
Abstract
Objective:
Children with cerebral palsy (CP) present motor learning disorders and somatosensory dysfunction. Although many protocols use videogames in children with CP, few apply or examine motor learning principles. This study aims at (1) implementing therapist–user–designer collaboration in adapting a videogame to the principles of motor learning and the characteristics of users with CP, and (2) piloting the effectiveness of these adaptations by analyzing the achievement of motor learning parameters (learning rate acquisition, retention, and transfer to motor and somatosensory function).
Materials and Methods:
Periodical interprofessional meetings conducted to the adaptation of a videogame, requiring the control of a joystick for traveling through a maze, to motor learning principles. In a pilot validation, effects in unilateral upper limb function, gross manual dexterity, and somatosensory thresholds were assessed before and after 10-week training in 13 children with CP.
Results:
After 10-week training with the adapted serious game, children showed learning rates above 90% and improvement in motor learning parameters along the sessions. Manual dexterity and pronation–supination of the dominant hand improved after training. No significant effects were found on somatosensory thresholds.
Conclusion:
Serious games are useful as motor learning tools for improving motor function in children with PC. Cooperative work among professionals and users is advisable for designing efficient videogames according to rehabilitation best practices.
Introduction
Rehabilitation programs for individuals with cerebral palsy (CP) increasingly use serious games to improve motor performance. 1 Videogaming can be challenging and fun, increasing motivation and promoting children's engagement.2,3 In fact, the use of videogames allows achieving high repetition rates for the required movements, with three times more movements than in conventional therapy.4,5 Videogames require the integration of sensory and motor processing, involving diverse brain networks and making videogame training a potential vehicle for neurorehabilitation of motor skills. 6 The use of videogaming, combined with conventional interventions, has proved effective in improving motor parameters such as upper and lower limb function, balance, gait, postural control, and physical activity in children with CP. 2 In particular, videogaming seems to be effective for the enhancement of different upper limb motor skills, such as grip strength and ability, fine manual dexterity, hand coordination, ability to lift objects, and finger range of motion.2,5,7,8
A recent systematic review reported that Nintendo® Wii-based therapy could represent a clinically relevant intervention in upper motor skills such as grip strength (standardized mean difference [SMD] = 0.5, 95% confidence interval [CI] 0.08–0.91), tip grip strength (SMD = 0.95, 95% CI 0.3–1.61), grasping ability (SMD = 0.72, 95% CI 0.14–1.3), and fine manual dexterity (SMD = 3.12, 95% CI 1.5–4.7). 7 Nevertheless, the transfer of arm and hand improvements to daily activities is controversial and comparative studies have displayed mixed results.5,7,9 Thus, although game-based interventions promote compliance and may potentiate therapeutic gains, mainstream videogames may lack therapeutic relevance due to a fair adjustment to the user's target goals or poor accent on neuroscientific principles.10,11
Motor learning strategies are a proved scientific method for motor rehabilitation in children with CP. 12 Training based on motor learning principles, such as active exploration, high repetition, motor variability, and error experience, enhance rehabilitation outcomes, enhancing accuracy and consistency of motor performance.13,14 Nevertheless, children with CP demonstrate high variability in response to motor training.15,16 The number of errors during practice, the complexity of the task, and the modalities and frequencies of feedback affect the amount of motor learning16,17 and must be taken into account when designing interventions in this population. Videogames can achieve the implementation of motor learning principles, such as high amount of practice, competitive score systems providing feedback and promoting the reduction of errors, and problem-solving requirement, making them effective tools in the training of motor skills in children with CP. 18 Moreover, videogaming has shown to produce an enlargement of spatial activation in some brain motor areas, such as the primary motor cortex and cerebellum, 8 suggesting neuroplastic mechanisms associated with motor learning.
However, few videogames are specifically designed for fulfilling the principles of motor learning and scant studies have explored the efficacy of videogames in the achievement of motor learning parameters.
Motor learning is based on three aspects: skill acquisition, transfer, and retention. 19 However, despite motor learning theory's emphasis on long-lasting changes and generalization, few studies on videogaming evaluate these parameters and their results are contradictory. Although skill acquisition is mostly achieved, it seems affected by motor and cognitive impairment. 20 Furthermore, retention18,21 and transfer to other environments or daily activities5,7,19 are controversial. New approaches to gaming design in collaboration with therapists and children have permitted incorporating relevant motor learning principles to game development, for example allowing adjusting difficulty settings, focusing on movements related to children's goals, identifying compensatory movements or monitoring performance data,11,22 in conjunction with the application of serious gaming principles, such as short-term goals, rewards, and feedback. This collaboration in the game design could modify the unsatisfactory retention and generalization rates obtained by standard videogames in children with CP.
