
Abstract
Purpose:
Virtual reality is widely used in patients with chronic musculoskeletal problems. However, the short-term effects on individuals with transtibial (TT) amputation during this process remain unclear. This study aimed at investigating the effects of virtual reality on rehabilitation outcomes in TT amputees.
Methods:
The study included 20 TT amputees who were using TT prostheses. The participants were divided into two groups randomly as follows: physiotherapy (PT) and virtual reality (VR). Participants were treated 3 days a week, for 4 weeks, and evaluations were made before and after treatment; a 6-minute walk test was used for performance, a single-leg balance test for balance, Trinity Amputation Prosthesis Experience Scale for prosthesis satisfaction, a 10-meter walking test for gait speed, and a wearable smart t-shirt to determine cadence.
Results:
It was found that there was a statistically significant difference in performance, balance, prosthesis satisfaction, cadence, and gait speed before and after PT (P < 0.05). There were differences in terms of performance, prosthesis satisfaction, balance, cadence, and gait speed before and after VR (P < 0.05). There was no statistically significant difference between PT and VR (P > 0.05).
Conclusion:
The 4 weeks of VR training improved performance, prosthesis satisfaction, balance, cadence, and gait speed in TT amputation rehabilitation similar to physiotherapy methods. The addition of VR training to amputation rehabilitation will bring improvements since it is a fun and safe intervention.
Clinical Trial Registration:
The trial is registered at Clinical Trials.gov, Trial No: NCT03872193
Introduction
In the physiotherapy training of amputees, carrying objects, walking training, office activities, climbing, strengthening, methods of virtual reality (VR), or video-based play therapy, which have become increasingly more common in recent years, are reported in the literature.1–3 The primary purpose of PT is to help patients to continue living in society by maximizing their mobility and ambulation. 4 PT in long-term prosthesis users contains exercises to improve the functionality of individuals.5,6 When amputees become active ambulators, they are directed to vocational and recreational activities.7,8 First, an evaluation for residual functional capacity is done 9 ; amputees may be able to improve their mobility, performance, and balance. 10 PT in this period can enhance the amputee simulate activities of work and recreation. 8
VR or video-based play therapy enables individuals to perform three-dimensional physical activities in a virtual environment.11,12 This virtual environment provides feedback and enjoyable activities to participants for the practice of the real-world tasks. Motor skills can be learned by virtual environments or video-based play therapy and the participants can reflect these skills in real life. 13 Then, VR is included in the rehabilitation process.14–16 VR is used to improve walking, balance, to decrease phantom and residual limb pain, and to provide the functionality of prostheses.2,17,18 Tao et al. 19 stated that VR could be used for balance with an application of a 4-week home-based program on older amputees. Studies usually take place as case series or as studies with comparative groups including healthy individuals and home-based programs.
To our knowledge, there is a small number of evidence about the short-term effects of VR on transtibial (TT) amputee rehabilitation outcomes in the literature.16,19 This study aimed at investigating the short-term effects of VR on rehabilitation results in TT amputees. The hypothesis of this study was created with this view to determine the short-term effects of VR in individuals with TT amputation.
Materials and Methods
The study was approved by the Hacettepe University Research Ethics Committee GO Decree No.16/283-38 in 2016. An informed consent form was obtained from all human study participants. The primary outcome of this study was performance. This study, in which we evaluated the effectiveness of VR in TT amputees, was performed at the Bilim Orthosis and Prosthesis Center between May 2017 and March 2018.
The inclusion criteria of this study were determined by the individuals' willingness to participate in the study after being given detailed information, being TT and unilateral amputees, being between 18 and 65 years old, being able to walk independently for at least 15 minutes, having stable residual limb and standard TT residual limb length, being cooperative, and able to understand the tests and evaluations. The Medicare Functional Classification Level was used for the classification of functional levels (K2: Limited community ambulator, K3: Community ambulator who can traverse most environmental barriers, K4: People who have prosthetic ambulation ability or potential exceeding the basic ambulation skills, athletes). 20 K4 level of amputees have the best functionality level. For the homogeneity of the groups and for the exercise program to have the same level of difficulty, all participants were chosen from the K4 level. 20
Exclusion criteria were determined as muscle shortness, limitation of joint movement and phantom pain in the residual limb, the presence of any discomfort or systemic health problem affecting walking except amputation, the presence of visual problems preventing participation in VR, and the use of a walking aid that prevents walking and other activities. Residual limb length was measured with an elastic tape measure. The joint movement was evaluated with a universal goniometer.
