
Abstract
Background:
Combined behavioral- and pharmacological-based tobacco cessation interventions are effective for adults with serious mental illness; yet, they continue to smoke at alarming rates.
Materials and Methods:
A pilot two-arm randomized controlled trial of the program consisted of 50 minutes of game-based groups 3×/week, for 12 weeks alongside counseling and pharmacotherapy. The intervention group engaged in game-based group physical activity (PA), while the control group engaged in sedentary games.
Results:
Multilevel regression analyses were used to examine the primary aims. Mean number of cigarettes smoked per week (cig/wk) for the sample (n = 48) at enrollment was 56.3 cigarettes. The linear change was significant at 2.9 fewer cig/wk. The average psychiatric symptom score at enrollment for the PA group was 41.5 points with a significant predicted linear decrease in scores.
Conclusion:
Both study groups showed a significant reduction in cig/wk. The combination of counseling and pharmacotherapy offered in groups may have aided with cessation and cigarette reduction while also providing a benefit to mental health.
Background
Smoking remains disproportionately high among adults with serious mental illness (SMI). Individuals with a SMI may have a diagnosis of schizophrenia, schizoaffective disorder, bipolar disorder, psychotic disorder, post-traumatic stress disorder, or treatment refractory major depression with a negative impact on functioning and well-being. 1 The age-adjusted mortality rates for adults with SMI are two times that of the general population,2–5 despite increasingly improved responses to psychiatric treatment.6,7 Cigarette smoking is the major contributing factor to this disparity and the high prevalence of acute and chronic disease and disability among adults with SMI.3,8 Adults with SMI are more likely to have stressful living conditions, low annual household income, and limited access to health care and help quitting smoking. These factors make it more challenging for adults with SMI to quit smoking.9,10
Evidence indicates that combined behavioral and pharmacological treatment for smoking cessation is effective for adults with and without SMI. 11 Studies in adults without SMI indicate that physical activity (PA) may be a beneficial additional component of a smoking cessation intervention to help people deal with the cravings and symptoms that come with the cessation process. 12
For the general population of adult smokers, PA can be a helpful additional component of smoking cessation programs and may help with psychological withdrawal symptoms and reduces the desire to smoke. 12 From a Cochrane review 12 of randomized controlled trials (RCTs) aimed at increasing PA, either alone or in combination with a smoking cessation intervention, four studies found an effect in favor of the intervention at the end of treatment.13–17 The Cochrane review highlighted that of the studies comparing activity levels for the exercise versus control groups, only 7 out of the 11 reported higher activity levels for exercise versus control participants, and no significant difference was found between groups when PA was objectively assessed. 12 The effects do indicate a positive impact of PA in smoking cessation and reducing symptoms such as anxiety and nicotine withdrawal; yet, it is unclear what level of PA (e.g., moderate, vigorous) is needed to aide with a cessation attempt.
The purpose of this article was to describe the impact of a pilot RCT PARQuit intervention for adults with SMI. The first aim was to examine the efficacy of the intervention group compared with the control group by smoking reduction and abstinence at 6 and 12 weeks. The second aim was to determine whether participants in the intervention group had a greater reduction in the number and severity of psychiatric symptoms compared with control participants.
Methods
The theoretical framework for the study was based on a model originally developed by Dr. Debra Lieberman, Director of the Health Games Research national program, and later refined by an American Heart Association scientific panel and published in a report entitled “The Power of Play: Innovations in Getting Active Summit 2011.” 18 The “Power of Play” theoretical model illustrates ways that active games may improve health behaviors (e.g., smoking cessation) by influencing mediating factors (e.g., PA) that are known to improve health behaviors. The model was used to guide the development and testing of the game-based PA program.
The 12-week PARQuit study was designed as a pilot RCT to inform a larger RCT. Institutional review board (IRB) approval was acquired from the sponsoring university’s human subjects committee. Anonymity and confidentiality were maintained.
Participants were recruited from the community, direct contact of potential subjects, and from outpatient mental health clinics and residential facilities. All potential participants were assessed for eligibility as follows: English speaking, >18 years old, diagnosis of SMI (e.g., schizophrenia), smoking at least five cigarettes a day for the past 6 months, and willingness to set a target quit date (TQD).