The present study aims at (1) implementing a therapist–user–designer collaboration in adapting a videogame commonly used in rehabilitation of upper limb (i.e., virtual maze) to the principles of motor learning and characteristics of users with CP, and (2) piloting the effectiveness of these adaptations for improving motor learning parameters, such as learning rate acquisition, retention, and transfer to upper limb motor and somatosensory function, after a 10-week videogame training in a small group of children with CP.
Materials and Methods
This study was performed in accordance with the Declaration of Helsinki (1991) and accepted by the Ethics Committee on research of the Balearic Islands (Ref. 3568/2015).
Collaborative videogame adaptation to principles of motor learning
Participants
A collaborative team was formed by researchers from the group Computer Graphics, Computer Vision and IA-DMI (http://ugivia.uib.es), and the Institute of Health Sciences Research (University of the Balearic Islands), together with teachers, physiotherapists, and children with CP from the Foundation Aspace-IB. The team was composed by the following professionals and users: 3 engineers, 1 doctor, 3 physiotherapists, 4 teachers, 13 children with CP. Children with CP who could not attend to the meetings gave their feedback through their teachers and were interviewed personally by a member of the research team in each phase of the adaptation.
Children diagnosed with CP were recruited from Fundación Aspace-IB, a CP foundation devoted to education and therapeutic activities in Majorca (Spain). Inclusion criteria were: diagnosis of CP, age between 8 and 18 years, cognitive level sufficient for following simple instructions (e.g., ability to understand the game basic rules). Exclusion criteria were: recent or programmed surgery in the upper arm, botulin toxin injections in the upper arm previous or programmed during the intervention, severe visual impairment, and severe cognitive impairment. Thirty-two potential participants were identified by the center manager and were invited with their parents to a meeting for providing information about the study.
Thirteen children agreed to participate in the game development and, subsequently, in the validation pilot study (age = 13.84 [3.58] years., 5 females). Parents signed informed consents and children provided their verbal approval to participate. Figure 1 displays a flow diagram of the children with CP participation in the different parts of the study.
Flow diagram of the participation of children with cerebral palsy.
Procedure
Periodical team meetings were conducted in the Foundation Aspace-IB, with the following discussing topics:
Necessities and objectives discussion. How to achieve these needs with motor learning interventions, how implementing them to the videogame and how to adapt the software for learning parameters' registration. Assessment of technical capabilities of the center computers. Adaptation of suitable software. Videogame technical testing and corrections. Videogame content design and adaptations. Videogame adaptation to users' capabilities. Agreement in a final version for piloting.
Each discussion session was followed by the implementation of the agreed suggestions and modifications, which were tested and modified until the achievement of the session goals. At the following session, results were reported, and new ideas were discussed.
Effectiveness of the adapted videogame for improving motor learning parameters
Participants
Children with CP that had participated in the discussions and tests for adapting the videogame (age = 13.84 [3.58] years., 5 females), completed 10 weeks of videogame training added to their conventional rehabilitation intervention. Demographic and clinical data were extracted from the clinical history (Table 1).
Demographic and Clinical Data of Participants
Videogame training
A virtual maze game, a classic videogame used in the rehabilitation of children with CP, 23 was selected for training upper limb function. The game consisted in moving a spherical object through the maze using a joystick paddle with the dominant hand. After a first phase dedicated to the adaptation of the videogame to motor learning principles, children performed 10 sessions of training, added to their usual rehabilitation treatment. Sessions were individual and were performed by a trained therapist from the center in a quiet and adapted room. Every participant performed one 30-minute session per week. After adjusting chair and table to the children's needs, children were only instructed to move the ball with the joystick for finding the maze exit. Children could progress to the next difficulty level only if they completed the maze in a due time, which was increased along the difficulty levels, giving the children more time for completing longer and more difficult mazes. If the maze was not successfully completed in that time, the screen was restarted in the same level screen until the participant completed the maze.
