
Abstract
Upper limb (UL) motor dysfunctions impact residual movement in hands/shoulders and limit participation in play, sports, and leisure activities. Clinical and laboratory assessments of UL movement can be time-intensive, subjective, and/or require specialized equipment and may not optimally capture a child's motor abilities. The restrictions to in-person research experienced during the COVID-19 pandemic have inspired investigators to design inclusive at-home studies with child participants and their families. Relying on the ubiquity of mobile devices, mobile health (mHealth) applications offer solutions for various clinical and research problems. This scoping review article aimed to aggregate and synthesize existing research that used health technology and mHealth approaches to evaluate and assess the hand function and UL movement in children with UL motor impairment. A scoping review based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) model was conducted in March 2023 yielding 25 articles (0.32% of 7891 studies). Assessment characteristics included game or task-based tests (13/25, 52%), primarily for neurological disorders (e.g., autism spectrum disorder [ASD], dystonia, dysgraphia) or children with cerebral palsy (CP). Although several mHealth studies were conducted in the clinical environment (10/25, 40%), studies conducted at home or in nonclinical settings (15/25, 60%) reported acceptable and highly satisfactory to the patients as minimizing the potential risks in participation. Moreover, the remaining barriers to clinical translation included object manipulation on a touch screen, offline data analysis, real-world usability, and age-appropriate application design for the wider population. However, the results emphasize the exploration of mHealth over traditional approaches, enabling user-centered study design, family-oriented methods, and large-scale sampling in future research.
Introduction
Upper limb (UL) impairments affect residual movement required for reaching, grasping, and dexterous movements of the finger and hand necessary to complete activities of daily living. Developmental and neurological disabilities such as cerebral palsy (CP), autism spectrum disorder (ASD) or attention-deficit/hyperactivity disorder (ADHD), dysgraphia, dystonia, and Down syndrome (DS) are common; 17% of children (1 in 6) aged 3–17 were diagnosed with a developmental disability in the United States during 2009–2017. 1 A common attribute among children with these diagnoses is the presence of hand and UL motor dysfunction.2–4 Children with fine motor disorder, especially dysgraphia and dystonia, tend to have more impaired eye–hand coordination, grasping, and gripping to perform an individual finger movement. In contrast, children with hemiparetic cerebral palsy (HCP) have difficulties with both fine and gross motor skills required to perform functional activities. 5
Because increases in newborn care lead to high survival rates, a primary goal of rehabilitation is to provide therapies early and throughout development to support long-term independence and function. To adequately determine the efficacy of novel rehabilitation therapies for these populations, reproducible measures of UL motor performance across development are critical. Furthermore, assessments of motor performance are pivotal for monitoring changes in a child's motor development and play a key role in studying atypical and typical motor development longitudinally throughout childhood.
Traditional motor assessments used in basic and clinical research for children with HCP include standardized clinical tests of gross and fine motor function, three-dimensional (3D) motion capture for kinematic analysis of the UL and gait, and functional tasks in a controlled laboratory setting.6−8 Advancements in technology have expanded the capabilities of researchers studying movement to include methodologies such as augmented/virtual reality (AR/VR), videogames, and wearable or mobile devices. Previously published review articles concluded that most studies of hand function development use clinical or qualitative assessments9,10 and that optoelectrical devices and 3D motion capture systems were the most often used technology for laboratory-based upper limb assessments. 11 Apart from the subjective nature of clinical assessments, a limitation of the laboratory remains the expensive and stationary nature of the equipment and often time-consuming analysis techniques.
Another barrier to laboratory and clinical assessments is the requirement for in-person administration and observation of participants by clinicians or researchers. Altogether, current assessment methodologies need the timeliness, specificity, and objectivity needed to examine motor performance and constrain how, when, and by whom UL motor performance can be assessed.
