many variations on rated perceived exertion (RPE).
The hybrid model, especially the VR component, was able to cause a lower heart rate (HR), simultaneously resulting in the exercise duration being prolonged. 17 The correlation is due to a favored parasympathetic predominance in the results compared with a well-adjusted autonomic nervous system. 18 However, there is still limited evidence about the potential for FES-exercise combined with VR technology to produce aerobic fitness benefits.
Materials and Methods
Participants
Eight male subjects (aged 49.9 ± 5.5 years, stature 1.75 ± 0.02 m, body mass 81.1 ± 5.8, body mass index [weight{kg}/height{m} 2 ]; time since injury 9.1 ± 1.5 years) with traumatic SCI level T4–T12, ASIA Impairment Scale A, B, and C (with intact lumbosacral lower motor neuron and good hand function), volunteered to participate in this study.
All subjects underwent full medical screening, which included a physical and neurological examination, a 12-lead resting electrocardiogram, resting blood pressure, and lower limb radiographs. The subjects were healthy, neurologically stable and had at least 6 weeks of previous experience with FES cycling exercise. This study was approved by the Human Research Ethics Committee of the University of Sydney (Ref. No. 01-2010/12385), and all participants underwent written informed consent.
Study design
All subjects performed indoor and outdoor cycling on a commercially available arm and FES-leg (hybrid) FES tricycle (Berkelbike, Berkelbike BV, Netherlands), which incorporated an in-built FES system to recruit leg musculature (Fig. 1). The Berkelbike is a semi-recumbent tricycle with FES-evoked leg cycling and arm cranking modalities for over ground propulsion. 13

Berkelbike BV. Color images are available online.
Subjects regulated their muscle stimulation through the FES system independently to each muscle group via amplitude control, and they could also choose a user-preferred chain-rim gearing for different terrains. A more difficult terrain requires a higher gear compared to an easier one, from within the range of gears that the bike has. The maximum stimulation intensity was 150 mA at a frequency of 35 Hz.
The relationship between the peak energy of the pulse, pulse width, and pulse repetition frequency determines how much energy is sent back to the radar receiver. To measure pulse width, we utilized counter-analysis of the Gate input signal to determine the width of a pulse. Counter-analysis involves scrutinizing contrasting viewpoints within Gate analysis to verify the accuracy and reliability of the measured signal. Here, the width of higher or lower pulses on the Gate signal is measured through the configuration of the counter.
The number of edges returned by the counter was then multiplied by the source signal's periodically yielding the pulse width. The hybrid tricycle could be deployed for both indoor or outdoor arm+FES-assisted leg exercise. When used indoors, it was mounted on a stationary cycle resistance trainer (Tacx i-Magic, Tacx BV, Netherlands) (Fig. 2) that was connected to a computer running commercial software for simulated cycling viewed on a large flat screen monitor (Fig. 3).

Tacx i-Magic BV. Color images are available online.