Assessment
Motor learning acquisition and retention
The videogame software stored the following performance variables for each trial: TIME (in seconds), PATH (distance in cm), and the number of COLLISIONS (errors). For further analyses, these variables were grouped by session (from session 1 to session 10) and level of difficulty (from level 1—the easiest—to level 10—the most difficult). Motor learning is operationally defined as a shift in the speed/accuracy trade-off, characterized by an increase of velocity and/or a reduction of errors (increment of accuracy).24,25 In our case, motor learning would be reflected by a reduction in time, collisions (errors), or distance (a straighter path, indicating higher accuracy). For displaying the trade-off among these variables, a new variable PERFORMANCE was calculated with the combination of the values of the TIME and COLLISIONS applying the formula [TT × (C + 1)]. According to this formula, a lower value of PERFORMANCE (less time or errors) would indicate higher learning. This formula has been previously used for evidencing motor learning after training in populations with stroke and CP.26,27
Transfer of motor learning
Transfer of motor learning to different environments was explored by the assessment of sensorimotor items before and immediately after the videogame training. To control that transfer was related to the videogame training and not to the usual rehabilitation, 13 additional children not participating in the training and matched in age, sex, and severity with the participants were assessed with the same tests in two time periods separated by 10 weeks. The assessment was performed by a member of the research team different to those related to the game development or training. To avoid anxiety, participants were allowed some time for familiarizing with the material and were accompanied by their teacher during the assessment. Following other transfer studies, 19 two tests of ability and performance of the upper arm were bilaterally assessed. With the aim to explore potential somatosensory effects of motor training, 28 two sensitivity tests were carried out.
Gross manual dexterity for each upper limb was assessed using the Box and Block Test. Each participant was instructed to pass over as many cubes, one by one, from one side to the other of a 100 mm center barrier for 60 seconds. Only the cubes that crossed over the barrier were counted. When more than one cube was transferred in a single movement, it was counted only as one unit. This test shows strong correlations with the performance of daily activities, and it is considered a reliable tool for examining changes after rehabilitation interventions in children with CP. 29
Upper limb unilateral function was assessed with a modification of the Melbourne Assessment of Unilateral Upper Limb Function, a reliable tool for measuring the quality of unilateral upper limb movement in children with CP. 30 The test is based on motor exercises such as manipulation, pronation/supination, transference, grip, and reach. The original test is composed of 16 tasks that are videorecorded. The final score is obtained by adding the score from each task and dividing it into the highest possible score. Following other studies, 19 we selected the four tasks more closely related to the videogame-targeted goals (i.e., reach forward, grasp of crayon, release of crayon, pronation/supination). These tasks reflect movements used in common daily functions such as eating or washing.
Somatosensory assessment was determined bilaterally and randomly in four locations: index finger, thenar eminence, hand dorsum, and dorsal forearm. Three measures were performed, and the mean was taken as the score for each location. Tactile thresholds were estimated by the application of von Frey monofilaments following the method of limits. The participants had to indicate yes/no, depending on if they felt the perception of being touched. Pressure pain thresholds were assessed with a digital algometer with rubber tip (1 cm2). Participants had to inform when the sensation was uncomfortable. Previous studies have shown the usefulness of these instruments to measure somatosensory sensitivity and its changes in children with neurodevelopmental disorders.31,32
Mathematical and statistical analyses
Motor learning was explored by the mathematical calculation of the learning rate and the learning curve along the 10 sessions of training. The use of a logarithmic model produces learning curves tending to decrease, approaching to 0 (Y = 0). Calculations were performed using the linear equation Log (Y) = NLog(x) + (K), where Y = mean of scores/session until the present session, N = learning rate, K = score in the first session, and x = score in the session. The learning curve would be the result of the formula (Y = K.xN). Changes in x and N allow predicting the variable behavior in future potential sessions.
Descriptive, Chi-square and t-tests were used to describe and compare demographic and clinical variables between the children performing or not performing the training. Two-way analysis of variance were performed with the between-subject factor GROUP (training vs. no-training) and within-subject factor TIME (pretraining vs. posttraining) in these assessments. Comparisons were made separately for the dominant and the nondominant hand. The magnitude of the change in comparisons was interpreted using the effect sizes following the guidelines proposed by Cohen (1988), 33 defining the magnitude of the change as not significant (<0.2), small (0.2–0.49), moderate (0.5–0.79), or large (>0.8). Bonferroni adjustments were made for multiple comparisons. Significance level was set at P < 0.05.
