
Abstract
Objective:
This study aims at comparing the energy expenditure (EE) and heart rate (HR) data from Ring Fit Adventure (RFA) with those from indirect calorimetry (COSMED) and a heart rate monitor (Polar FT7). A secondary goal is to evaluate self-reported enjoyment and perceived effort levels.
Materials and Methods:
Thirty participants (age = 21.8 ± 2.2; body mass index = 31.8 ± 4.4) were recruited for two laboratory visits. The first visit involved baseline measurements. In the second visit, participants performed a 55-minute ad libitum exercise session with the RFA in adventure mode with moderate difficulty. During this session, EE, HR, perceived effort, and enjoyment of physical activity were recorded.
Results:
Although no statistically significant overestimation of EE was found between the RFA and the metabolic cart, two-way analysis of variance results show a main effect of condition (RFA vs. Polar FT7) on HR (122.8 ± 20.1 bpm and 129.0 ± 18.6 bpm; P = 0.007; ᶯp2 = 0.235). Based on comprehensive statistical evaluations, including the mean absolute percent error, intraclass correlations, typical error of measurement, and limits of agreement, the data suggest that the RFA provides reliable estimates for EE and HR. Overall, participants enjoyed the game considerably (71.3 ± 5.9/80 arbitrary units), and their reported perceived exertion was low.
Conclusion:
This study underscores that the RFA values are relatively accurate and precise, and thus it can be safely suggested for individuals with overweight and obesity to adopt an active lifestyle.
Introduction
Epidemiological data indicate that there has been a substantial increase in overweight and obesity worldwide (OW/OB).1–3 In Latin America, Mexico presents one of the highest indices. Approximately 73% of the population is at least OW and 36.1% OB.4,5 It is estimated that by 2050, the cost of Mexican health care for OW/OB will be around $1.7 billion. 6
Higher values of body mass index (BMI; defined as weight in kilograms divided by height in meters squared) involve serious consequences, including cardiovascular disease and diabetes,7,8 cancer, 9 and a steeper decline in cognitive abilities. 10 More precisely, in Mexico, comorbidities (e.g., diabetes and hypertension) associated with OW/OB have accounted for an increase in mortality rates, premature death, and/or disability. 11 Therefore, finding methods to reduce the incidence of OW/OB will be critical in the coming years.
Regular physical activity (PA) has been identified as an effective method to impact body weight and reduce OW/OB levels. PA is generally defined as any voluntary body movement that requires greater energy expenditure (EE) than resting. 12 The Physical Activity Guidelines for Americans state that adults must engage in 150 minutes of moderate, or 75 minutes of vigorous PA or an equivalent combination of two intensities per week.12,13
In Mexico, the past 12 years have driven the population to a significant reduction in PA levels, accompanied by an increase in sedentary time, 14 despite efforts of the government to implement multiple programs (e.g., “Chécate, Mídete, Muévete,” and “Pausas por la Salud”) tailored to reduce time spent in such behaviors.15,16 A recent study identified the most frequently perceived barriers by OW/OB people to engage in PA or exercise, which include a lack of time and/or motivation, dislike of PA/exercise, and lack of a safe and adequate space to exercise. 17 Concerning this matter, one possible strategy to attenuate the levels of inactivity would be to promote new, enjoyable, and home-based activities that might aid with habitual exercise engagement, such as exergames.18,19
Currently, videogames enjoy widespread popularity across all age groups.20,21 This surge is largely attributable to their evolution from wired, static consoles, which limit embodied interaction, to sophisticated, dynamic systems that enable players to perform more realistic movements and engage with a global player base. These pivotal advancements in console technology have positioned active videogames as a promising strategy to bolster PA levels during an era where sedentary and/or physically inactive lifestyles are prevalent and have been associated, among other health issues, with weight gain and increased adiposity.22–24
Exergames are videogames in which people are required to use their body and gross motor movements to interact with the main character or images on the screen. Different movement patterns may be required depending on the game or modality, but are usually composed of aerobic, and/or strengthening, and/or balancing movements.25,26 The combination of these three important components (i.e., aerobic, strength, and balance) promotes higher levels of EE that are associated with partially reducing weight and adiposity, while simultaneously increasing enjoyment and adherence.25–29
Several studies have examined the benefits of exergames in healthy children and adolescents with OW/OB or healthy older adults19,25,28,30,31; however, evidence to sustain the possible effects on OW/OB healthy young adults is scarce. 32 Some studies have suggested that adults 18–35 years of age can reach up to 1000 kcal/week playing exergames with at least 30 min/day, five times a week.33,34 In addition, significantly higher values in maximal oxygen consumption (VO2max) have been reported after comparing a boxing exergame with a light walk (but not a brisk walk on a treadmill). 35
From a psychophysiological viewpoint, no differences in the rating of perceived exertion (RPE) were found after participants played with an interactive cycling video and traditional cycling, even though they selected a higher intensity in the game compared with the traditional one,36,37 leading to more kcal spent engaging with the former. 37 An improvement in enjoyment during and after playing with exergames has been consistent across different ages, and in OW/OB people.18,20,26,38,39 Enjoyment enhancement is one of the main components that can help to increase exercise adherence.40,41
Several mechanisms have been proposed to moderate/mediate these effects such as endorphin release, endocannabinoids (i.e., lipid mediators isolated from the brain and peripheral tissues), among others.42–44 Undoubtedly, such reductionistic molecular mechanisms have partial explanatory power. However, we suggest a more comprehensive biopsychosocial position be adopted to focus on the right level of analysis to best explain the phenomena at hand.