Participants were excluded if they had known medical conditions or other physical problems that required special attention to engage in an exercise program (e.g., uncontrolled hypertension, use of nitroglycerin to treat angina).
All participants passed a capacity to consent test based on comprehension of the consent form and gave informed consent.
Randomization
After enrollment and baseline data collection, participants were randomized to the PARQuit PA condition or PARQuit control condition. Assignment cards were generated using a software program written to generate random assignment numbers for two equal groups of 5 in blocks of 10 cards.
Intervention groups
The intervention groups were implemented in five successive 12-week “waves.” One intervention and one control groups ran during each 12-week wave, with five participants in each group. Before the COVID-19 pandemic, the first wave was conducted indoors, within a transitional residential program, using motion-based videogames as the PA intervention and seated games for the control group. The transitional residential program provided mental health care, housing, and opportunities for social connections for adults with a SMI. The average length of stay was 6 months, with clients discharged to a variety of places such as a board and care, independent living in an apartment, another mental health facility, or a temporary shelter. Most patients admitted to the transitional residence were admitted from a mental health care acute care unit.
Following systemic shutdowns in early 2020, study protocols were adapted and approved by the IRB to safely continue research outdoors without changing intervention procedures or data collection methods; these new protocols were used for the last four participant waves. The major differences between the initial cohorts and subsequent groups were indoor versus outdoor location and availability of specific games.
PARQuit PA intervention
Participants in the intervention groups were taught warning signs to be aware of while exercising (e.g., shortness of breath, dizziness). Study staff facilitating the groups completed training in Basic Life Support, including training in CPR. After each game session, participants were instructed to rate their perceived exertion 19 on a scale of 0–10 with 0–2 rest to easy; 3–4 moderate to sort of hard; 5–8 hard to really hard; and 9–10 really, really hard to maximal.
All PARQuit PA participants were introduced to the game-based PA intervention 2 weeks before their TQD. As participants prepared to quit, they were familiarized with the PA program, so that activities were a routine part of their week to help buffer cravings and withdrawal symptoms upon the quit date.
Procedures for PARQuit PA first wave
Participants played an active videogame using the Kinect for Xbox® 360 game system (Microsoft, Redmond, WA) for 50 minutes thrice a week for 12 weeks. Each participant had the appropriate amount of space to have full range of motion. Approximately six feet of free space between the participant and the Xbox Kinect sensor is needed. The games offered a variety of levels, and each group started at the beginner level. Some games, like Yoga, provided participants with feedback about how to correct their body movements to correctly match the coach on the screen.
The 12-week wave started with bowling from the Kinect Sports DVD, and participants had the option of 10 games to try for each additional session. All participants eventually played the same 10 games. These games included the following: Kinect Sports (bowling, baseball, volleyball, and skiing), Kinect Dance Central 2, Kinect Adventures (River Rush and 20,000 Leaks), Twister, and Kinect Your Shape Fitness Evolved (Yoga and Body Focus Workouts). The games provide a variety of upper and lower body activities and promote coordination and balance, aerobic capacity, and strength and flexibility.
Procedures for the PARQuit PA subsequent waves
Participants engaged in an active game in a group outdoors in a San Francisco public park for 50 minutes, thrice a week, for 12 weeks. Groups were led by study staff. The game sessions started with a 10–15-minute warm-up (e.g., walking, stretching) and concluded with a 5-minute cooldown. Participants were given the option of a variety of games to try for each session. All participants eventually played the same games. These games included the following: scavenger hunts, lawn bowling, hopscotch, jump rope competitions, spoon and golf ball races, dance competitions, kick ball, soccer, Simon Says with strengthening and flexibility activities, limbo, and timed strengthening and flexibility circuit activities. All games were chosen based on feedback from previous participants and research staff experiences playing the different games in groups of people with SMI. The games provided a variety of upper and lower body activities and promoted coordination and balance, aerobic capacity, and strength and flexibility. All games allowed for multiple players at one time.
PARQuit control intervention
All control group participants were introduced to the sedentary games 2 weeks before their TQD.
Procedures for the PARQuit control first wave
Participants randomized to the control group played sedentary videogames using the Xbox 360 game system (without the Kinect sensor) for 50 minutes thrice per week for 12 weeks. Participants were given the option of 10 games to try. All participants eventually played the same 10 games. These games included the following: Family Feud, The Price is Right, Cars Race-O-Rama, Family Game Night (Connect 4, Yahtzee, Life, Jenga, Clue), Wheel of Fortune, and Pac-Man. Participants played the games seated with a remote-control wireless device.