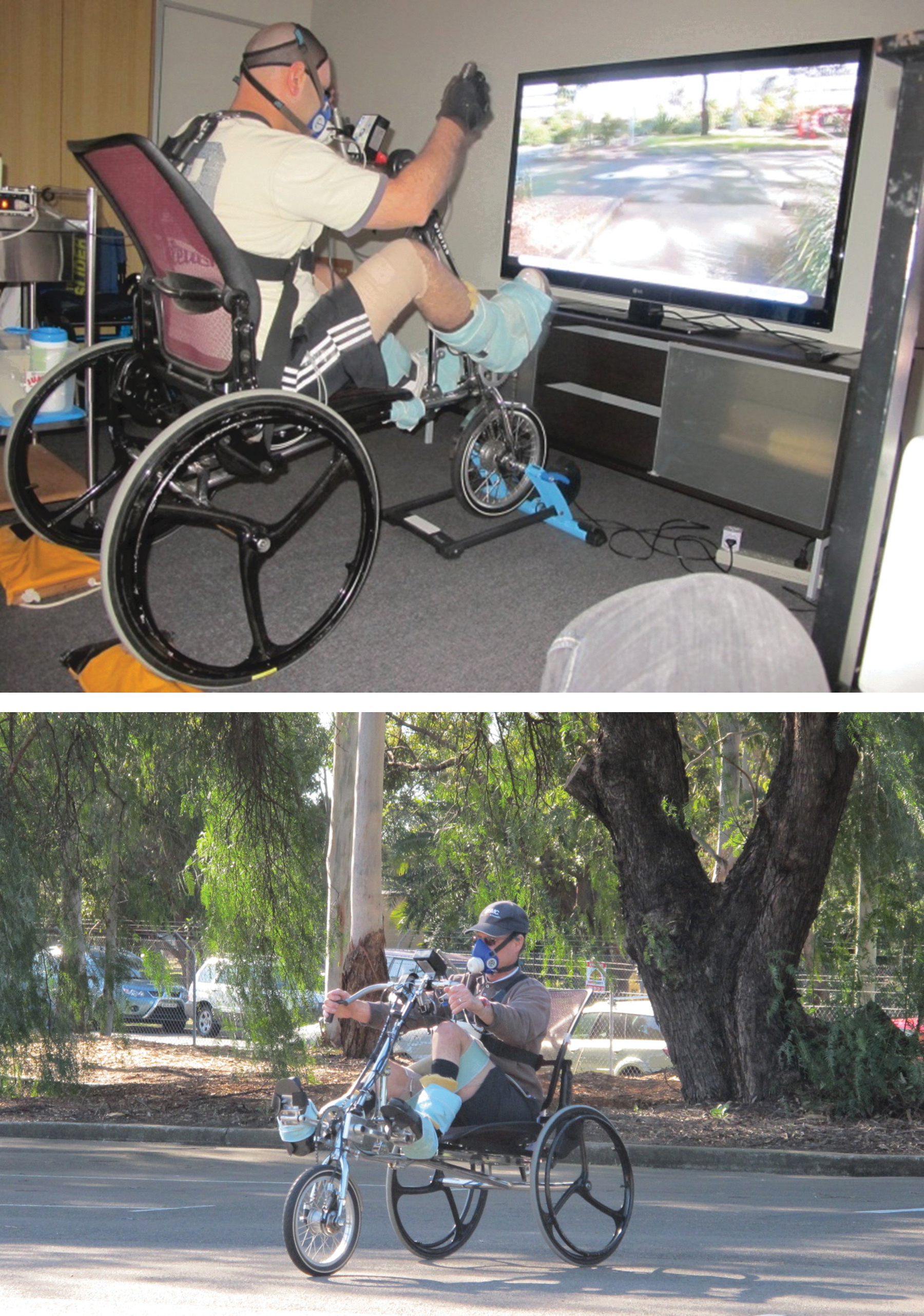
Monitor screen of VR terrain (top panel) and actual terrain (bottom panel). VR, virtual reality. Color images are available online.
The CycleForce frame of the i-Magic is suitable for racing and hybrid bicycles and mountain bikes with a wheel diameter of 610 to 720 mm and a high functioning electronics brake system. The i-Magic interface was then connected once the i-Magic interface and the adapter of the motor brake were mounted onto the frame.
Before the FES cycling, gel-backed self-adhesive surface electrodes were placed over the bellies of the quadriceps, hamstrings, and glutei muscle groups (Fig. 4). Electrode placement was kept consistent by measurements to key anatomical landmarks, ensuring muscle group recruitment was similar between trials. Subject preparation and the experimental set-up were all performed by the author to maintain consistency.

Electrode placement at the
The electrodes were held securely in place by thigh stockings to prevent slippage. Following electrode placement, the subjects transferred onto the hybrid tricycle and had their feet and legs strapped to the pedals and held in position by customized carbon-fiber leg supports for lower-limb stability, thereby minimizing leg movements in undesired directions.
Outdoor FES cycling
The cycling track consisted of paved concrete paths and tarred track around the Faculty of Health Sciences, University of Sydney campus grounds. The complete track was 1260.4 m with elevation change of 19.4 m (+13.37 m, −6.07 m), requiring both left- hand and right-hand turns.