Several components found in exergames can reduce the likelihood of a lack of interest, while simultaneously increasing intrinsic motivation, enjoyment, and adherence to PA/exercise. Among them are novelty or even variations to a familiar stimulus.45,46 Exergames have been gaining more attention over the years as a tool to sustain higher PA levels because they allow for individualization and adaptivity to the individual's current physical abilities.47,48
One of the recent exergames, the Ring Fit Adventure (RFA), developed by Nintendo for the Nintendo Switch, uses a resistance ring to exercise the upper body and a leg strap with an accelerometer to sense the movement of the player, which moves the digital avatar accordingly. As the player advances in the game, there is a concomitant increase in intensity and hence, difficulty of the exercises. Only one study in OW/OB has used the RFA. 39
The authors found that the RFA was the second exergame—the first one being BKOOL—that spent more kcal/min in children. Moreover, the RFA is equipped with a mechanism that records heart rate (HR) and kcal/min and provides a summary of such metrics at the end of a game. However, no previous study validating these measurements has been conducted in individuals with OW/OB. These values turn out to be relevant considering reported associations between kcal spent in exercise and lower indices of OW/OB. 39
To the best of our knowledge, no study to date has corroborated the possible physiological (i.e., kcal) and/or psychological (i.e., RPE and enjoyment) advantages that the use of exergames may have in people with OW/OB in Mexico. Therefore, the main purpose of this study is to compare the EE and HR provided by the RFA to gold-standard and validated measures (indirect calorimetry [COSMED]; heart rate monitor [Polar FT7], respectively).
The secondary objective is to report levels of enjoyment and RPE, given that there is no way to objectively quantify those besides self-report. Based on the previously cited literature, we expect the RFA's EE and HR to be relatively accurate and precise when compared with gold-standard/validated measures. In addition, given the combination of multisensorial immersion with the ability to auto-regulate one's pace, we hypothesize that participants will report high levels of enjoyment and progressively higher levels of exertion throughout the game (i.e., progressively higher RPE).
Materials and Methods
Power analysis
An a priori power analysis with data from six participants was computed to calculate the sample size using a repeated-measures t-test. A total sample of 30 participants was estimated for the study, using the following settings: Cohen's d effect size of 0.47, 49 with an alpha level of 0.05, power at 0.80.
Participants
Anthropometrics, body composition, and fitness parameters of participants are summarized in Table 1. The participants included 30 male volunteers with OW (n = 13) and OB (n = 17) recruited by advertisements on the Autonomous University of Baja California in Tijuana, Mexico. Convenience sampling was used to recruit participants. The age range was from 19 to 28 years (age 21.8 ± 2.2 years). The inclusion criteria were (1) having a BMI >25 kg/m2, (2) normal or corrected to normal vision, (3) not having a prior history of neurological illness (e.g., stroke or Parkinson's disease), (4) not having a history of head injury, and (5) not having any physical impairments that would prevent them from engaging in exergames. Participants with previous experience in the RFA were excluded.
Anthropometrics, Body Composition, and Fitness Parameters of Participants (n = 30)
BMI, body mass index; EE, energy expenditure; HR, heart rate; HRmax, maximal heart rate; MC, metabolic cart; PhA, phase angle; RFA, Ring Fit Adventure; RPE, rating of perceived effort; VO2max, maximal oxygen consumption.
This study was performed in accordance with the ethical guidelines of the Helsinki Declaration and were reviewed and approved by the Teaching Support and Research Department from the Autonomous University of Baja California, under the IRB approval ID P-01-2023-1.
Procedures
All participants were informed of the study's nature and risks before giving written consent. They attended two sessions at the Human Motor Biosciences Laboratory, Autonomous University of Baja California, Sports Faculty. During the first visit, body weight, body fat, muscle mass, and phase angle (PhA) were measured using a bioimpedance scale (InBody 770; Seoul, Korea). Height was recorded with a stadiometer (InBody BSM, Seoul, Korea).