Participants were divided randomly into two groups (Fig. 1). The authors generated a random list through an internet site called “www.random.org” with a 1:1 ratio. Twenty volunteering subjects with TT amputations were randomly divided into two groups as Group 1—Physiotherapy (PT) and Group 2—Virtual Reality (VR). Amputees received a number according to the order they applied in the clinic, and it was decided that they would be included in the virtual reality or exercise group according to the list obtained from the site. A qualified physiotherapist performed the rehabilitation process for 4 weeks for both interventions. The authors recorded the demographic and clinical data of all individuals (Table 1).
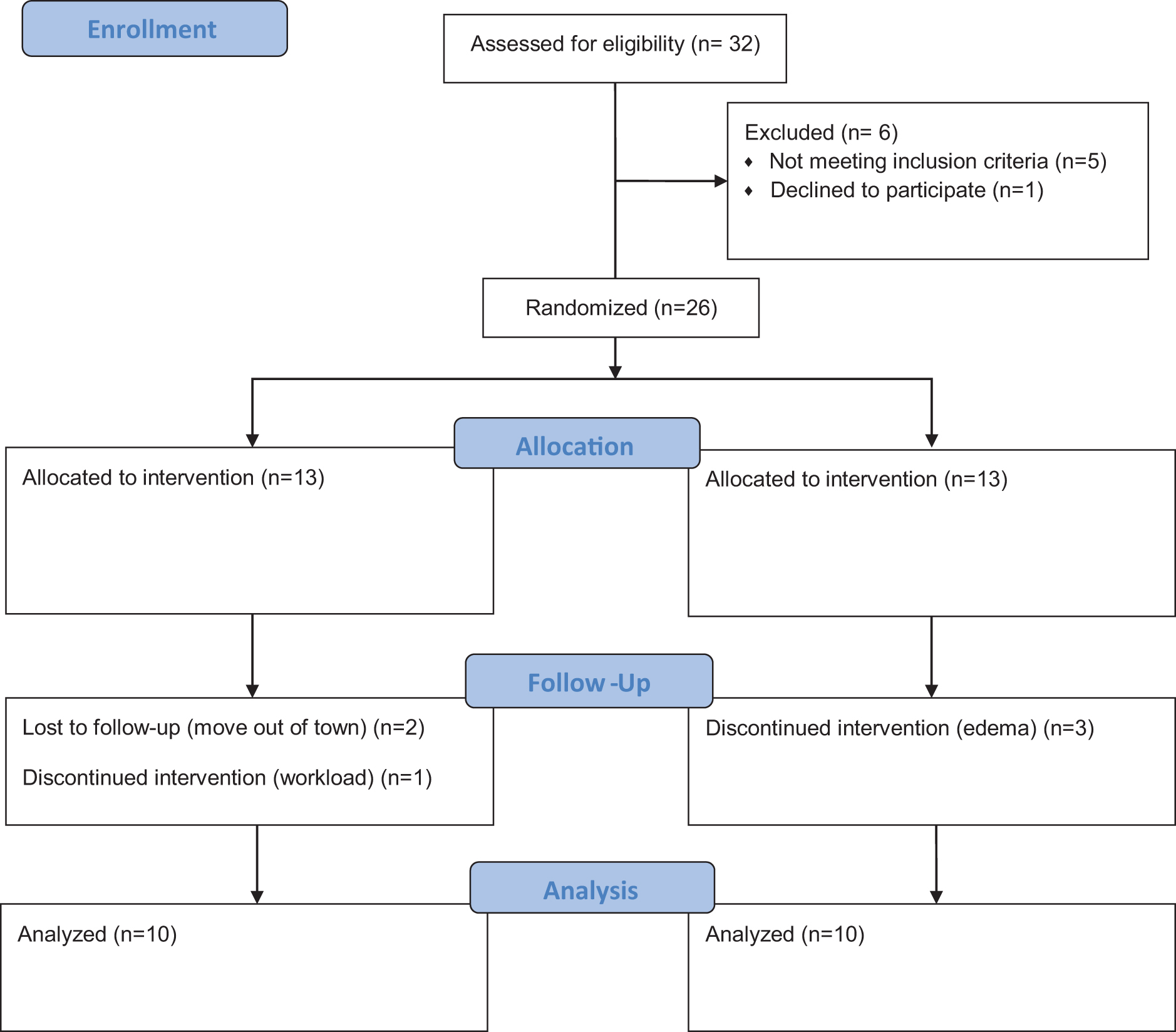
Flow diagram of participants showing the division into two groups.