Researchers have recently focused on designing and developing game-based clinical diagnostics and motor skill assessment methods for long-term rehabilitation to address these barriers. High-resolution, ready-to-use, portable, accessible, flexible, and customizable systems for participants to perform real-world behaviors illustrate the benefits of using games and mobile health (mHealth) platforms for experimental protocol design, leading toward effective data collection outside the laboratory. 12 A purposive sampling model on 305 respondents found a positive impact of mHealth service quality on user satisfaction and continued usage, highlighting the importance of providing high-quality services to maintain user engagement. 13 Another study examined the smartphone accessibility requirements on patients with disabilities (e.g., dexterity impairments), where physical presentation, easy navigation, and reducing the layout complexity were found effective for accessibility. 14
A survey of 30 individuals with stroke and 19 occupational therapists showed that game-based rehabilitation systems effectively deliver rehabilitation exercises at home for long-term recovery. 15 Another investigation on the use of mHealth in musculoskeletal physiotherapy physical therapy showed that mobile devices are most acceptable and cost-effective in rehabilitation, especially regarding pain and self-management. 16
In this scoping review, we describe and evaluate the available scholarly literature on mHealth technology and motor assessment in children with UL motor impairments, primarily developmental disabilities. Since existing systematic reviews (SR) on AR/VR and exergaming in UL dysfunctions have previously been published,17−21 we focused this review on newer and ubiquitous mobile devices and mHealth technology. Furthermore, we were interested in articles whose primary goal was assessing or measuring UL motor function rather than intervention or treatment.
Materials and Methods
A standardized framework 22 was followed to conduct this scoping review, where the methods were structured into five stages. Moreover, this review was guided by the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews) 23 and an SR tool, rayyan.ai. 24
Stage-1: identifying the research question
The primary objective of this review was to identify the scope of the mHealth technology, particularly “gamification” and the impact on motor skill assessment in children with motor disabilities (e.g., monitoring and improvement of fine motor disorders using an iPad game). We developed the following research questions (RQ) to guide the scoping review process:
RQ1: What types of mHealth applications using mobile devices such as an iPad, tablet, or iPhone have been developed for assessment of UL motor skills in children with motor disabilities?
RQ2: What clinical conditions/disorders and/or groups of children might benefit from mHealth applications assessing and evaluating UL motor skills?
RQ3: What analytic approaches are commonly used in mHealth applications to analyze UL movement variables quantitatively or qualitatively in children with motor disabilities?
RQ4: What are the current barriers and limitations of mHealth applications for children with motor disabilities that prevent uptake into regular clinical use?
Eligibility criteria
Studies were assessed against the following criteria: (1) written in the English language, (2) peer-reviewed articles published in journals or conferences where the full-text was available, (3) original quantitative study, (4) use of technology capable of being used outside of a laboratory environment OR mobile devices (iPhone, iPad, other tablet), and (5) includes children or pediatric populations with a clinical diagnosis or potential for UL motor impairment.
Stage-2: identifying relevant studies