Results
Collaborative videogame adaptation to principles of motor learning
The collaborative team mentioned above cooperated in the videogame adaptation to principles of motor learning by sharing needs, discussing solutions, selecting objectives, and monitoring all the phases of the design, implementation, and evaluation. A virtual maze game, classically used in the rehabilitation of children with CP, 23 was selected for training upper limb function. The videogame consisted in moving a spherical object through the maze until the exit, by the use of a joystick paddle adapted to the needs of each participant. The videogame was developed in a Windows software, easy to run in the center computers and was programmed for saving the performance of each participant in every trial. Videogame modifications were made in an iterative fashion based on observations from children and clinical team members. Professionals incorporated principles of motor learning to the game, designing a game of 10 screens with increasing levels of difficulty on the maze resolution and required movements, reduction of therapist feedback (explicit learning) and increasing of feedback provided by the game, highlighting errors or giving scores of total time (implicit learning).
Users introduced feedback elements in the last levels, highlighting collisions with bomb explosions or introducing awards with the achievement of the goals. Pretests were used for ensuring technical stability in the center computers and adapting the game to the performance of users with CP, reducing the difficulty in the starting levels and increasing the amount of time allowed for finishing the maze. In the final version, there were no safety issues or technical flaws.
Effectiveness of the adapted videogame for improving motor learning parameters
Motor learning acquisition and retention
A descriptive analysis of the task performance parameters (TIME, PATH, COLLISIONS, and PERFORMANCE) showed an increment of scores along the maze levels, revealing lower accomplishment as mazes increased in complexity and confirming that the game offered a progressive difficulty (Fig. 2). The parameters, PATH and COLLISIONS, evolved parallel. The average time for completing the maze varied between 10 seconds for the first level, <30 seconds for half of the easiest levels, and almost 1 minute for the most difficult levels; thus, all the mazes could be finished before the due time.
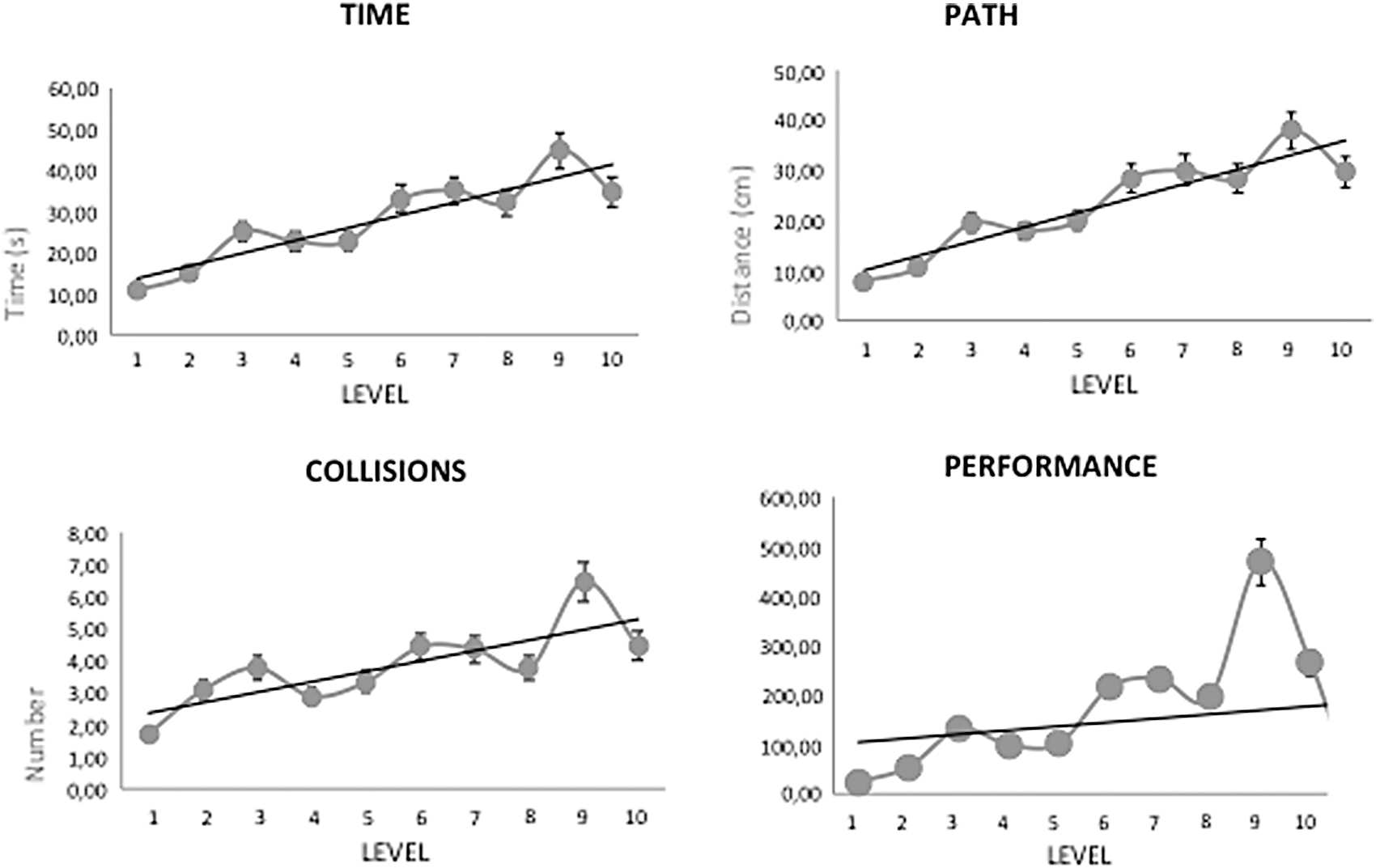
Time, path, collisions, and performance in the different difficulty levels.