Demographic Features of Subjects
P < 0.05.
Max, maximum; Min, minimum; PT, physiotherapy methods; VR, virtual reality.
Exercise protocol
Subjects exercised in the rehabilitation room of a private prosthesis and orthosis center. The exercises focused on hip and core strengthening, balance-oriented exercises such as obstacle management, walking training such as lateral and backward walking, carrying heavy objects such as 5 kg for each hand, walking on rough, unstable surfaces, on a line with speed and closed eyes, and exercises specific to work such as walking up and down the stairs and recreational activities in the physiotherapy methods group (PT). 16 Exercises with balance ball, walking on a narrow support surface, walking on rough, grassy, sandy, pebbly ground, and crossing obstacles were studied. Functional activity training such as walking on uneven floors and walking with weights was given.11,13 As recreational and work activities, individuals are generally interested in football and gardening.
As for activities, strengthening weak muscles such as abdominals and hip muscles, balance exercises for sound limbs, running outside, jumping, and resistive exercises that increase endurance16,19 were preferred.
VR protocol
The Kinect X-Box program (Microsoft, Redmond, WA, USA) was used within the VR group. The names of the games were Kinect Sports, Motion Sports, and Xbox Dashboard. Within the scope of the applications, activities such as skiing, football, jogging, and rafting were done, so that movements similar to hip flexion, abduction in both healthy and prosthetic limbs, weight transfer to both healthy and prosthetic sides, body lateral flexion, and flexion, jumping, bilateral arm flexion, and squats were performed.11,16 Movements used in games were recorded with Kinect. Motion capture data were then used to show the patient's in-game performance guiding the patient through the same movements. It consisted of hip abduction, flexion, weight transfer, knee flexion, and a series of lower extremity and trunk movements used in the games. The games chosen were determined to include regular, repetitive movements as well as all movements in the lower body.
These two factors (movements and repetitions with varying degrees of freedom) have proven useful in state-of-the-art rehabilitation therapies. Body and limb movements during each game were performed simultaneously with the original music recorded in the game. With repeated sessions, the patients followed the virtual games and repeatedly applied lower extremity and trunk movements for rehabilitation11,16 (Fig. 2).