Two searches were conducted in the databases PubMed, CINAHL, Web for Science, Cochrane, and IEEE public and private articles and created two distinct workspaces in March 2023. Two search strategies identified 7891 records by initial searching. Search Strategy 1 (SS1) contains 884 and Search Strategy 2 (SS2) contains 5681 articles after removing the duplicate records automatically. The two search strategies encompassed a variety of search terms to identify UL movement, children/pediatrics, and categories of technology, including mobile and computer videogames, AR/VR, and robotics. Once the searches were complete, they were imported to the rayyan.ai platform for review. 24 An example of the electronic search strategy is attached in the Multimedia Supplementary Data. Figure 1 shows the stages of the identification process based on the PRISMA-ScR model. 23
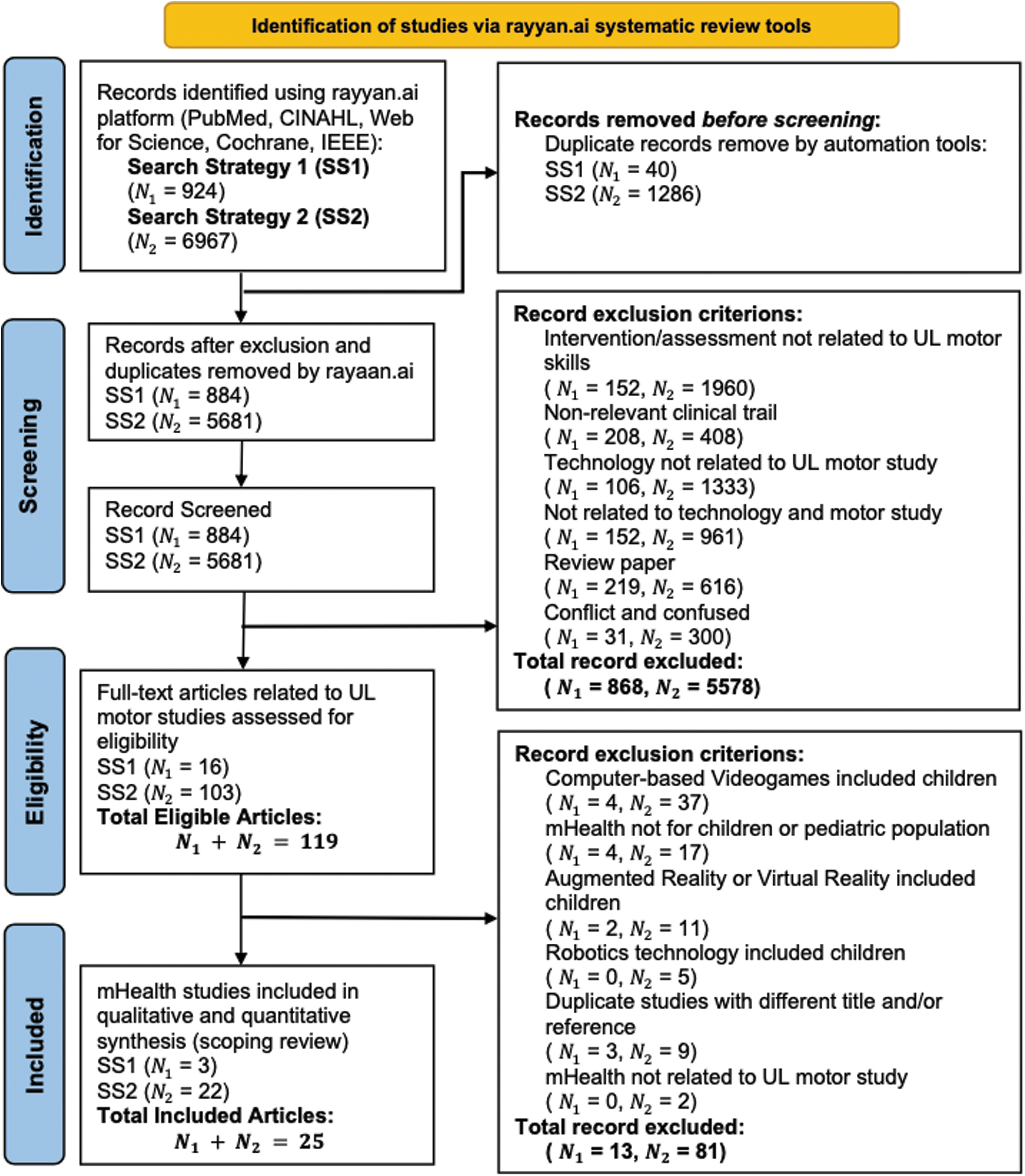
PRISMA-ScR model-based article selection for this scoping review. PRISMA-ScR, Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews. Color images are available online.
In the ‘Screening’ phase, we excluded 98.1% of records from SS1 (868 of 884 articles) and 98.2% from the SS2 (5578 of 5681 articles) workspace after reading the title and abstract. Each article was screened by at least two members of the research team. Any articles with noncongruent ratings (include/exclude) were decided by the Principal Investigator (S.T.N.). Only 119 articles were selected as eligible studies screened by 6 research team members.
Stage-3: study selection
All eligible article references were imported into an MS Excel sheet to create a collaborative workbook. One hundred and nineteen eligible articles were assigned to the group equally for full-text review based on the eligibility criteria. Twelve articles were found to have duplicative content, although their titles and references were different. Eligible articles were grouped into categories and subcategories based on the health technologies, clinical study types, and diagnoses, as shown in Figure 2. Twenty-five articles from SS1 (n = 3) and SS2 (n = 22) that met all the inclusion criteria were included in this scoping review.

A taxonomy tree of all articles after the initial screening of articles. A second round of screening was performed to include articles that only used mHealth technologies for UL motor function assessment and intervention. ASD, autism spectrum disorder; CP, cerebral palsy; mHealth, mobile health; MSDs, musculoskeletal disorders; UL, upper limb. Color images are available online.
Stage-4: charting the data
A data-charting workbook was developed to collect the necessary information from the included studies. This workbook included general data such as author, publication year, and study region, as well as more specific information (e.g., study focus, conditions, methodology, participants, findings, and limitations) relevant to this study. The data-charting was conducted by assigning an equal portion of the articles to the collaborators. Five researchers subsequently charted the data from the included studies, with two additional researchers reviewing information for validity.
Stage-5: collating, summarizing, and reporting the results
Several tables and diagrams were generated to summarize the data for the qualitative and quantitative synthesis of the literature related to using mHealth application (app) in motor skill study. The synthesis included aspects such as the nature of the clinical study, mHealth application types, conditions and target motor skill assessment, experimental design, data analysis methods, and the implication of mHealth applications in children with movement disorders. An iterative process was followed to analyze the data to address the RQ based on specific themes and categories.