The analysis of the parameters through the sessions displayed a fluctuating pattern, globally representing a decrease in TIME, PATH, COLLISIONS, and PERFORMANCE from session 1 to session 10, thus indicating successful motor learning (Fig. 3). The parameter PERFORMANCE (time/accuracy trade-off) exhibited a peak in session 6, induced by the low rate of COLLISIONS (but not of PATH or TIME) in that session. Thus, although TIME showed a progressive reduction throughout the sessions, both PATH and COLLISIONS showed a peak differing scores in the first session and in the last session. These pattern changes occurred before in the reduction of PATH (session 4) than in the reduction of COLLISIONS (session 6).
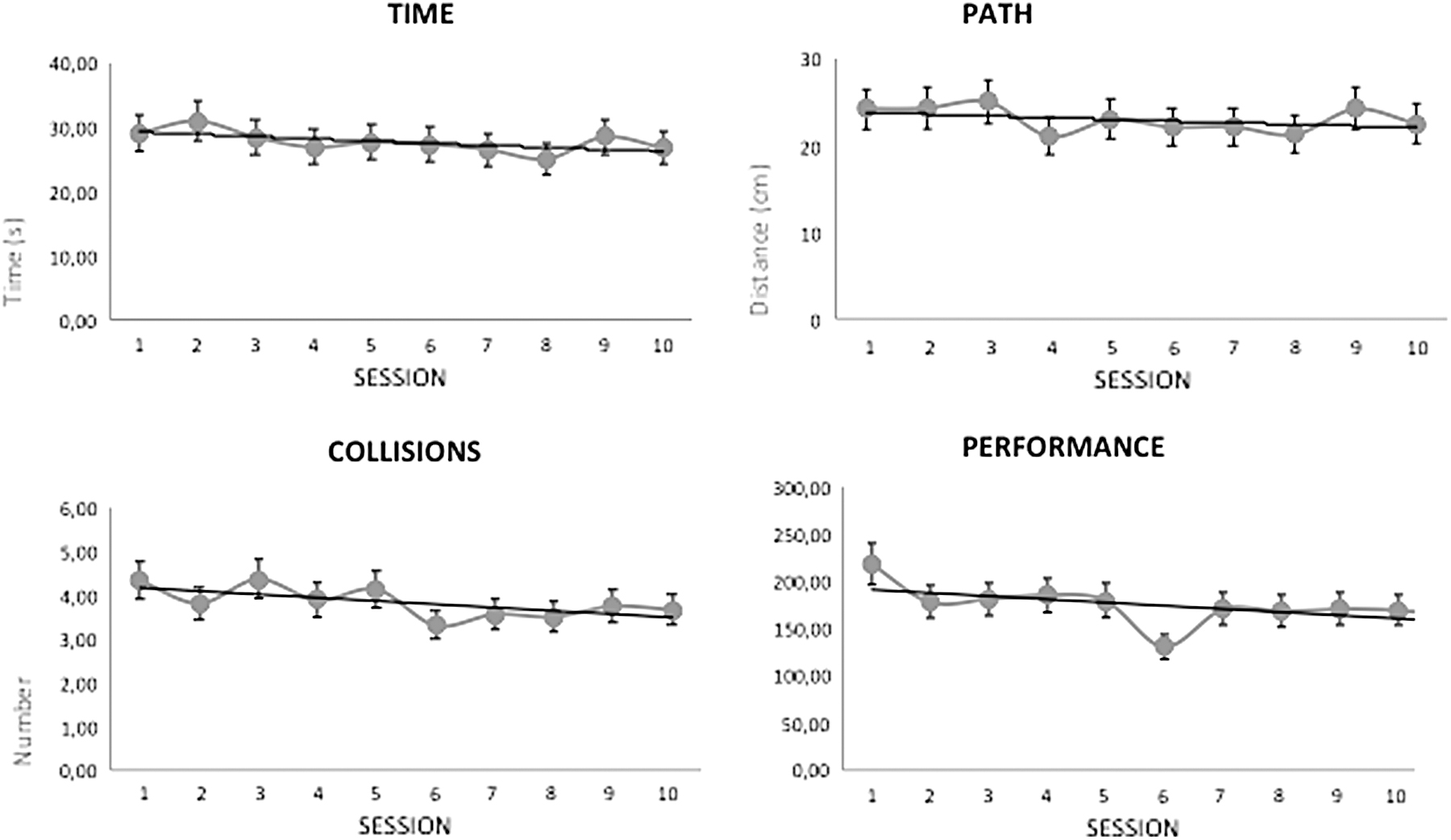
Time, path, collisions, and performance in the different training sessions.