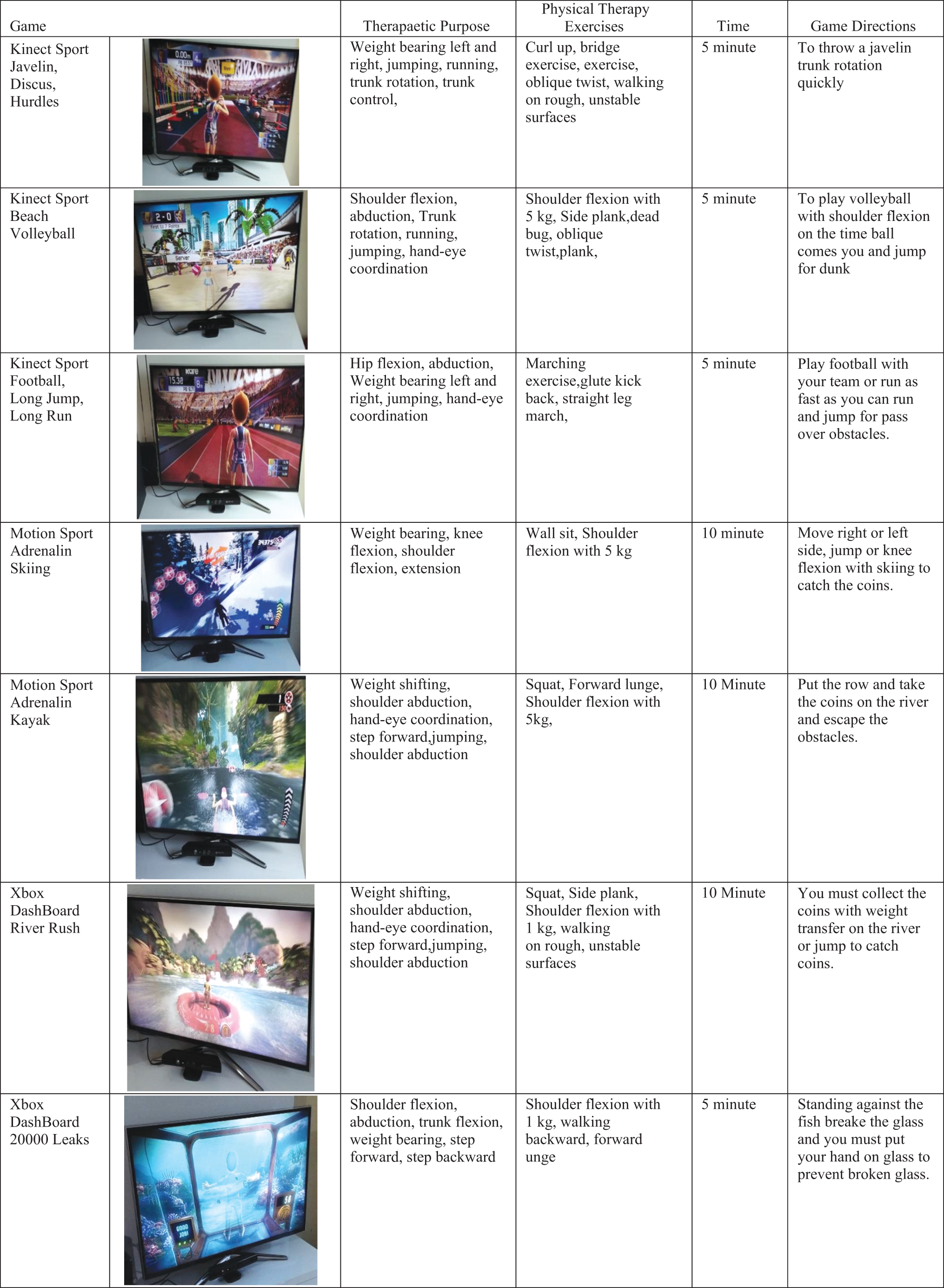
Microsoft Kinect Xbox 360 virtual reality: physical therapy exercise program.
The PT group's exercises took about 1 hour. The VR group's exercises took about 1 hour as well. The applications were performed on the individuals for 3 days a week, for 4 weeks. Results of the evaluations were recorded each week before practices and at the end of the week. At the beginning and the end of the practices, easier activities were determined for both groups and warm-up and cool-down exercises were performed.