VR indoor cycling
Indoor cycling was performed on the same hybrid FES tricycle mounted onto a Tacx stationary cycle trainer. The hybrid FES tricycle and the cycle trainer were connected to a notebook PC and a 150 cm flat screen full 1080p plasma television to enable VR enhanced cycling. Flat-screen technology was chosen, as it required no sensors, head mounted displays, or other equipment to be attached to the subject.
This enabled unrestricted movement that was deemed necessary for the large body motions elicited during arm and leg cycling. No individuals reported nausea or other symptoms of cybersickness associated sometimes with VR technologies. 19 Comparable to how genuine the movement, such as that experienced on a rocking boat, stimulates the visual and vestibular systems, the symptoms linked with VR situations are similar to that. Virtual reality environment (VRE) produced by computers does not include vestibular stimulation.
Users of VREs can utilize a standardized test called the Simulator Sickness Questionnaire (SSQ) 20 to identify whether they suffer the symptoms of cybersickness. Previous research using the SSQ has revealed that between 50% and 80% of individuals experience mild to severe cybersickness symptoms after being exposed to simulated motion in a VRE.20–23
The virtual environment software (Tacx i-Magic VR Trainer) was programmed to simulate the same outdoor cycling track, so subjects cycled over the same virtual test course. The outdoor cycling track had been previously videotaped using a 1080p high- definition video camcorder and the track properties (distance and elevation) were recorded via a global positioning system unit (Garmin Edge 705, USA). These data along with the video were professionally converted into VR program compatible with the Tacx i-Magic software.
Protocol
Following two sessions of familiarization outdoors, each individual underwent two trials each of indoor and outdoor cycling. 9 These were repeated at least 1 week apart at the same time of the day. Subjects were randomized between conditions of indoor versus outdoor cycling on each test day.
For outdoor trial, participants were instructed to cycle for 30 minutes and complete as many circuits of the 1260 m cycling track as they could within that duration. They were encouraged to cycle to their best effort within self-perceived safety limits and to increase their stimulation intensities to the legs within personal tolerance. The primary investigator cycled behind the subject to provide encouragement and advice on terrain safety during turning.
As with the indoor trial, the subjects were instructed to cycle for 30 minutes on the stationary tricycle in front of the television and to complete as many circuits of the simulated track as they could within that duration. The subjects were encouraged to cycle to their best effort within safety limits and increase their stimulation intensities, as they deemed necessary.
Indoor VR testing was conducted in a quiet darkened room. The monitor was mounted 1.5 m from the subjects' open eyes, with 0 deg elevation from eyes to screen center. The primary investigator stood outside of subjects' field of vision to provide encouragement of best effort.
Measurements of cardiorespiratory performance during cycling
Cardiorespiratory variables and HR were measured continuously breath-by-breath using the Cosmed K4b2 portable metabolic system (Cosmed, Italy). The K4b2 has been accepted to accurately measure VO2 and estimate energy expenditure over a wide range of metabolic rates in adults. 24 The subjects breathed through a rubber face mask (Hans Rudolph Inc., Kansas City, USA), into the portable metabolic system.
The system was calibrated before each test according to the manufacturer's instructions. This portable system and the battery pack were attached to the subject's trunk via a snug fitting harness. 25 Breath-by-breath VO2 was smoothed using a three-step ensemble-average, and then averaged every 15 seconds (Data management software, Cosmed, Rome, Italy). An index of metabolic stress [Net oxygen (O2) cost; mL/(kg·min)] was calculated from speed, body weight, and VO2, whereas cardiorespiratory strain (Physical Cost Index, b/m) was calculated from HR and speed.
Limb movements measurements
Two Actigraph GT3x (ActiGraph, Pensacola, USA) tri-axial accelerometers were used for motion analysis of the cycling limbs. A study by Warms and Belza had previously established that actigraphy was suitable as a measurement of physical activity for people with SCI. 26 A GT3x was strapped on the dorsal aspect of the left wrist and ankle of each subject.