Procedures for the PARQuit control subsequent waves
Participants randomized to the control group played sedentary group games outdoors in a public park for 50 minutes, thrice per week, for 12 weeks. The principal investigator (PI) or study staff facilitated the weekly sessions. Participants were given options for a variety of games to try. All participants eventually played the same games. Games included the following: Bingo, Guess the Song, Tic Tac Toe, Pictionary, trivia, charades, paper airplane building and racing, clay building competition, and art-based games. The control groups were held at a different time of day than the intervention groups to avoid contamination.
Pharmacotherapy
All study participants were provided with a prescription for nicotine replacement therapy (NRT) (e.g., transdermal patch, gum, and/or lozenges) or bupropion sustained release (SR), detailed information on possible adverse events related to use of NRT and/or bupropion SR, and a schedule for 12 weeks. TQD for all participants was set for 14 days from initiation of the game sessions and counseling.
Participants had a follow-up visit with the PI at 24 and 48 hours after initiation of pharmacotherapy, to monitor for adverse effects (e.g., headache, nausea), and also 1 and 2 weeks after initiation of pharmacotherapy. NRT and bupropion SR are on most prescription drug formularies (including Medicare and Medicaid). Evidence-based tobacco treatments remain underutilized by adults with SMI. Provisions in the Patient Protection and Affordable Care Act have expanded access to Food and Drug Administration-approved cessation medications for Medi-Cal patients, and public/private insurance covers medications at low or no cost. The PI was available to participants throughout the study to consult about any health issues that arose related to the intervention.
Smoking cessation counseling
All study participants were engaged in smoking cessation counseling. We adapted the intervention treatment protocol tested for psychiatric outpatients as described below. 20 The project director facilitated the counseling intervention and has experience delivering counseling for intervention studies. Counseling consisted of eight sessions delivered in-person or by telephone over 12 weeks. In-person sessions lasted 30 minutes each, and follow-up calls were 15–20 minutes. The counseling intervention relied on a cognitive-behavioral framework that focused on enhancing commitment to smoking abstinence, promoting medical adherence, and increasing behavioral skills for achieving and maintaining abstinence. Before the quit dates in sessions 1 and 2, counseling focused on developing an individualized quit plan by engaging each participant to complete a set of brief questionnaires to gain self-understanding of reasons for smoking, concerns and benefits of quitting, and identifying triggers or high-risk smoking situations and corresponding coping strategies. Counseling post-quit date focused on managing withdrawal symptoms, mood management with discussions on increasing pleasant activities, adapting healthy lifestyles, and increasing social support. Throughout the 12-week program, counseling sessions incorporated the use of PA to manage withdrawal symptoms and mood and to increase social support.
Fidelity of the intervention
After field researchers were trained, the PI observed the first two group sessions. The length of the intervention and level of participants’ engagement during the session were recorded by the research team.
Retention protocol
Multiple strategies were used to maximize retention. Study staff made weekly reminder calls to participants for the game sessions and assessment visits. A remuneration plan that increased for each assessment was used. Participants were remunerated with $20 at the first assessment point, $40 at the second assessment (week 6), and $60 upon completion of the intervention or control program (week 12).
Measures
Assessments were completed before starting the program and after 6 and 12 weeks of the program. Participants completed questionnaires and participated in assessments about clinical and sociodemographic information. Study staff measured the outcomes and were not blinded. In this article, we report the smoking cessation and psychiatric symptom assessment findings.
Smoking cessation
Feasibility was measured with a count of sessions attended. Overall retention rates were calculated from the beginning to the end of the intervention.
Tobacco abstinence was assessed at enrollment, 6 weeks, and 12 weeks. Assessment included the number of cigarettes, even a puff, smoked in the past week (7-day abstinence) or use of any form of tobacco or alternative tobacco product (e.g., smokeless tobacco or heat not burn).