Six-minute walk test
Six-minute walk test (6MWT) is used to determine aerobic exercise capacity and performance. It is a valid and reliable test for TT amputees. Subjects were asked to walk as fast as possible for 6 minutes in a 15-meter corridor. During the test, a physiotherapist directed the amputee from a fixed point and used standard expressions. After the test, the distance of the 6-minute walk was recorded. 21
Single-leg balance test
The single-leg balance test is used to show balance loss of individuals with both the healthy extremity and the prosthetic limb. The individual was asked to perform hip-knee flexion until balance loss was determined. The duration was recorded from the starting point until the extremity in the air touched the ground. The test was repeated three times on both sides and a mean was recorded. The chronometer was integrated into the biometric device.22,23
Trinity Amputation Prosthesis Experience Scale
Subjects filled the Turkish version of the Trinity Amputation Prosthesis Experience Scale (TAPES), which is a multifaceted assessment tool developed to determine prosthesis satisfaction level in the amputees. 24 A psychosocial adjustment subscale is scored with a 5-point Likert scale. The total score that can be obtained from this area varies from 5 to 75 and a high score indicates that the adjustment level is high. The activity restriction subsection is scored with a 3-level Likert scale. The score that can be obtained in this area ranges from 12 to 36 and a high score activity indicates that the limitation is high. The lower section of the prosthesis satisfaction is scored with a 5-point Likert scale. The score that can be obtained from this area ranges from 10 to 50 and a high score shows high satisfaction with a prosthesis. 25
Hexoskin Smart Shirt
A Hexoskin Smart Shirt (Montreal, Canada), which has been identified as valid and reliable for the gait parameter cadence of individuals, was used. 26 Data recorded during walking were reflected by Bluetooth to the application previously downloaded to a mobile phone. Cadence was determined with this method. 26
10-Meter walk test
The gait speed was identified with a 10-meter walk test and this test is valid and reliable to examine the gait speed for lower limb amputations. The time it took for the individual to walk the 10-meter distance at a pace of his/her choice was recorded. A stopwatch was used to record the times. 27
Statistical analysis
Statistical analysis used in the research was performed using SPSS 18.0 software. Conformity of the variables to normal distribution was examined using visual (histogram and probability graphs) and analytical methods (Kolmogorov–Smirnov/Shapiro–Wilk tests). Since parametric test conditions were not met, the statistical significance of time change for parameters in nonparametric conditions was investigated by using the Friedman test. In-group paired comparisons were made using the Wilcoxon test. For paired comparisons between the groups, the Mann–Whitney U test was used. 28 The size of this study sample was determined with the G*Power program (version 3.1.9.4.; Universität Düsseldorf, Düsseldorf, Germany) with 5% type 1 error, 10% type 2 error, and 90% power to be obtained. When the statistical significance of alpha was found to be 5%, and the confidence interval was taken as 95%, the power (1-β) of the study was found to be 90%.
The sample size was determined based on a pilot study with 6 amputees, on performance with the 6MWT. With a sample size of 9 in each group, the difference between the averages of the changes in the pre/post-training test time of the two groups was calculated as 6.25 and the difference between the standard deviations was 2.35. It was determined that there should be at least 9 subjects in each group (a total of 18 people).
Results
A total of 20 subjects with a mean age of 38.10 ± 13.42 years participated in this study (Fig. 1). All subjects included in the study consisted of male TT amputees using carbon foot prosthesis with an active vacuum system for at least 1 year.
Age, body mass index, residual limb length, and duration of prosthesis use were similar in both the PT and VR groups (P > 0.05) (Table 1).
Reasons for amputation, systemic diseases, and amputee sides are given in Table 2.
Clinical Features of Subjects
After the 4-week training programs, the improvement of the performance of individuals was examined and the change in weeks was found as statistically significant in both groups (pvr < 0.001, ppt = 0.001). Therefore, paired comparisons were made in-group. The evaluation in groups that created a difference in the VR group was before the treatment, on the 3rd week of the treatment, and on the 4th week of the treatment. On the contrary, the evaluation in the PT group that created a difference was found before the treatment and on the 1st week of the treatment. The difference was found between groups in all evaluations between the PT and VR groups (P < 0.05) (Table 3).
Performance, Balance, Gait Speed, and Cadence of Subjects Intra- and Between Groups
P < 0.05, **P < 0.001.
MWT, minute walk test.