Results
This scoping review included 0.32% of studies returned by the search strategies (25/7891). The characteristics of the studies, including publication year, mHealth application types, study focus, region of the study, and participants, are outlined in Table 1. Overall, more studies focused on assessment (14/25, 56%) than interventions (11/25, 44%). Several studies focused on evaluating the effectiveness of the technology (6/25, 24%) and feasibility or reliability (3/25, 12%) of mHealth applications. All studies used quantitative rather than qualitative methods, where randomized controlled trials (11/25, 44%) were prioritized. Table 2 summarizes the outcomes of the studies with potential limitations. The medical conditions and experimental protocols to assess motor skills are also mentioned in Table 2.
Study Characteristics and Participation
app, application; ADHD, attention-deficit/hyperactivity disorder; ASD, autism spectrum disorder; CG, Control Group; CP, cerebral palsy; DMD, Duchenne muscular dystrophy; DS, Down syndrome; GMA, General Movements Assessments; LRJ, left-right judgment; MDD, minimal detectable difference; MT, movement time; OT, occupational therapy; ROCF, Ray-Osterrieth complex figure; TD, typically developing; VM, visual-motor; VMI, visual-motor integration.
Conditions, Methods, and Outcome Measures with Limitations
CI, confidence interval; ID, index of difficulty; mHealth, mobile health; PPVT-R, Peabody picture vocabulary test-revised; SES, socio-demographic status; TGMD-3, test of gross motor development, third edition; TP, throughput.
Types of mHealth applications using mobile devices (RQ1)
Most of the mHealth technology used Apple devices (20/25, 80%), including tablets or iPad (12/20, 60%), and iOS smartphones (8/20, 40%). Other studies used Android (4/25, 16%) or both Android and Apple devices (1/25, 4%). Most of the applications were games or task-based tests (14/25, 56%), and some of the other types were handwriting or drawing (5/25, 20%), video capturing or filming (2/25, 8%), and communication (1/25, 4%) apps. Although all studies stated mHealth was part of the intervention, several experiments included ubiquitous technology (e.g., smartwatch, 30 goniometer 48 ) with mobile devices.
Several studies utilized existing theories and clinical scales to implement motor skill testing with a mobile device. These included the Bruininks–Oseretsky Test of Motor Proficiency for children's fine motor performance, 29 Beery-Buktenica developmental test of visual-motor integration,34,39,40 the Miller function and participation scales for developmental delay, 39 The Hawaii Early Learning Profile for mastery of a skill, 40 Grapho-Motor and Postural Difficulties in Writing using Difficoltà Grafo-Motorie e Posturali (DGM-P), 34 and motor coordination and cognitive abilities test using Movement Assessment Battery for Children 2nd edition (MABC-2).34,38 Fitts law related to human interaction with computer interfaces was also used as a theoretical model to study UL performance within mobile devices.27,31,32
Gamification attributes (e.g., scoring, animations, advancing skill/difficulty) were used in many of the included studies (13/25, 52%). The Marble Maze Classic game, where a ball needs to move toward a destination through a maze path and records movement time, was used to evaluate visual motor skills,39,44 upper limb motor performance, 45 and motor skill learning in CP. 47 Dragging, dropping, and tracking objects on the touch screen were found effective in fine motor skills, 38 arm movements, 28 oral motor skills, 42 grapho-motor skill 34 assessment, and eye–hand coordination. 49 These object-tracking studies analyzed kinematic parameters such as movement path (x and y coordinate in two-dimensional [2D] space), trajectory, time, velocity, error count and score, and difficulty level. Drawing objects (e.g., square, circle, shape) and handwriting tasks in tablet/iPad game were used for evaluating manual dexterity and handwriting skills in children with dysgraphia.26,43,46
Moreover, tablet-based complex figure drawing (e.g., Rey–Osterrieth complex figure) was explored to analyze performance between autistic and attention-deficit/hyperactivity disorder (ADHD) cohorts. 36 The smart-tablet serious game was materialized in an upper extremity and finger movement study design. 35 The iterative cycle was considered a suitable game design based on user-centric feedback and input, such as OutWords 42 and HanDex. 46
Clinical conditions or diagnoses where mHealth has been used (RQ2)
Developmental and/or intellectual disorders were the most common conditions (12/25, 48%), which included ASD and/or ADHD (4/12, 33.3%), dysgraphia or handwriting difficulties (3/12, 25%), CP (2/12, 16.67%), DS (1/12, 8.3%), dystonia (1/12, 8.3%), and other developmental disabilities (1/12, 8.3%). Other motor disorders where mHealth was used also included musculoskeletal disorders (1/25, 4%) and Duchenne muscular dystrophy (DMD; 1/25, 4%). Several articles explored specific motor skill disabilities, such as visual motor perception and integration skills (2/25, 8%), fine motor disorders (2/25, 8%), and grapho-motor impairments (1/25, 4%), rather than investigating motor difficulties among groups with specific diagnosis. In total, 2653 participants were represented in the included studies (1960/2653, 73.9% children), with sample sizes ranging from 7 to 780 participants (median sample size = 54).