The activity monitors sampled movement data every second as the sum of the number of “counts” captured at a rate of 33 Hz along the x, y and z axes. The data were ensemble-averaged every 10s to reduce excess noise, and total activity counts over 30 minutes were collected. Activity counts represented by the GT3x, characterized a combination of limb movements and “vigor” (forces) as measured by the hardware in 0.01664 g/(s·count), where each level is considered as one (1) count. 27
By mounting the accelerometers on the wrists and ankles of the subjects during arm and leg (hybrid) cycling both indoors and outdoors, it was possible to collect data on how “active” the arms and legs were throughout the entire duration of the cycling.
Psychological measurements
RPE were requested at 15 and 30 minutes using a Borg Category Ratio 10-point scale (BORG CR 10) during all trials. Grange et al. 28 had observed that perceived exertion using the BORG CR 1029 was a useful measure of exercise intensity in individuals with SCI during 45-minute wheelchair ergometry in a supervised clinical setting. During the familiarization session, each subject was given instructions on the use of the BORG CR 10. During the trial, subjects were requested to provide their RPE score at 15 minutes and at 30 minutes. The answers were hand-signaled as they were breathing through facemasks.
At the end of each cycling trial, the subjects were asked about their cycling experience through face-to-face questionnaire interviews. The Exercise-induced Feeling Inventory (EIFI) developed by Gauvin and Rejeski was used to measure feelings evoked by the 30-minute hybrid FES cycling exercise. 30 The EIFI is a self- report that requires the user to answer on a 5-point scale anchored by 0 = “do not feel” and 4 = “feel very strongly.” The EIFI measures “positive engagement,” “revitalization,” “tranquility,” and “physical exhaustion” by totaling three-item response scores in four subscales. Gauvin and Rejeski observed that the EIFI was very sensitive to changes in feeling states that occur with exercise, and that the measure was able to detect differences in the social context of different exercise interventions. 30
Participants also completed the Activation-Deactivation Adjective Checklist (AD-ACL), 31 which is a measure of activation or arousal state after the cooling down period post-exercise in all trials. The AD-ACL is a multidimensional test of various transitory arousal states consisting of 20 items with 4 subscales: energy, tiredness, tension, and calmness. The items are rated on a 4-point Likert scale; higher scores reflect greater intensity of mood. In this study, the scores of subscales energy and tension were analyzed since they are the best indications of energetic and tense arousal respectively.
User satisfaction measurements
The Quebec User Evaluation of Satisfaction with Assistive Technology Questionnaire (QUEST 2.0) 32 was used to evaluate subjects' experience and satisfaction with using the hybrid FES tricycle. The QUEST 2.0 was designed as an outcome measurement instrument to evaluate a person's satisfaction with a wide range of assistive technology.
The QUEST 2.0 is a self-administered questionnaire consisting of 12 items rated on a 5-point satisfaction scale. Response ranges from 1 (not satisfied at all) and 5 (very satisfied). The 12 items are subscales of eight assistive device items and four service items. In this study, only items within the assistive device were included, that is, satisfaction with the dimensions, weight, ease of adjusting, safety and security, durability, usability and effectiveness of the assistive device.
Finally, subjects' experience using VR-assisted hybrid FES cycling was assessed using the Virtual Reality Symptom Questionnaire (VRSQ). 33 The VRSQ was developed for use in investigating symptoms that result from VR viewing. It consists of 13 symptom questions: 8 non-ocular (general discomfort, fatigue, boredom, drowsiness, headache, dizziness, difficulty concentrating, and nausea) and 5 ocular (tired eyes, sore/aching eyes, eyestrain, blurred vision, and difficulty focusing).
The VRSQ was administered during the familiarization session so that subjects were familiar with the questionnaire during the test trials. The questionnaire was administered immediately following the cessation of exercise before the symptoms dissipate as suggested by Ames et al. 33 that the assessment of symptoms needs to occur in the first 5 minute of post-viewing.
Differences of outcome measures obtained during outdoor versus VR-assisted indoor hybrid FES cycling were analyzed by two-way analysis of variance (ANOVA). All statistical analysis was performed using the SPSS 21 statistical package. Data are presented as mean ± standard error, and the level of statistical significance was set to the 95% confidence limit (P < 0.05).