In the TAPES questionnaire, psychosocial compliance, activity restrictions, duration of daily prosthesis usage, and prosthesis satisfaction were considered. For the psychosocial compliance subscale subheading, change in time was not found statistically significant in either group (pvr = 0.075, ppt = 0.998). Therefore, no paired comparisons were made within the group. No difference was determined in any of the evaluations between the PT and VR groups and in any of the intergroup evaluations (p0 = 0.796, p1 = 0.95, p2 = 0.98, p3 = 0.97, p4 = 0.79).
For the subheading of prosthetic satisfaction, change over weeks was found statistically significant in the VR group (pvr = 0.008). Change over time was not statistically significant in the PT group (ppt = 0.094). In paired comparisons within the VR group, evaluation in the 4th week was found to be different. No difference was found in any of the evaluations between the PT and VR groups (p0 = 0.73, p1 = 0.78, p2 = 0.75, p3 = 0.68, p4 = 0.64).
There was no significant statistical difference in the duration of prosthesis usage, which is a subheading of the TAPES questionnaire in both VR (P = 0.448) and SPM groups, before and after treatment (P = 0.470). No intergroup difference was found before (P = 0.015) and after treatment (P = 0.059).
For both groups, balance evaluation was found to be statistically significant in the change of weeks with both the healthy extremity (pvr = 0.008, ppt = 0.004) and the prosthetic limb (pvr < 0.001, ppt = 0.001). In paired comparisons between groups, while the evaluation was on the 3rd and 4th weeks of the treatment on the prosthetic limb in the VR group, the evaluation was before the treatment and on the 1st and 4th weeks of the treatment in the PT group. For all evaluations between the PT and VR groups, only the prosthetic limb balance between groups on the 3rd and 4th weeks of treatment was found to be different (P = 0.029, P = 0.028) (Table 3).
After the 4-week training, a statistically significant difference was found in cadence in the PT and VR groups, and in-group evaluations (pvr = 0.000) (ppt = 0.002). In paired comparisons, it was seen that the evaluations on the 1st and 4th weeks of the treatment in the VR group and on the 1st and 2nd weeks of the treatment in the PT group caused a statistically significant difference (P < 0.05). When comparisons between the groups were examined, a statistically significant difference for all evaluations was found (p0 = 0.04) (p1 = 0.002) (p2 = 0.01) (p3 = 0.009) (p4 = 0.01) (Table 3).
As for gait speed, a statistically significant difference was found between the PT and VR groups in the intragroup evaluations (pvr = 0.007, ppt = 0.002). In paired comparisons, a statistically significant difference was found in the evaluation before the treatment and on the 1st week evaluation of the VR and PT groups (P < 0.05). In the comparison between the groups, the authors found a difference in all evaluations (p0 = 0.02, p1 = 0.02, p2 = 0.003, p3 = 0.007, p4 = 0.007) (Table 3).
Discussion
This study was done to evaluate the short-term effects of VR on rehabilitation outcomes and to compare PT improvements in performance, balance, prosthesis satisfaction, cadence, and gait speed after 4 weeks of application in TT amputee rehabilitations. This tells us that VR affects rehabilitation outcomes positively and can be used in individuals with TT amputations. This study is one of the few studies on the short-term effects of VR on rehabilitation outcomes in individuals with TT amputation.
When the literature is examined, the 6MWT is observed to be a widespread test in the performance evaluations of amputees.21,29 It was observed that the walking distance increased significantly in both groups at the end of the 4-week treatments. After 4 weeks of VR, it was observed that the 6MWT results were better than PT. It was considered that the reason for the development seen in the VR group is the mirror neuron system's activation by monitoring the image of the person in the virtual environment and this system is believed to increase motor performance and that the individual himself can see this. 13
An improvement was observed in performance in the PT group but not as much as the VR group. It was thought that this is because the age range of the subjects was higher, and the subjects were more active and quicker in virtual reality exercises compared with the other exercises.
Tao et al. 19 aimed to evaluate the validity, reliability, and balance performance of VR with an application of a 4-week home-based balance program. It was emphasized in the study results that VR could be used in balance training in older adult amputees. They have stated that VR has effects on postural control in older adult amputees with loss of balance and reported that short-term results are effective on balance but not on physical performance. 19 In this study, when the balance results of the PT and VR groups were compared before and after the treatment, it was seen that there was a difference in both the sound limb and the extremity of the prosthesis. Improvement in the results of applications in both groups shows that PT and VR had positive effects on balance.