A graded exercise treadmill test (Bruce Protocol) was conducted on a treadmill (COSMED T200, Rome, Italy) to determine kcal/min, maximal heart rate (HRmax), and VO2max using a metabolic cart (COSMED, Quark CPET model, Rome, Italy). 50 A player profile and ring calibration for the RFA were set up. The bioimpedance assessment was performed fasted following the standardized protocol of the American College of Sports Medicine. 51 One night prior, subjects were asked to refrain from food or diuretic beverages (e.g., caffeine, energy drinks, alcohol, caffeinated tea, among others), engaging in moderate or high PA, and were asked to drink a minimum of 1.5 L of water for proper hydration.
In the second session, participants' HR (Polar FT7) was monitored for 10 minutes while lying supine. Their HR and RPE were then recorded, 52 and they were connected to the metabolic cart before starting the RFA to track HR and kcal/min. They played the game at their chosen intensity for 55 minutes, starting from the game's first stage. HR and RPE were recorded every 5 minutes. After 55 minutes, a 5-minute cool-down was done, and HR and RPE were recorded again (Fig. 1).
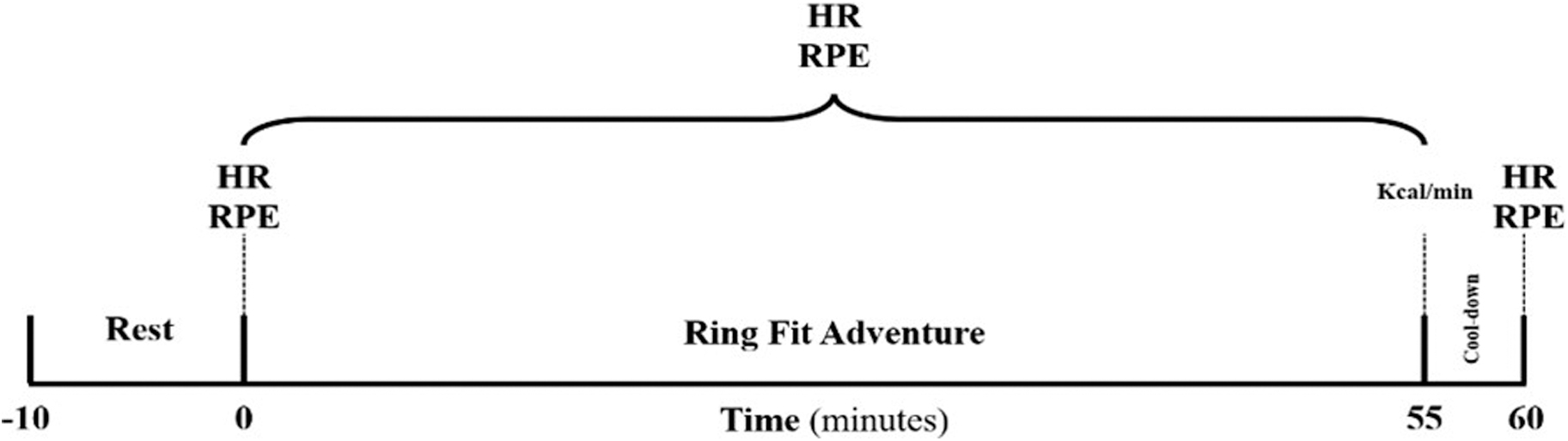
Exergame protocol for the RFA. HR and RPE were collected at the start (0 minutes) and after cool-down (55 minutes), as well as every 5 minutes during the RFA exercise period. Kcal/min was only collected at the start of the cool-down period. HR, heart rate; RFA, Ring Fit Adventure; RPE, rating of perceived effort.
RFA is an action role-playing videogame. It consists of multiple physical movements (jogging, squat, overhead press, knee-to-chest, chair pose, front press, knee lift, among others), using the ring-con and the leg strap. The purpose of the game is to defeat a series of villains that increases the game level and unlocks more intense exercises. The videogame provides several game modes. However, for this study, we decided to choose the adventure mode.
The adventure mode has four difficulties: casual (i.e., low intensity), moderate, intense, and extreme (i.e., high intensity). This game mode was assisted by an avatar who explained the exercises. Two researchers were inside the room the whole session assisting participants. Importantly, all participants were new to this videogame, which they engaged in individually.
The RFA provided the kcal/min spent after the 55 min based on the movement captured via the Joy-Con controllers (i.e., the Nintendo Switch controllers). HR was assessed by the Joy-Con's infrared motion camera after completion of each level by the participant. These two values were used for comparison with the ones obtained by the metabolic cart and the Polar FT7, respectively.