The number and severity of psychiatric symptoms were assessed with the Brief Psychiatric Rating Scale (BPRS). 21 The BPRS consists of 16 items rated from 1 (not present) to 7 (extremely severe), and the items are summed for a total psychopathology score. The BPRS is one of the most widely used scales for assessing psychopathology, and the reliability, sensitivity, and validity have been extensively examined. 22 The BPRS was administered at enrollment, 6 weeks, and 12 weeks.
Additional study measures
Demographic information (including gender, age, years of education) and current/past medical history were obtained.
Analysis
Descriptive statistics (means and standard deviations [SDs], or medians and interquartile ranges, as appropriate depending on distributional symmetry) were calculated for quantitative demographic and assessment variables, and frequencies and percentages were calculated for categorical variables. All hypotheses were tested with alpha = 0.05 (two-sided). The analysis for the first and second aims was carried out with multilevel regression analysis 23 to test the change over three assessments in success in smoking cessation (AIM 1) and number and severity of psychiatric symptoms (AIM 2). Change in these outcomes was examined to test the difference in the linear change trajectories between the two arms of the study over three assessments from baseline to 12 weeks (also called the cross-level interaction between group and time). In addition, a multilevel model for each outcome was used to test the pairwise changes from baseline to 6 weeks, 6 to 12 weeks, and the overall change from baseline to 12 weeks.
The method of estimation depended on the scale of the outcome. 24 Multilevel logistic regression was used for change in binary outcomes. 25 For smoking reduction and number and severity of psychiatric symptoms, multilevel linear regression was used. 23 Multilevel regression models typically require large samples for reliable estimation, being based on maximum likelihood estimation (ML) for continuous outcomes and ML with numerical integration and adaptive Gaussian quadrature for dichotomous outcomes. 26 Given the small sample, these methods were used, but estimates and inferences regarding statistical significance were obtained through the use of the nonparametric bootstrap with bias-corrected (BC) confidence intervals (CIs). 27 For non-normal data (such as we expected for number of nonsmoking days and psychiatric symptom severity), this method also has the advantage of providing unbiased estimates without the required assumption of normality for parametric tests.
In the event that participants missed an assessment or dropped out from the study, with multilevel regression, cases with missing data are not lost to the analysis. Multilevel regression estimates are unbiased even with missing data through the use of full information maximum likelihood (FIML) 28 with the expectation–maximization algorithm,28,29 assuming that the missing data mechanism is ignorable, a reasonable assumption for most outcomes in this study.30–32 However, even in dealing with possible nonignorable missingness, it has been shown that missing data methods such as FIML result in less bias in the estimates than estimates using singly imputed values or listwise deletion (complete case analysis).28,33–36
Results
Recruitment and retention
Study recruitment began in August 2019 and continued through March 2022. Sixty-three people consented to participate. Of those 63 participants, 48 were randomized to the PARQuit PA condition 24 or PARQuit control condition. 24 The CONSORT flow diagram in Figure 1 provides more details about recruitment, enrollment, and allocation to the study arms. Seventy percent were male and 30% female. As shown in Table 1, the mean age that participants started smoking was 19.9 (SD = 11.3), and average years of smoking was 23.8 (SD = 15.6). The mean age was 45.4 years (SD = 12.7) and 50% identified as White. More than half the sample had a diagnosis of schizophrenia or schizoaffective disorder (58.4%). The majority (64.4%) lived in a transitional residence.

CONSORT flow diagram.
Characteristics of Participants, n = 48
SD, standard deviation
Feasibility
For the entire sample, the mean number of game sessions attended was 13.4 (SD = 11.1). Twenty-one participants (44%) attended at least half of the sessions. For the PARQuit PA condition, the mean number of active sessions attended was 11.8 (SD = 12). Ten active participants attended at least half of the active sessions. For the PARQuit control condition, the mean number of seated groups attended was 14.9 (SD = 10.2). Thirteen seated/control group participants attended at least half of the sessions.
The average perceived exertion score after completing the PA groups was 4.1 (SD = 2.1) indicating moderate exertion.