Analytic approaches to quantify movement variables (RQ3)
Among studies in which the aims were related to movement assessment, most used spatiotemporal variables to quantify movement speed and accuracy.25–27,29,32,34–36,38,42,43,45,46,49 Others used the sensors (accelerometers, cameras) existing within the device to measure whole-limb kinematics and/or whole-limb movement.28,30,33,41,48 Questionnaires or surveys collecting data directly from participants or parents were used in the pre- and post assessment of conditions and motor skills.28,33,36,42 Two studies proposed mobile apps as clinical diagnostic or monitoring tools, which can calculate clinical parameters (e.g., Index of Performance, Throughput, Movement Time vs. Index of Difficulty) from movement.26,27 Common statistical analysis methods (analysis of variance,34,48 regression analysis, 44 chi-square [χ 2 ],33,35 and Tukey's honest significance 45 ) were used to test differences among groups and experimental conditions (8/25, 32%). Data analyses were conducted using MATLAB, Python, IBM SPSS Statistics, or other programming languages/tools, where data were stored, processed, and retrieved from a comma-separated value (CSV) or other machine-readable formats .26,34,35,38–40,46
Barriers and limitations of mHealth applications (RQ4)
Studies whose goal was feasibility and usability testing involved relatively small samples with a lack of power analysis. Some studies relied upon existing apps and games in their work,25,28,39,44,45,47 while others used custom-built and adaptable software motor skill testing and intervention. Specialized equipment 25 or wearable devices (e.g., smartwatch, 30 goniometer 48 ) integrated with smartphones/tablets were required to collect data for some studies. A few studies provided comparisons between movement assessment parameters and gold standard tests/scales for testing validity.33,34,44,45,48
Discussion
Potential of mHealth applications for studying UL movement (RQ1)
This scoping review revealed a small body of relevant research on mHealth and other mobile technologies for motor intervention and assessment in pediatric populations. Ubiquitous technologies such as the Apple iPad were the most common investigation platforms. There were two main strategies for collecting movement data. The first involved implementing games and tasks into the touch screen for direct user interaction. Not surprisingly, a common focus of many studies surrounded specific visuomotor skills, such as handwriting, which are easily captured using a 2D touch screen. The second strategy utilized the inertial sensors (accelerometer and gyroscope) or video recording features of the device for 3D movement analysis during functional tasks.
These two strategies produced primarily spatiotemporal (2D visuomotor tasks) or kinematic (3D) outcome variables, respectively. Using a user-centered design allowed for flexibility to modify and adapt mobile applications for children with physical or developmental disabilities, many of which were the focus of the studies within this review. Still, studies using other technologies (computers, VR, commercial videogame systems—not included in this review) appeared to outnumber those using mHealth and mobile device technologies. The lack of studies is likely due to the relative recency and ubiquity of mobile devices and the expansion of broadband wireless internet communication. While broadband internet access is still growing, the ubiquity of mobile devices outpaces other forms of technology 50 that are used daily, regardless of racial or socioeconomic standing.