Subsequently, subjects completed the Physical Activity Enjoyment Scale (PACES) questionnaire. 53 This scale was used to assess the level of enjoyment of the RFA using participant responses to 16 questions scored on a 1–7 Likert scale, ranging in score from a minimum score of 16 (does not enjoy the activity at all) to a maximum score of 80 (full enjoyment of the activity). To obtain the level of enjoyment, 54 all values were summed (reverse-scoring for negative items) and a score between 16 and 80 was calculated.
Statistical analyses
Normality was assessed via histogram, quantile-quantile plot (Q-Q plot), and Shapiro–Wilk test. Outcomes are expressed as mean ± standard deviation. Descriptive statistics were generated for participant baseline characteristics (e.g., age, height, weight, body fat percentage, PhA, maximal oxygen consumption, EE, HR, RPE, and enjoyment of PA; Table 1).
The validation of the RFA will be established through the following statistical analyses:
The Mean Absolute Percentage Error (MAPE) measures the average error between the validated devices (metabolic cart and HR monitor) and the RFA, indicating the accuracy of EE and HR measurements. The Intraclass Correlation Coefficient (ICC) gauges the consistency of EE and HR readings between the validated methods and the RFA. The correlation coefficient will be interpreted as very low (≤0.19), weak (0.20–0.39), moderate (0.40–0.59), strong (0.55–0.79), and very strong (≥0.80).
55
The Typical Error of Measurement (TEM) and the Limits of Agreement (LoA) from Bland–Altman plots are both utilized to assess the precision of EE and HR measurements made by the RFA, in comparison to validated measures (indirect calorimetry [COSMED]; HR monitor [Polar FT7]). However, they serve distinct purposes. TEM is specifically focused on quantifying the magnitude of measurement error. It is calculated using the standard deviation of the differences between related measured methods, divided by the square root of 2. The TEM values are then categorized based on their magnitude: good (<5%), moderate (5 to 9.99%), or poor (≥10%). On the other hand, LoA in Bland–Altman plots provide a range within which most differences between the RFA's measurements and the validated methods are expected to lie. This range helps in understanding how closely the RFA's measurements agree with the standard methods over repeated trials. The LoA thus offers a more comprehensive view of measurement consistency and potential variability. In addition, a two-way analysis of variance (ANOVA) (conditions × BMI groups) was performed for EE and HR to identify if there were group-level differences. Main effects were analyzed with the Bonferroni post-hoc test. EE was calculated based on total calories measured by the metabolic cart divided by effective playing time during the session. Effect sizes (partial eta squared [ᶯp