Smoking cessation and reduction
Upon enrollment in the study, 69% of the sample opted to use NRT as a cessation aid, 23% opted for bupropion SR, and 8% opted not to use any pharmacotherapy. The mean number of cigarettes smoked per week (cig/wk) for the entire sample (n = 48) at enrollment was 56.3 cigarettes. The linear change was 2.9 fewer cigarettes for each week. This finding for the rate of change was significant (95% BC bootstrap CI = −4.3 to −1.6). The rate of change differed for the two groups (simple slopes), but the difference was not significant. Both groups showed a significant linear decline in cig/wk. The average smoked per week at enrollment for the PA group was 46.8, and the predicted decrease for each week was 2.8 (95% BC CI = −4.8 to −0.9). For the PA group, the mean number of cig/wk at 6 weeks was 23.4, and at 12 weeks, it was 22.2. The mean number of cig/wk at enrollment for the sedentary controls was 65.4, and the decrease for each week was 3.06 (95% BC CI = −5.0 to −1.2). For the sedentary control group, the mean number of cig/wk at 6 weeks was 30.8, and at 12 weeks, it was 37.8.
These differences in the rate of change were very similar, and the sedentary group showed slightly greater absolute change compared with the PA group. Examining the change only as the linear change from enrollment to 12 weeks might obscure important differences in the way the two groups changed. Therefore, given the small sample for this preliminary study, the differences in means at each assessment were evaluated to determine the effect size for the differences between the two groups (using Cohen’s standardized effect size d). 37 This estimate of the effect of the intervention is not influenced by sample size nor on variation in the rates of change (slopes), whereas significance tests are strongly dependent on sample size to provide adequate power to detect even medium effects. This analysis does not test differences between the groups across assessments. The groups did not differ in their rate of change, as described above. This analysis only examines differences between the two groups at each assessment as a simple estimate of how many cigarettes each group smoked at that assessment, and how large the difference was in mean number of cigarettes smoked that week.
As can be seen in Figure 2 (a plot of bootstrapped predicted means from a right-skewed distribution), the mean number of cigarettes smoked declined for both groups from enrollment to 6 weeks, with the difference between them being a medium effect (raw difference = 23.3, d = 0.49) at enrollment and a Cohen’s d weak effect (raw difference = 5.7, d = 0.15) at 6 weeks. However, the difference again increased for the PA group compared with the sedentary group by 12 weeks (raw difference = 24.2, d = 0.54, also a medium effect size). In Figure 2, the mean estimates plotted at each assessment were obtained using a nonparametric, BC bootstrap with 5000 draws and do not imply within-subject change from one assessment to the next. This method provides unbiased estimates of the means without regard for normality in the distribution.

Cigarettes smoked over weeks by group.
At the midpoint assessment, three PA group participants had quit, and two control group participants had quit. At the final assessment, two PA group participants had quit, and four control group participants had quit. However, the differences between the two groups are not significant at either time nor is there a significant change from midpoint to final assessment.
Psychiatric symptoms
Participants’ psychiatric symptoms were examined using the BPRS (Fig. 3). A significant linear decline in BPRS scores for the PA group was found, whereas the control group did not show a significant change. The mean score at enrollment for the total group was 41.6 with a predicted decrease of −0.28 units for each week. However, the average BPRS score at enrollment for the PA group was 41.5 points with a significant predicted linear decrease in scores of −0.37 units per week (simple slope, 95% BC CI = −0.66 to −0.02). The sedentary group reported a mean BPRS score of 41.8 at enrollment and a nonsignificant linear decrease in scores of −0.21 units for each week (simple slope, 95% BC CI = −0.56 to 0.09).