Mechanical efficiencies
During indoor cycling, speed (m/min), distance (m), and power output (W) were recorded from the software that controlled the hybrid tricycle (Tacx i-Magic). During outdoor cycling, the Garmin GPS system was used to record speed (m/min), and distance (m) cycled over the 30-minute test duration. Outdoor power output (W) was estimated by an internet online calculator (Bikecalculator.com) with inputs of rider body weight, cycle weight, tire type, and environmental conditions.
The authors note that power output for outdoor cycling reported herein is only a proxy of true power output, since the online calculator was devised for a cycle with two wheels. Gross mechanical efficiency (MEG; %) and net mechanical efficiency (MEN; %) were calculated as a function of power output (Equation 1 & 2) and VO2. These variables were calculated using the formulae:

where
[Power Output (W), 6.12 = kgm × W−1, 426.8 = kcal × kgm−1, VO2 (mL·min−1) and respiratory exchange rate (RER) × 1.232 + 3.815 is Caloric Equivalent of non-protein RER by linear regression, but when RER >1.0 was taken to be RER = 1.0].
This implies that they measure fundamentally different aspects of mechanical efficiency (ME) when compared with other problems and imprecisions with other efficiency indices, whereas gross efficiency seems to be the best indicator for ME because of its consistency and unambiguity. The methodological approach of MEN calculation is nontransferable to other works of a similar kind as the efficiency indices fall into a class that is incapable of interacting with each other. 18
Results
Eight subjects completed all indoor and outdoor trials. ANOVA revealed that there were no differences between trials (trial 1 vs. trial 2) or between conditions (outdoor exercise vs. indoor VR-exercise) for most of the cardiorespiratory measurements (P > 0.05). Where there were differences between exercise modes, but not between trials within modes, the data presented were pooled data from both trials.
The average VO2 during outdoor cycling was 1255 ± 53 mL/min and during indoor VR-exercise was 1316 ± mL/min. The highest VO2 observed during outdoor cycling was 1725 ± 67 mL/min and during indoor exercise was 1615 ± 67 mL/min. Average HR during outdoor cycling was 128 ± 3 b/min and during indoor exercise was 125 ± 3 b/min. The highest HR during outdoor cycling was 153 ± 4 b/min and during indoor cycling was 149 ± 4 b/min. There were no significant differences between these VO2 and HRs between modes (P > 0.05).
There were no significant differences in net O2 cost and physical cost index between modes. The cycle performance, metabolic stress (Net O2 cost), and cardiovascular strain (Physical Cost Index) are presented in Table 1.
Cycle Performance, Metabolic Stress, and Cardiovascular Strain During Indoor-Virtual Reality Versus Outdoor Exercise
Data are mean ± standard error.
Denotes P < 0.05.
O2, oxygen; VR, virtual reality.
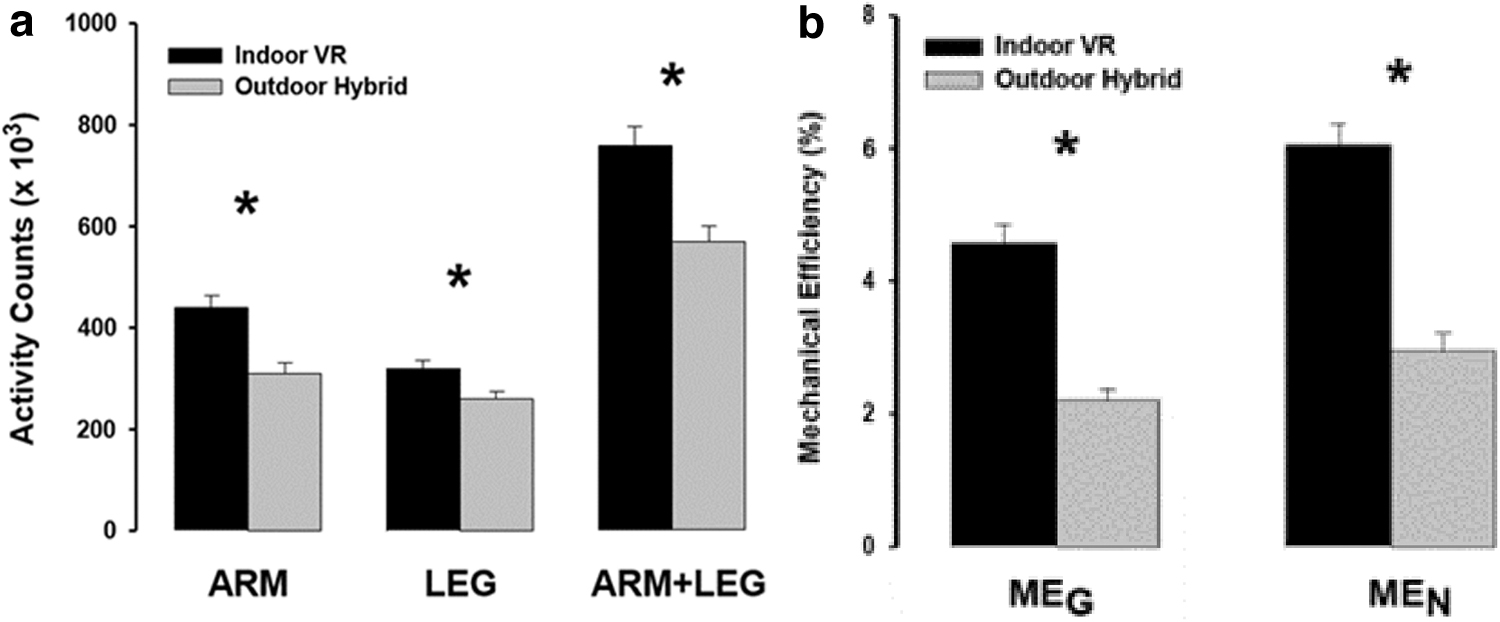