The linear equation 2^N displayed learning rates over 90% for all variables (Table 2). Logarithmic learning curves (Fig. 4) showed a tendency to decrease through the sessions for all variables (approach to Y = 0, indicating learning).
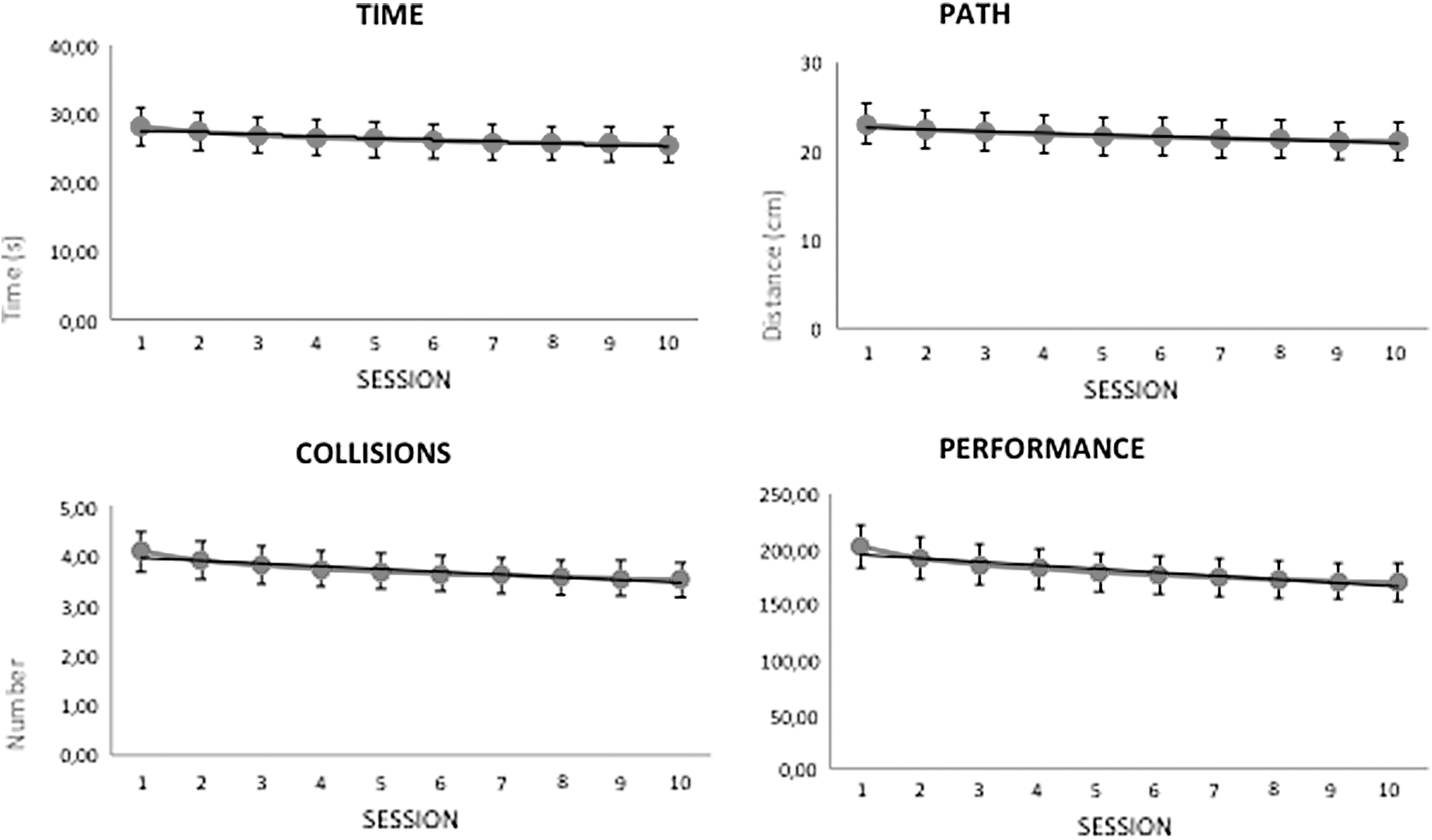
Learning curve for each variable (time, path, collisions, and performance) along the different training sessions.