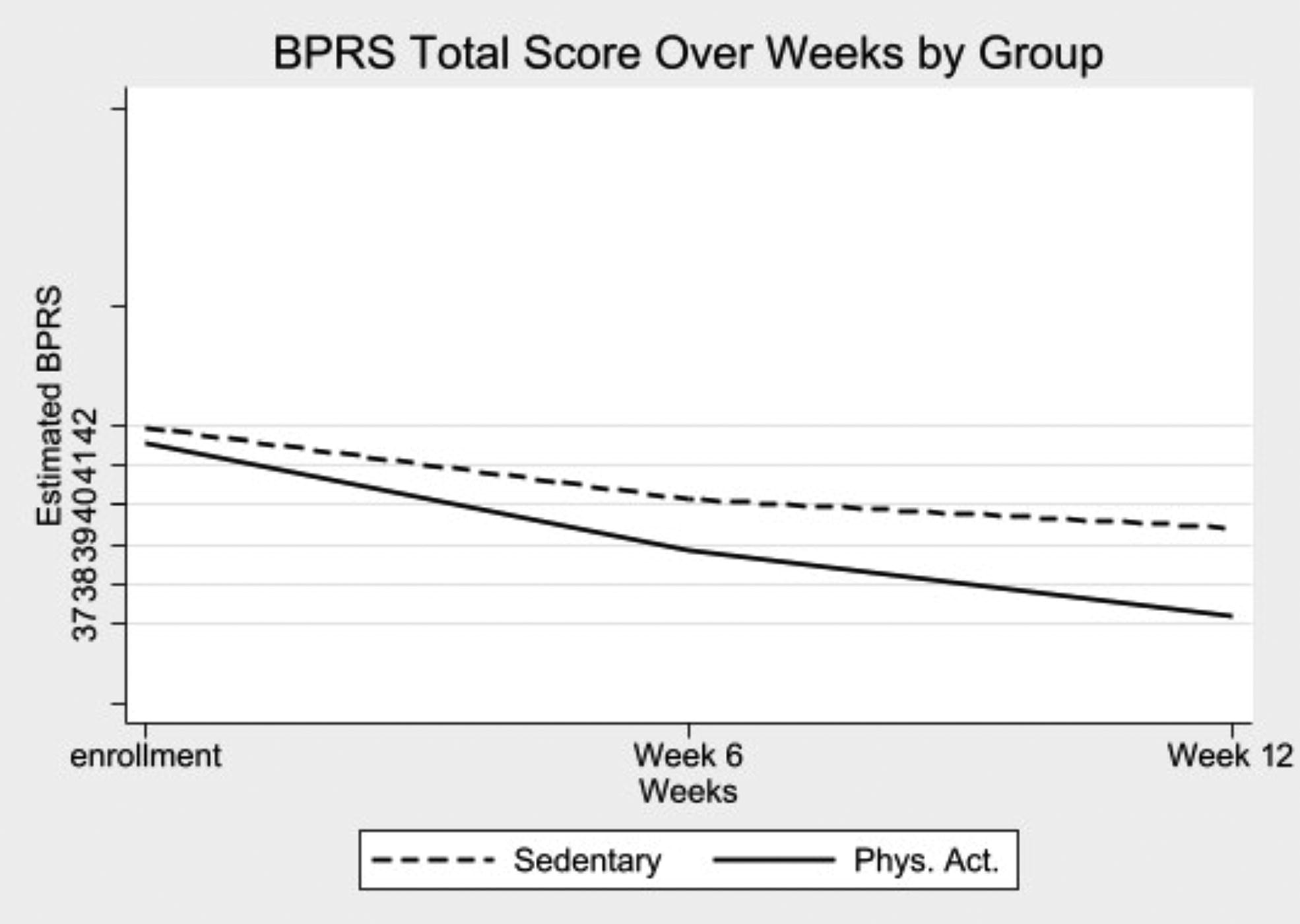
BPRS total score over weeks by group. BPRS, Brief Psychiatric Rating Scale.
Just as for the number of cigarettes smoked, the difference between the two groups on their linear change in BPRS scores was not statistically significant with the small pilot data sample. In examining the differences at each assessment, the initial 0.44-unit difference between the two groups at enrollment (Cohen’s d = 0.04, a weak effect), increased at 6 weeks (difference = 1.4 units, d = 0.13, a weak effect), and increased further at 12 weeks to a difference of 2.7 (Cohen’s d = 0.30, between a weak and medium effect) at the final assessment.
Discussion
This study is the first to show the synergistic effect of a group-based smoking cessation program and game-based PA in an outdoor park setting. Both control and exercise group participants showed significant reductions in cig/wk. Neither group showed an increase in psychiatric symptoms. The findings suggest that this intervention may be a feasible and effective way to help individuals with SMI to begin their smoking cessation journey.
This work complements previous work in this area that shows the mental health benefits of quitting smoking. 38 Two prior studies12,13 documented that adding PA to smoking cessation strategies may benefit people experiencing depression and anxiety. The results presented in this article provide preliminary support for the added benefit of PA for the cessation process and mental health in a sample of adults with SMI.