A greater distance was cycled indoors compared with outdoors—almost twice (1.8 times) the distance over the 30 minutes of cycling. Hybrid tricycle speed was 2.2 times faster during indoor cycling compared with outdoor cycling. Arm, leg, and arm+leg activity counts during VR-assisted hybrid FES cycling indoors were significantly greater than observed during outdoor cycling. During indoor cycling the total arm activity was 42% more and leg activity was 23% more than was observed during outdoor cycling (Fig. 5a).
Despite the initial assumption that outdoor hybrid FES cycling might contribute to superior psychological outcomes than indoor exercise, two-way ANOVA showed no differences in the subscales of the EIFI (positive engagement, revitalization, tranquility and physical exhaustion) and the subscales AD-ACL (energy, tiredness, tension, calmness) between cycling modes. There were also no significant differences in RPE at 15 and 30 minutes of exercise during both modes.
The RPE at 15 minutes during outdoor cycling was 5.9 ± 0.4 and during indoor VR-enhanced cycling was 6.3 ± 0.4. At the end of the exercise (i.e., at 30 minutes), the RPE was 8.1 ± 1.8 during both outdoor cycling and VR-enhanced indoor cycling, consistent with the feeling of exercising very hard. 29 From the QUEST, it was observed that the subjects were satisfied with the hybrid FES tricycle, but there were no differences in satisfaction between modes.
The VR-assisted FES cycling did not result in high ocular symptoms assessed from the VRSQ. The total scores for the ocular symptom ranged between 0 and 16 out of a possible score of 30.
Since there were no significant differences of VO2 between the two cycling modalities, the calculated net oxygen cost which was significantly higher during outdoor cycling and the calculated physical cost index was also estimated to be significantly higher during outdoor cycling. VR-assisted hybrid FES cycling indoors was more mechanically efficient compared with outdoor cycling (Fig. 5b). MEG during indoor cycling ranged between 4.1% and 5.1% from the subjects compared with 1.7% to 2.7% for outdoor cycling. MEN during indoor cycling ranged between 5.4% and 6.7% for the individuals compared with 2.3% to 3.6% for outdoor cycling.
The VR-assisted hybrid indoor FES cycling revealed a significantly higher MEG, MEN, activity counts for arms and legs, distance traveled in 30 minutes, and speed compared with outdoor hybrid FES cycling (P < 0.05). The power output readings were also significantly higher, but since it was derived as an estimate, it was not considered as the main outcome. 27
Discussion
This work revealed some interesting features about how SCI users approached the two exercise conditions by manipulating “cruising and steering” and “gearing” of the tricycle. In addition, the expectation of a greater indoor VR-cycling performance over outdoor cycling was borne out in the current study. This could be attributed to a number of casual factors.