Formula for the Calculation of Learning Rate and Learning Curves of the Different Motor Learning Outcomes: Time, Path, Collisions, and Performance
As the learning curves showed a tendency to a plateau in the last sessions that might indicate stabilization in the acquisition of knowledge, a projection of the variable PERFORMANCE was applied to potential sessions 16 and 32 to analyze what would have happened if training had been continued up to that point (Fig. 5). The curve shows a continuous decreasing (indicating greater learning) with a progressive stagnation until session 32.
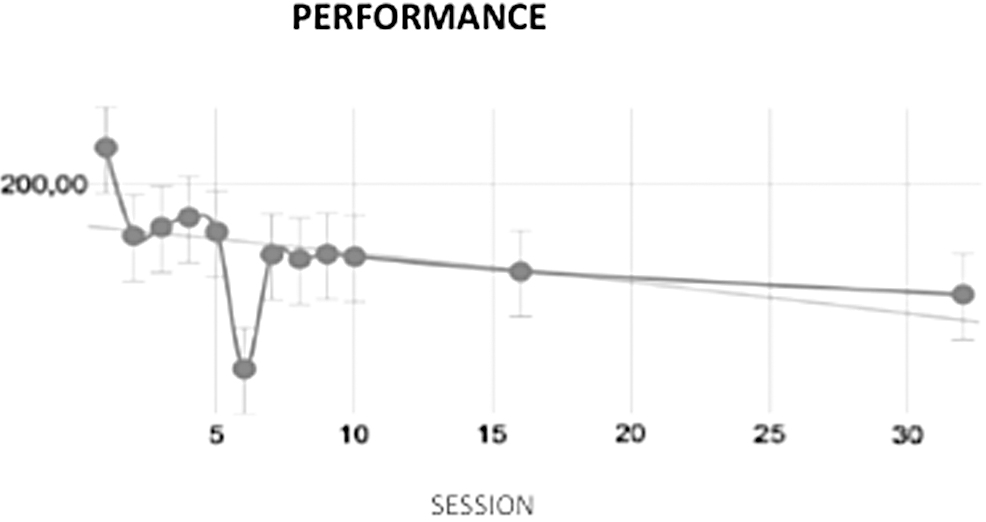
Projection of the PERFORMANCE learning curve until potential session 32.
Generalization of motor learning
Children not performing the training, who were included for the evaluation of the transfer of motor learning, did not differ significantly in age, gender, laterality, and fine or gross motor function from children performing the videogame training.
The Box and Block test for the dominant hand (the one that moved the joystick) showed a significant TIME × GROUP interaction [F(1,24) = 7.16, P = 0.011]. Post hoc comparisons indicated that children who had performed the videogame training scored higher in the posttraining than in the pretraining (P = 0.042, Cohen's d = −0.12), whereas scores after 10 weeks did not change in children not playing the videogame (P = 0.092). No significant main effects of GROUP or TIME were found. No significant effects were revealed on the nondominant hand.
Regarding the four tasks assessing upper limb unilateral function, effects were found in two tasks (i.e., Reach forward—assessing the mobility, precision and fluidity of the trunk, shoulder, elbow, and wrist—and Pronation/Supination—forearm mobility). Both tasks showed a significant TIME effect for the dominant hand (both F > 5.49, both P < 0.029) with higher scores in posttraining in comparison with pretraining. Furthermore, the task Pronation/Supination showed a significant TIME × GROUP interaction [F(1.21) = 4.55, P = 0.045] indicating higher scores in the posttraining compared with pretraining only in the children who played the videogame (P = 0.002, Cohen's d = −2.82), whereas children who did not play showed no significant changes after 10 weeks (P = 0.072). There were no significant effects for the nondominant hand or for the tasks Grasp and Release of crayon.