2
]) were reported for OW, OB, and the total.
Results
All data were analyzed using the Statistical Package for Social Science, version 23.0 (IBM Corp, 2015). A 68.5% HRmax was measured during RFA, which represents a moderate intensity (130.3 ± 25.3 bpm) (Fig. 2; Table 1). Participants increased their EE rate by ∼6.9 ± 1.5 kcal/min. A relatively low RPE was reported across the entire session (11.8 ± 3.4) (52), meaning that the participants perceived an effort of 45% (Fig. 2).
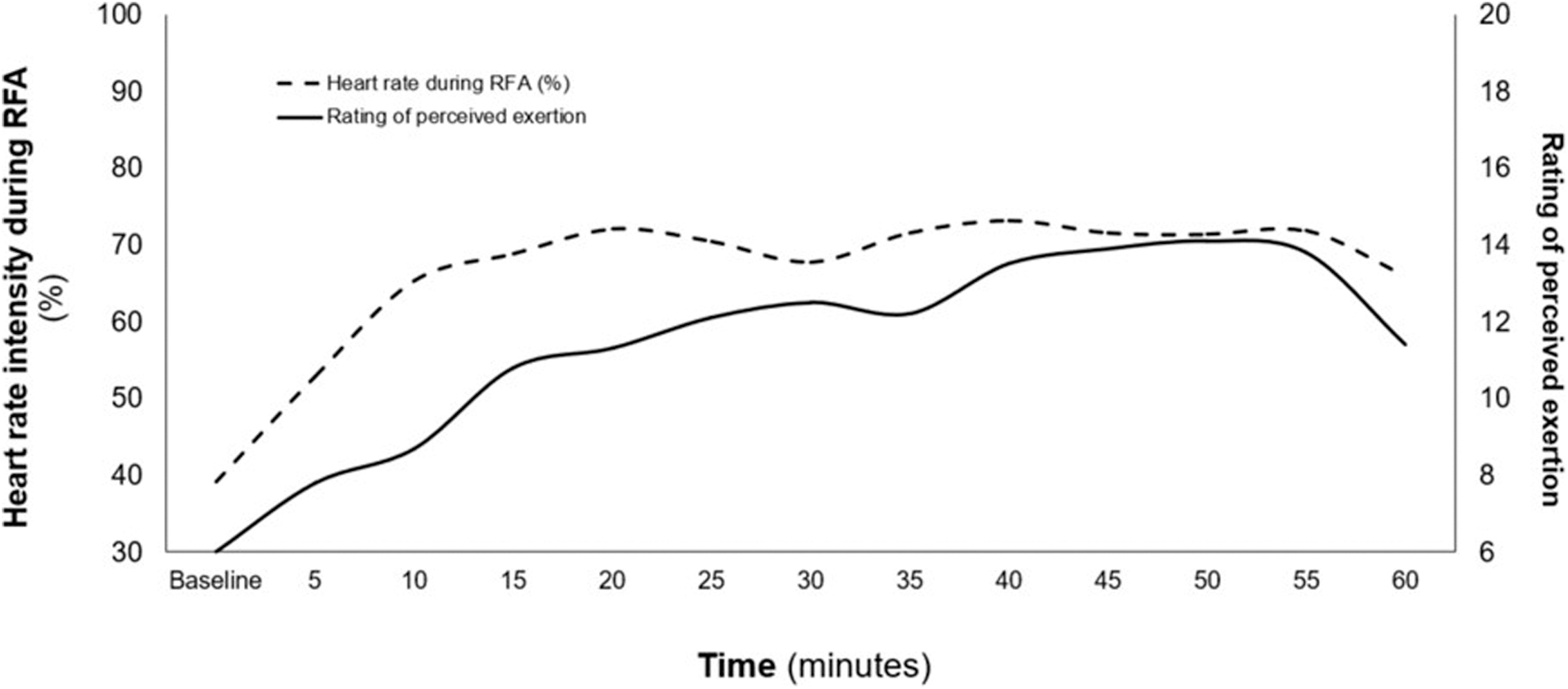
Heart rate intensity and rating of perceived effort during the 60-minute session.
The enjoyment score reported through the PACES questionnaire was very high (71.3 ± 5.9). There were no significant differences (mean score OW = 71.8 ± 5.9; mean score OB = 70.9 ± 5.9; P = 0.688) between OW and OB participants. A low MAPE was found, suggesting accurate EE estimations by the RFA videogame compared with the metabolic cart (10.8%), and HR measurements closely matched those of the Polar monitor (7.7%).
ICC revealed a very strong correlation for EE between RFA and the metabolic cart in individuals with OW (r = 0.839; P = 0.001) and OB (r = 0.815; P = 0.001), indicating high reliability between measurements in these groups. The ICC for HR also indicated a strong agreement with the Polar monitor across all groups (r = 0.832; P = 0.001 and r = 0.820; P = 0.001; for OW and OB, respectively). The TEM was considered poor for EE (16.6%) but moderate for HR (8.1%), with a moderate coefficient of variation for both EE and HR, suggesting some variability in the measurements.
However, the Bland–Altman LoA demonstrated consistent variance around the mean difference for both EE and HR, indicating that, despite noted differences, both instruments can provide comparable HR and EE estimates.
The two-way ANOVA shows no significant differences in the interaction term (F = 1.333; P = 0.258; ᶯp 2 = 0.45), main effects of condition (F = 3.584; P = 0.069; ᶯp 2 = 0.113), or BMI category (F = 2.230; P = 0.147; ᶯp 2 = 0.074) on EE. Similarly, there were no significant findings in the interaction term (F = 0.104; P = 0.749; ᶯp 2 = 0.004) or in the simple effects of BMI categories (F = 0.034; P = 0.854; ᶯp 2 = 0.001) on HR. However, a main effect of condition (F = 8.599; P = 0.007; ᶯp 2 = 0.235) on HR was found.
Discussion
This study provides early evidence regarding the validity of the RFA in the assessment of HR and EE after a 55-minute game session. In general, strong intraclass correlation coefficients were found between HR and EE reported by the RFA, metabolic cart, and Polar FT7. Even though TEM values suggest poor and moderate error in measurement for EE and HR, respectively, LoA, visualized via Bland-Altman plots (Figs. 3 and 4), suggests that the values obtained by the RFA may be a valid measure for HR and EE.