The PA program was designed not only to meet frequently (thrice a week) over a 12-week period to maintain close contact with participants during their cessation process but also to offer the PA program consistently to help people build PA into their lifestyles. This dose of PA may not have been sufficient to assist with abstinence, but the findings indicate that PA may have played a role in cigarette reduction. In the Cochrane review 12 of RCTs aimed at increasing PA in smoking cessation, the authors theorized that the mechanisms through which PA helps with cessation are multifold and yet to be truly understood but include: (1) developing a physically active identity; (2) brief bouts of PA may curb cravings; and (3) PA may stimulate the central nervous system thus creating an alternative reinforcer to smoking. The average perceived exertion rating after PA in the groups was moderate. More work needs to be done to fully understand the role PA plays in treating tobacco use disorders through a more thorough evaluation of PA levels with both self-report and objective assessments (e.g., PA monitors). The findings show success with cigarette reduction, but there was less success with cessation, consistent with other work on cessation among people with SMI. 39 It is possible that participants need a longer treatment period and more follow-up for the intervention to have an impact on abstinence.
The PARQuit study used a similar combined counseling and pharmacotherapy approach as the Smoking Cessation Intervention for Severe Mental Illness trial (SCIMITAR+). 39 In the SCIMITAR+ trial, intervention group participants were offered a smoking cessation intervention that was adapted for people with SMI. The PARQuit study is similar in that NRT was also offered before the quit date, and multiple counseling sessions were offered before the quit date. PARQuit differs from SCIMITAR+ in that PA was added as an additional cessation support. The SCIMITAR study results showed that maintaining smoking cessation was difficult for program participants. Further testing of the PARQuit program is needed to determine the longer term outcomes for smoking cessation and/or reduction. It is possible that the addition of PA to counseling and pharmacotherapy may help with longer term outcomes. Both the PARQuit and SCIMITAR+ trial demonstrated that engaging in a smoking cessation program was not detrimental to mental health. The reduction in psychiatric symptoms in the PA group in the PARQuit program may have been due, in part, to the benefit of engaging in PA.
In addition, transitioning to the park setting was feasible and accessible for participants who tend to spend hours in indoor programs. These findings complement research on benefits of park-based PA.40–42 In a systematic review of 11 studies evaluating the effects of outdoor PA initiatives versus those conducted indoors, the vast majority of studies (n = 9) showed that mental well-being improved in outdoor PA. 41 Urban parks have been identified as a key social determinant of health that can provide a platform for active recreation options in a free and accessible location. 43 In this study, participants were introduced to and familiarized with nonsmoking park settings where exercise or relaxation can be continued after program completion.
Important limitations to this study need to be considered. First, the emergence of the COVID-19 pandemic necessitated important protocol changes with the transition from indoor-based games to games offered outside in public parks. In addition, the lack of objective verification of smoking cessation is a limitation. Although the results show success with reduction, to achieve the ideal goal of cessation, modifications that may be needed include a longer intervention, incorporation of peer support, and additional ongoing reminders to take the NRT. It should also be noted that only 50% of the PA participants completed the 12-week assessment. Despite these limitations, the pilot study informed the larger RCT currently underway. Furthermore, this work demonstrates an important step toward improving tobacco treatment in a population that is often not prioritized for these treatments.
Conclusion
Further research is needed to determine efficacy with a larger sample and to evaluate the impact of the program on sustained smoking cessation. Additional work needs to be done to evaluate the cost-effectiveness of incorporating the intervention into clinical practice. Similarly, evaluating the feasibility of adapting this program to other settings, such as rural areas, is needed.
Footnotes
Authors’ Contributions
H.L. conceived of and designed the study, obtained funding, assisted with data collection, analysis, and interpretation, and wrote the first draft of the article. E.H. assisted with data collection, administered the study protocol, assisted with data management, and edited the article. T.B. assisted with data management and edited the article. D.B. assisted with data collection, assisted with administering the study protocol, assisted with data management, and edited the article. B.C. analyzed and interpreted the data. R.B.S. assisted with the design of the study and data interpretation and edited the article. G.H. assisted with the design of the study and data interpretation and edited the article. All authors read and approved the final article.
Ethics Approval and Consent to Participate
Institutional review board approval was acquired from the sponsoring university’s human subjects committee, and informed consent to participate was acquired from all participants.
Consent for Publication
Not applicable.
Availability of Data and Materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Author Disclosure Statement
All the authors have declared that they have no conflicts of interest in relation to the subject of this study.