The average and peak cardiorespiratory data were consistent with previously reported studies that employed submaximal and maximal FES arm and leg cycling exercise.5,13,34–40 These findings, in part, reject the initial assumption that VR-indoor hybrid cycling would engender greater cardiorespiratory responses due to a higher cycling performance for that mode. The RPE reported during the 15 minutes of cycling were also consistent with the description of exercising “hard,” and “very hard” at the end of 30-minute exercise.41–43
The greater cycling performance in terms of number of cycles and derived distances for VR-indoor exercise was observed, but the expected translation to higher cardiorespiratory responses was not. The subjects were instructed to cycle to their best ability and were allowed to self-select their speed and gear ratio to ensure safety and comfort both indoors and outdoors.
Hence, they selected different gearing indoors and outdoors to maintain their metabolic responses within a range perceived as “safe” but “comfortable” (i.e., “moderate” exercise intensity) over 30 minutes. These findings clearly demonstrated that exercise outcomes in this subject population might not be influenced by the “reality” of exercise modality (i.e., outdoor exercise or VR- assisted indoor exercise), but by self-perceptions of effort that SCI users could control by “gearing” within a moderate-intensity metabolic range that could be sustained over 30 minutes.
The lack of difference in metabolic and HR demands between VR-assisted indoor exercise and outdoor exercise over ground cycling implies that either condition may be selected by the individual with SCI if the goal is physical activity for health promotion. For individuals desiring an “outside” experience or whether they may prefer indoor exercise, either is beneficial. For the clinician or therapist who might recommend hybrid cycling for either rehabilitation or fitness training, the selection of optimal condition becomes a matter of client-focused preferences.
It was clearly observed during the experiments that during indoor cycling the subjects arm-cranked nearly continuously throughout the 30-minute duration of the test course. In contrast, during outdoor cycling, the subjects incorporated cruising techniques while going down slopes and careful steering techniques during cornering. This “cruising and steering” effect lessened the number of arm activity counts and leg movements; when the arms were not cranking to cruise and steer the tricycle, the legs did neither.
With less active limb movements developed over 30 minutes of outdoor cycling, the average velocity was slower (by 126 m/min) and the distance traveled was much less (by 55%) at approximately half of the estimated average power output. The author speculated that even though all participants were provided with familiarization sessions, the nature of the undulating terrain of the test course and the nature of the tricycle made them more cautious about possible tipping, and they adopted more careful cruising and steering strategies.
The MEs observed in this study seemed low, but this may be compromised by the low accuracy of the estimated power output measurement. The authors were, therefore, unable to compare the findings with some other previous studies on FES-leg cycling.44,45 Previous studies have reported MEG values as low as 4%–6% for FES-evoked cycling.34,45,46
A low ME was not surprising as the mode of exercise was arm and FES-leg cycling, and it has been previously reported that metabolic efficiencies were lower during arm cranking compared with voluntary leg cycling due to the postural and body stabilization required during arm cranking exercise.17,47,48
Blake and Wakeling provided evidence that muscle coordination, power output, and overall ME fluctuate during an outdoor time trial due in part to the pacing strategy and changing terrain. 49 It was interesting to find that the Net Oxygen Cost and Physical Cost Index were significantly higher during outdoor cycling compared with VR indoor exercise. This outcome could be attributed to the cycling inefficiencies during outdoor exercise.
Conclusion
VR-enhanced hybrid indoor cycling produced no different cardiorespiratory responses than outdoor arm+leg cycling. Nevertheless, limb movement counts and power output were higher during the indoor cycling possibly due to user-adjusted gearing, steering, and cruising techniques that were adopted during outdoor exercise. Combining FES technology and virtual reality technology may provide new opportunities for physical activity promotion or exercise rehabilitation in the SCI population.
Footnotes
Acknowledgments
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work is partially supported by the Ministry of Higher Education Malaysia (Grant No. FRGS/1/2021/SKK06/UNIKL/03/3).