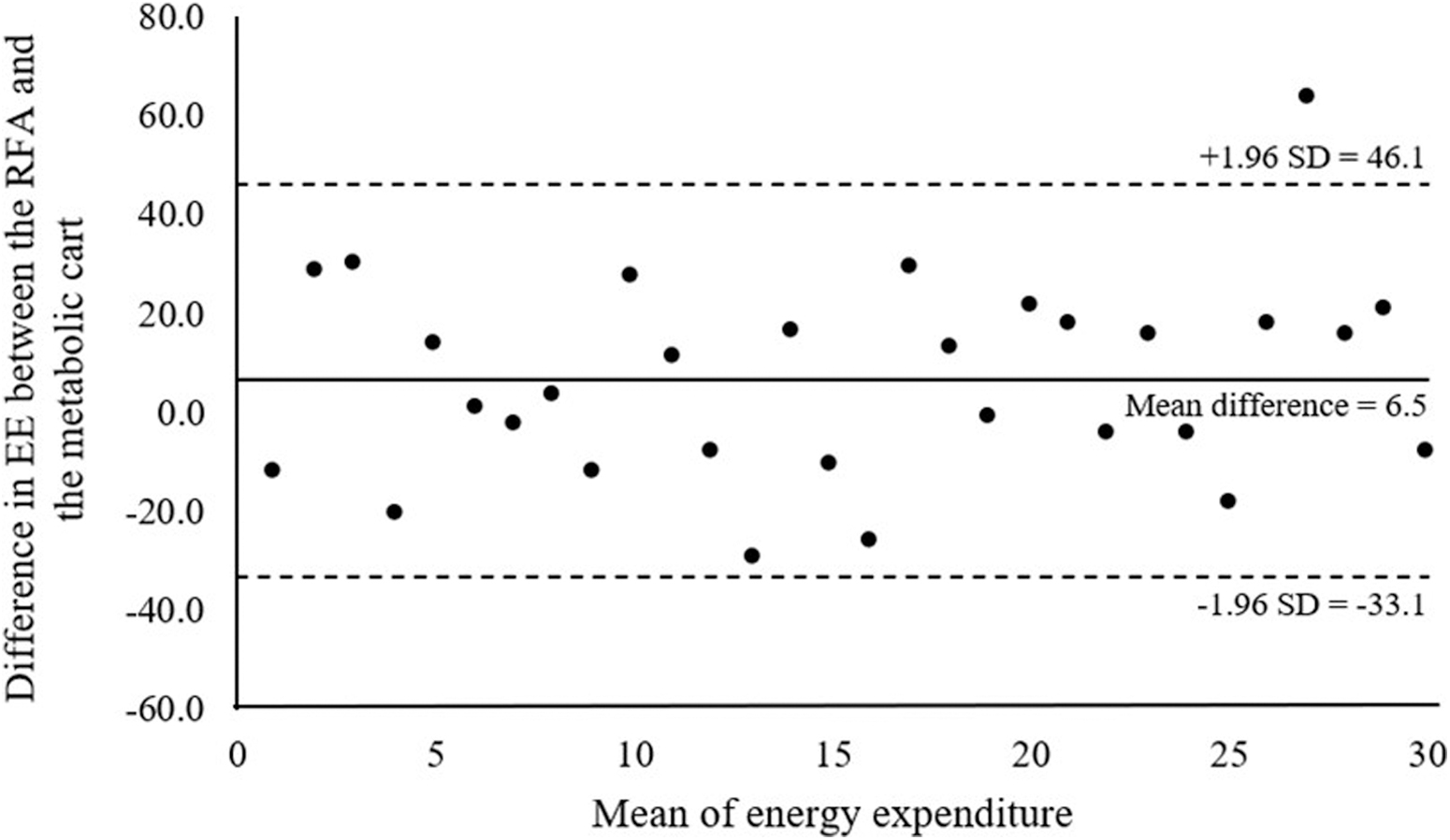
Bland–Altman plots for kcal estimated from The RFA and metabolic cart. EE, energy expenditure; SD, standard deviation.