No significant effects were found on somatosensory measures of tactile or pressure pain thresholds.
Discussion
The objective of this study was to explore the efficacy of a videogame task in improving motor learning of the upper limb in children with CP. The training with this videogame, added to the conventional rehabilitation sessions, produced acquisition and retention of the task, with more modest results in generalization of motor skills to daily life environments.
This study engaged children, therapists, researchers, and engineers in a user and goal-centered approach. The final videogame incorporated principles of motor learning that have proven effective in children with CP. Moreover, the system allowed recording children's performance data based on the operational parameters of the speed/accuracy trade-off. 24 General features, such as friendly interfaces, simple instructions, or ergonomic accessibility are essential for game engagement.34–36 The participation of users in the design and development allowed adapting videogame features to their specific needs, achieving a tool adaptable to multiple cognitive and motor impairments. 36 Moreover, it was safe, technically reliable, and feasible for use in a low-tech clinical setting. As in previous experiences,11,22 joint clinical–user–engineer work in serious game development has resulted in a videogame friendly and therapeutically relevant for children with CP.
Training with the videogame produced high learning rates (higher than 90%) and a decrement of the learning curves along the sessions that would indicate motor learning acquisition and retention. However, the projection to future potential sessions revealed that continuing the training would have produced higher learning. Videogaming dosage is still an unresolved question. Studies vary in the number of training weeks from 8 to 16, with different number of sessions into the week.5,37 Furthermore, cognitive and motor impairment may determine the extent in what children with CP modify muscle activity to accomplish the game demands, 20 and consequently, the amount of practice required for learning acquisition. Future research is warranted to establish clinical protocols for achieving optimal motor learning, considering individual characteristics, in line with person-based medicine.
In our study, there seem to exist transfer of motor learning to motor abilities of the hand that guided the joystick, although transfer to more complex motor skills required in daily living, such as reaching, grasping, and releasing or to somatosensory parameters was not attained. Although the use of videogaming combined with conventional rehabilitation interventions has proved effective in enhancing multiple motor skills in children with CP, 9 previous studies have already pointed to the difficulties in generalization of the acquired motor skills to daily environments.5,19 The videogame movement range was restricted to small movements of the joystick and only this hand was active in the videogame, minimizing the use and concomitant plasticity of the nondominant hand and bilateral activity, what are crucial for daily life activities. Therefore, our effect sizes are discrete and in very specific movements, in contrast with other videogame interventions for upper limbs. 7 More active and global gaming should have produced better generalization and must be explored in future research.
Some limitations, such as the small and heterogeneous sample, the lack of follow-up or the absence of assessments for objectively measuring enjoyment could have been causes of bias. Nevertheless, this study may be worthy as a preliminary experience for implementing user–interprofessional collaboration in the development of serious games, showing aspects to replicate or to improve in the future design and implementation of therapeutic technology in children with CP.
Conclusions
Interprofessional–user collaboration can design safe and flexible serious games incorporating principles of motor learning that can be useful as complementary therapies in children with CP. Further research establishing the optimal dosage and goal-related games would allow optimizing protocols for incorporating serious games to the clinical practice.
Footnotes
Acknowledgments
The authors acknowledge the participation of the students of the CEE Pinyol Vermell from the Fundación Aspace. The collaborative teamwork was coordinated by Cecilia Nicolau (teacher of the CEE Pinyol Vermell from the Fundación Aspace) and Diego Bautista (member of the research team).
Author Disclosure Statement
The authors report no conflicts of interest.
Funding Information
This research was funded by the grant PID2020-114967GA-I00 funded by MCIN/AEI/10.13039/501100011033 to I.R. Also, this research was funded by the Ministerio de Economía, Industria y Competitividad (MINECO), the Agencia Estatal de Investigación (AEI), and the European Regional Development Funds (ERDF, EU) for its support to the project TIN2015-67149-C3-2-R (MINECO/AEI/ERDF, EU), PERGAMEX RTI2018-096986-B-C31 (MINECO/AEI/ERDF, EU), and PID2019-104829RA-I00/AEI/10.13039/501100011033 (MICINN).