Van Helm et al. 30 determined that limitation of activity in individuals with lower limb amputation is caused by strength and balance loss of hip muscles of individuals. They also stated that this situation will negatively affect the gait of individuals and consequently, this situation can be eliminated by active lifestyle interventions. Lifestyle interventions for the people with a lower limb amputation may improve the physical and psychosocial functioning of people with lower limb amputation.30,31 In this study, it was determined that there was no difference in the intra- and between-activity limitations, in the subheading of activity restriction.
Studies comparing the effect of the prosthesis satisfaction questionnaire scores on amputees with different prostheses are common in the literature, but studies evaluating prosthetic satisfaction before and after applications are rarely encountered. Eskridge et al. 32 stated that military amputees were satisfied with the overall functionality of their prosthesis but dissatisfied with the effect of their prosthesis on clothing and skin. Sheehan et al. 33 suggested that VR-based rehabilitation programs can be used for military-specific lower limb amputees for improvement of prosthesis satisfaction. After 4 weeks, it was determined that there is a difference in favor of the VR group in prosthetic satisfaction levels.
Abbas et al. 16 showed that VR is a safe, promising, and amusing intervention for addressing gait in unilateral, traumatic lower limb amputees. Cadence is improved in PT and VR in 4 weeks. In terms of cadence, positive changes were observed in this group. This is thought to result from the increase in performance. The authors thought that motor performance was positively affected. 13
The gait speed of individuals with TT amputation has been increasingly studied more in recent years. Understanding the gait speed differences will direct both the prescribing of prostheses satisfaction and the determination of rehabilitation strategies. Beisheim et al. 34 found that gait speed best predicted increased cadence variability during community ambulation. Sturk et al. 35 described and quantified that VR can be used for transfemoral amputees to maintain stable gait over a variety of surfaces, including downhill and uphill, top and bottom cross-slopes, medial-lateral translations, rolling hills, and simulated rocky surfaces. They concluded that transfemoral amputees adapted to nonlevel conditions by changing their walking speed. When gait speed is considered, it is understood that the performance of the individual improves with positive developments even though it is not significant in the group. PT and VR were found to contribute positively to rehabilitation outcomes.
Tao et al. 36 showed in their current study that the frequency of unsupervised virtual reality home exercises decreased compared with the supervised ones. Therefore, they emphasized that social and clinical guidance features are necessary for continuous lower extremity amputation exergame participation at home.
Limitations
Individuals' duration of prosthesis usage, age range of the amputees, and unable to show the long-term effects of VR are the limitations of this study. In the future, studies with larger sample sizes with double-blind to prevent bias may be done as randomized crossover studies.
Conclusion
VR compared with PT improved balance, performance, prosthesis satisfaction, gait speed, and cadence. So, VR can be an engaging, enjoyable, useful, and motivational adjunct to TT amputation rehabilitation. To our knowledge, there is a lack of studies about VR on amputee rehabilitation long-term outcomes in the literature, and the authors hope that this study will lead the way to further research in this area.
Footnotes
Authors' Contributions
Conceptualization, T.Y.Ş. Methodology, F.E. Software, T.Y.Ş. and F.E. Formal analysis, T.Y.Ş. and F.E. Investigation, T.Y.Ş. and F.E. Resources, F.E. and T.Y.Ş. Data curation, F.E. and T.Y.Ş. Writing—original draft, T.Y.Ş. Writing—review and editing, F.E. and T.Y.Ş. Supervision, F.E.
Ethical Approval
This study was approved by the University Clinical Research Ethics Committee (Decision No: 16/283-38 in 2016). All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Data Available Statement
Data is available upon reasonable request.
Previous Presentation
Any previous presentation of the research, article, or abstract was not published.
Authorship Statement
We assure that authorship has been granted only to those individuals who have contributed substantially to the research or article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
There is no funding for this research.