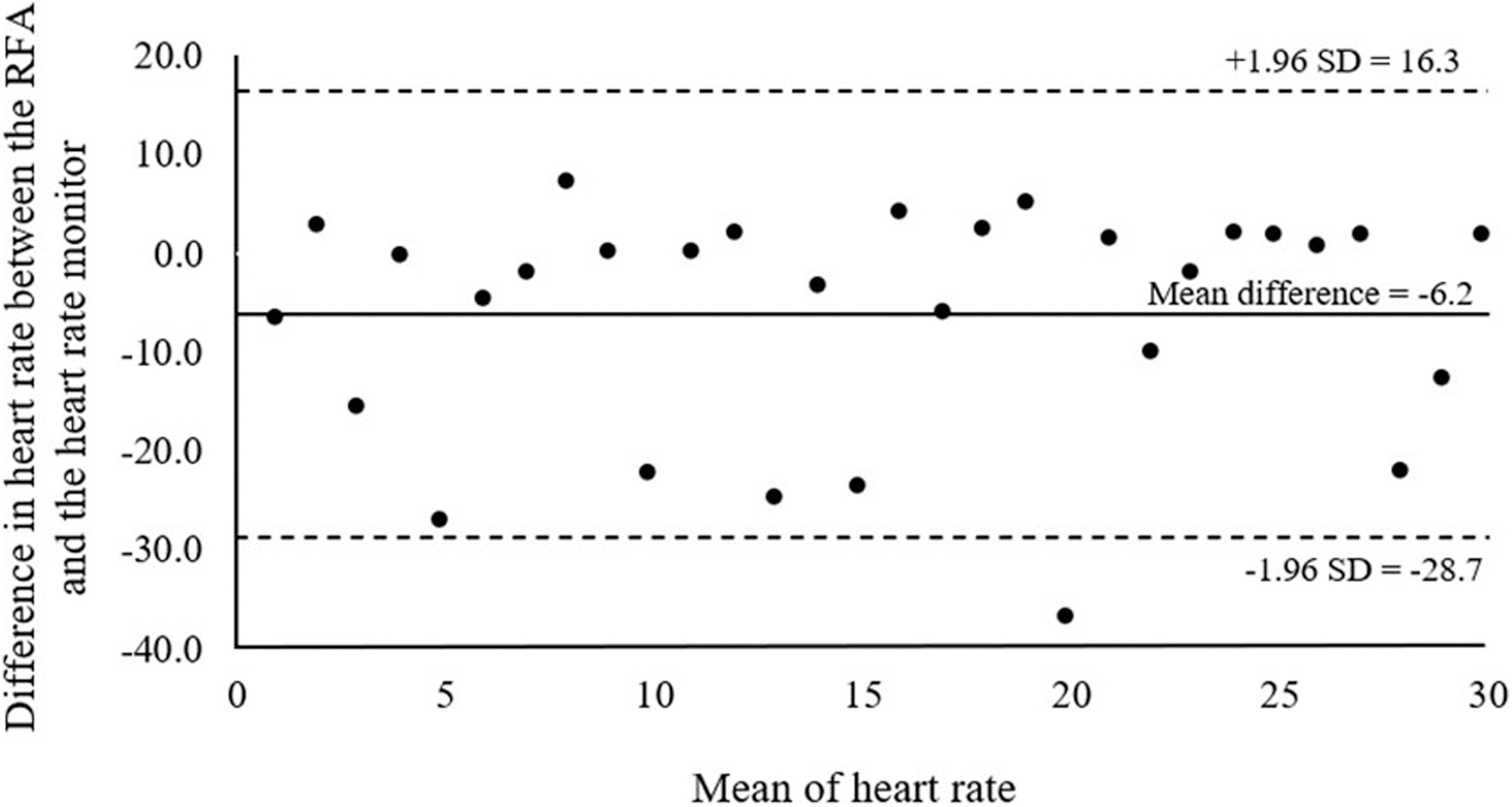
Bland–Altman plots for heart rate estimated from The RFA and heart rate monitor.
For detailed data on the mean values, the MAPE, and the MAPE-adjusted range of these measurements, refer to Table 2. Levels of enjoyment were reported as fairly high whereas the RPEs reported remained low (although, as we hypothesized, progressively increased throughout the session).
Mean Values, Mean Absolute Percentage Error (MAPE), and MAPE-Adjusted Range for Energy Expenditure and Heart Rate as Measured by Ring Fit Adventure
MAPE, Mean Absolute Percentage Error.
One session with the RFA increased the participant's EE by ∼6.9 ± 1.5 kcal/min. This value is higher than the one reported by Comeras-Chueca et al. that reached 4.9 ± 2.0 kcal/min in a sample of 45 children with an age range of 10.1 ± 1.0. 39 It is important to highlight that compared with other exercise modalities, the RFA stayed below the EE mean.