Target population of gamification approaches (RQ2)
Various conditions and diagnoses were found across the studies, highlighting the broad scope of upper limb motor dysfunction in childhood. Some research groups tested their mHealth game in multiple populations (e.g., ASD, hypotonia, and DS).25,30 However, it remains to be determined if available technologies apply to more than one clinical population. Furthermore, there are often wide age ranges in pediatric studies, likely to represent a wider population of children with certain diagnoses or to study the impact of neurodevelopment on motor functions. However, large age differences pose challenges for designing age-appropriate games and applications that will motivate and engage all users. For instance, a teenager may require fewer instructions and more significant skill challenges for completing tablet-based tasks than a young child. Future work investigating usability should consider how design features such as animations, graphics, and degree of difficulty are matched with a potential user's age or neurodevelopmental status.
mHealth technologies facilitate quantitative movement analysis (RQ3)
Movement data were primarily analyzed quantitatively, capitalizing on the sensor technology within the mobile devices. Spatiotemporal, kinematic, and performance-based measures were the most used analytic methods, altogether reducing subjectivity and observer-rated bias. Combined with analytical approaches, studies using multivisit observational study designs were effective in tracking the gradual progress of motor skill performance or determining motor skill acquisition and/or retention. Collectively, these results emphasize the advantages of mHealth and mobile applications over traditional clinical or laboratory approaches and could facilitate population-based studies through large-scale and repeated sampling. More sophisticated analytic techniques, such as automated analysis output, machine learning, and artificial intelligence, could also be incorporated to future solutions. Studies that focused on mHealth technology as an intervention tended not to include formal analysis of movement data and relied on traditional in-person assessments as outcomes.29,37,39,40,42,43
Thus, expanding how mobile technologies might be used as clinical outcome measures needs to be tested in future research. In addition, although quantitative measures provide precise quantification of movement parameters, it is still being determined whether or how these metrics relate to real-world upper limb motor studies and participation in everyday activities.
Remaining barriers to clinical translation (RQ4)
The ubiquitous nature of the mHealth application has the potential to conduct large-scale studies outside the laboratory. Despite the feasibility of mHealth approaches, as evidenced in the studies reported herein, there are several limitations and remaining barriers to clinical implantation. General methodological limitations were common across the articles reviewed: comparison of outcomes with gold standard laboratory methods, lack of control/comparison groups, and small sample sizes.30–32,36,38,40–43,46 One main barrier to further clinical translation is how data are processed and analyzed once collected by the mHealth application. The summarized studies mostly used offline data analysis approaches, which require more time and effort from the research team. If the primary outcomes are identified a priori, one other upside of application development is the ability to program automated analysis scripts for instant data analysis and presentation. Access to real-time data would be advantageous for the clinician for efficient decision-making and planning.
A second barrier is designing usable applications without the aid of research or clinical staff. For many mHealth technologies summarized, the real-world usability of these applications still needs to be determined as only 12% of studies (3/25) were designed to take place in the home environment. mHealth interventions and assessment tools promise that they will facilitate real-world research in various settings. However, the validity of these applications requires further testing to ensure acceptability and to minimize nonuse from technical and user errors. Furthermore, touch screen interfaces limit object manipulation assessment, critical for real-world functional activities. Thus, mHealth assessments may only evaluate parts of tasks (reaching, individual finger movements) rather than whole tasks. The connection between 2D movement analysis and the performance of functional tasks remains to be elucidated.
Furthermore, there appeared to be fewer studies focusing on mHealth applications in children, which may reflect the imbalance of funded research dedicated to pediatrics compared with adults in the United States. 51 Given their ongoing neurological, social, and emotional development, children may be less motivated or cooperative in performing traditional motor assessments, making them an ideal population for game-based approaches that are engaging and intrinsically motivating.
Limitations
The limitations identified in this review include the articles selected from the last 10 years' publication range, as well as we excluded non-English articles (e.g., Russian, Japanese, Chinese). Moreover, consulting with authors in the review process may have revealed additional insightful information. Despite this, the presented scoping review sufficiently meets the study's aims.
Conclusion
Mobile devices integrated into mHealth solutions can assess movement remotely and provide objective and quantifiable measurements. This scoping review highlights the advantages of mHealth for evaluating upper limb motor dysfunctions. Recently, mobile applications have been the most accepted media among patients for communication and as diagnostic, monitoring, and treatment tools. This review has identified the remaining barriers to clinical translation, primarily the lack of real-time mobile data processing, clinical aid for research participation at home, and age-appropriate games or applications designed for large-scale study. In addition to extensive user-centered design and development, further validation and reliability research should be pursued based on current solutions to facilitate future translation into clinical and community settings.
Footnotes
Acknowledgments
The authors thank the occupational therapy graduate research assistants who completed article screening and data extraction.
Disclaimer
The content is solely the authors' responsibility and does not necessarily represent the official views of the National Institutes of Health.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Research reported in this publication was supported by the Eunice Kennedy Shriver National Institute of Child Health & Human Development of the National Institutes of Health under Award Number P2CHD101899.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.