For example, Gerosa-Nieto et al. in a sample of adult men with OB reported that with 20 minutes of high-intensity interval training (HIIT) participants burned 13.9 ± 1.9 kcal/min, whereas in a 40-minute session of moderate intensity continuous training (MICT) a total of 7.5 ± 0.5 kcal/min was achieved. 56
Even though the number of calories is relevant to reduce visceral and subcutaneous fat stores and other comorbidities, 57 fostering exercise adherence is paramount, as it promotes intrinsic motivation and enjoyment, which are key to sustained weight management. Taking this into consideration, our protocol with exergames demonstrated that exercise engagement was higher (89.1%) than the scores from HIIT (62.9%) and MICT (61.4%) in Ram et al. 58
Therefore, a better perception of exercise enjoyment through the exergames may be associated with greater future engagement, and thus, a greater likelihood of becoming habitual, as previously proposed by several authors.40,59,60
Given the previously mentioned time and intensity guidelines stated in the Physical Activity Guidelines for Americans, it is worth noting that several studies have noticed that playing exergames can elicit mainly a light-to-moderate intensity activity with some reporting even vigorous intensity.34,61–67
These discrepancies in intensity may be explained based on the type of game (e.g., golf, boxing) and the console (e.g., Xbox, Nintendo Wii). In the present study, the exercise intensity during RFA was mostly moderate intensity during 70% of the intervention. Continued engagement, however, is likely to result in greater engagement with exergames, ultimately resulting in more time spent exercising. Hence, they will likely allow people to comply with the Physical Activity Guidelines with greater ease, leading to an improvement over time in their cardiorespiratory fitness and overall health.68,69
It is important to highlight that RPE using Borg's scale varied from very light (value of 6) to somewhat hard (value of 14) along with a high enjoyment perception (71.3 ± 5.9 Arbitrary units) during the 55-minute session. It is important to highlight that on average, higher RPEs were reported as the game progressed, which matched the increase in HR. Nevertheless, high enjoyment perception persisted during the 55-minute session. Even though no comparison was conducted between a traditional exercise and the RFA, previous literature demonstrates that exergames elicit a lower RPE as compared with traditional stationary cycling,36,70 dancing, 71 and treadmill walking. 63
We propose that the high levels of immersion in the RFA, as well as the autoregulation that the game allows for result in high levels of enjoyment despite concomitantly increasing RPEs and HR. These results are supported by the Dual-Mode Theory of affective responses to exercise posing that exercise intensities below the individual's sub-ventilatory/lactate threshold tend to be uniformly perceived as pleasant, whereas exercise intensities approaching their threshold tend to be more variable, and those exceeding it are uniformly perceived as unpleasant. 72
Unsurprisingly, sub-ventilatory/lactate responses tend to correspond to light-to-moderate exercise intensity, which was precisely the exercise intensity that participants in this study self-selected. All these findings have important implications in OW and OB populations since they might be more likely to engage in session with exergames and, consequently, improve PA level.
One of the most relevant contributions of the present study is the very strong ICC between EE reported in the RFA (180.7 ± 44.1 kcal) and the metabolic cart (171.8 ± 39.7 kcal) during the exergame session. In short, it would be valid and reliable to use either of the two devices to evaluate EE. In the same line, HR between the RFA (122.8 ± 20.1 bpm) and the Polar FT7 (129.0 ± 18.6 bpm) yielded a very strong ICC, but after comparing both methods against each other, a significant difference was found.
This seems to indicate that the videogame underestimated the HR of the participants. However, a low MAPE, moderate TEM, and narrow LoA suggests that the HR reported by the RFA can be considered reliable, although with some consistent deviation between measurements that do not vary widely from the standard reference. Although our findings suggest that the RFA provides reliable EE and HR measurements, it is important to consider methodological limitations from this study that could have influenced results.
Among them, biological sex as a potential moderator/mediator stands out. Previous research indicates that physiological responses can vary across the menstrual cycle, affecting oxygen consumption and EE. 73 Our study, being the first to validate RFA output measures, did not account for these variations, which presents a limitation and points to the need for future research to address our limitations when assessing the validity of exercise-related physiological metrics. To the best of our knowledge, this study is the first to validate the RFA's physiological metrics against established measures. As such, we recommend that subsequent research incorporate these biological considerations. While we proceed cautiously with our conclusions, we encourage further studies to refine and corroborate our findings.
Conclusion
We conclude that EE and HR collected by the RFA are valid measures after comparing them with a gold standard and a validated method (i.e., metabolic cart and HR monitor, respectively). People who use the RFA as a tool to perform PA can rely on the HR and EE values provided by the device. More specifically, people with OW and OB, who usually tend to face more barriers for exercise adherence and enjoyment, 74 can use the RFA (and its corresponding outputs) to engage in regular exercise and thus increase their PA levels while benefiting from its downstream benefits all the while.
Although our findings are encouraging, we suggest further research to be conducted and current limitations to be addressed to corroborate current findings and address existing limitations that prevent generalizing these results.
Footnotes
Authors' Contributions
P.B.M.C. and N.E.C.C.: Conceptualization, investigation (data collection, data extraction), and writing–original draft. R.E.G., J.J.C.N., and B.M.H.: Conceptualization, methodology, writing–original draft, and writing–review and editing. J.C.: Writing–original draft, writing–review and editing. J.A.A.C.: Conceptualization, methodology, formal analysis, writing–original draft, and writing–review and editing.
Data Availability Statement
The datasets generated and analyzed during the current study are not publicly available but will be provided by the corresponding author on reasonable request.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
The author(s) received no financial support for the research, authorship, and/or publication of this article.