
Abstract
Background:
Hospitalized pediatric patients and their caregivers often experience anxiety and fear, resulting in withdrawal and aggression. Despite virtual reality (VR) being a safe and effective anxiolytic, it is unknown what software design aspects contribute to its effectiveness. This prospective observational study evaluated which VR application elements increased awe, which is correlated with improved behavior and satisfaction.
Methods:
Patients aged 6 to 25 years and their caregivers at an academic pediatric hospital interacted with a custom VR application that compared design aspects, including environment, graphics fidelity, and presence of a motivational character. Outcomes investigated self-reported awe, vastness, accommodation, and engagement. Data were analyzed using repeated measure ANOVA tests and correlation analyses.
Results:
A total of 202 participants were enrolled, and 179 (88 pediatric patients, 91 adult caregivers) were included in the final analysis. A fictional environment was more effective at increasing awe in pediatric patients (P = 0.030) compared with a realistic environment. However, increased graphics fidelity was more effective at increasing awe in caregiver adults (P = 0.023) compared with low resolution graphics. Presence of a motivational character did not influence awe in either patients or caregivers (P = 0.432, P = 0.904, respectively). All measures of awe were positively correlated with application engagement (P < 0.005).
Conclusion:
In conclusion, when software developers design VR software for pediatric patients and their caregivers, fictional settings and increased graphic fidelity should be considered for pediatric patients and adults, respectively. Future studies will explore other VR elements in gameplay settings.
Introduction
Hospitalized pediatric patients often experience anxiety and fear, resulting in lack of cooperation, withdrawal, and aggression.1,2 These reactions delay medical care and negatively impact patient experiences. 3 Similarly, the majority of caregivers also experience anxiety while caring for their children in the hospital. 4 Traditional strategies to manage health care-related anxiety include education about the hospital experience, child-centered play therapy by certified child life specialists (CCLSs), and anxiolytic medications such as benzodiazepines.5–10
Virtual reality (VR) is a safe and effective adjunct that reduces anxiety and pain perception without the side effects of pharmacological agents or need for the individualized attention of a CCLS.11–15 In addition to pediatric patients, VR also mitigates caregiver apprehension. 16 Anxiety-relieving VR applications can be experienced by patients and caregivers at low cost and low risk, providing family-centered care that increases patients’ sense of agency.11,16 VR supports efforts to engage patients and their families in their treatment plans, which improves rehabilitation and compliance. 17 Given the potential drawbacks of benzodiazepines and limited availability of CCLS, VR is an effective anxiolytic poised for widespread utilization.9,11,18 However, development of VR health care applications has progressed faster than research related to what aspects of VR applications are actually most effective at relieving stress.
The definition of awe integrates insights from religion texts, humanities, and social science research. 19 Awe is a powerful emotion with two primary components, perceived vastness and need for accommodation from Piaget’s theory of cognitive development. 20 The former involves the perception of something large or all-encompassing, such as El Capitan in Yosemite National Park, CA, or the Golden Gate Bridge in San Francisco, CA.19–21 The latter refers to the cognitive process whereby individuals are compelled to restructure their mental frameworks of the world to accommodate the perceived vastness, such as spiritual or epiphanic experiences that can change the course of one’s life.19–21 Moreover, the construct of awe encompasses five features as follows: the supernatural, exceptional ability, virtue, threat, and beauty, which converge to evoke a complex and positively valenced emotion with promising applications in promoting human flourishing. 19 Awe predicts decreased levels of anxiety and depression, coupled with augmentation of feelings of well-being.22–24 Awe also decreases daily stress and fosters curiosity, a holistic measure of engagement that contributes to cognitive and emotional involvement.25–27 Finally, awe has high application potential in VR technology; visual immersion with VR elevates self-reported feelings of awe and induces the autonomic nervous system.21,28
In the hospital, most anxiety-relieving VR applications are commercially developed. 11 However, data regarding design elements that differentially contribute to application effectiveness are limited. The primary aim investigated software design elements of VR applications that improved self-reported awe of hospitalized pediatric patients and adult caregivers. The secondary aims evaluated how VR software design elements modulated vastness, accommodation, and engagement of pediatric patients and their caregivers.
Methods
Study design
This was a prospective, observational registered clinical trial (NCT05743062) approved by Stanford University Internal Review Board (IRB-69170) that adhered to STrengthening the Reporting of OBservational studies in Epidemiology cohort study guidelines. 29
Setting
This study was conducted at Lucile Packard Children’s Hospital Stanford (LPCHS), an academic, quaternary care children’s hospital in Northern California containing 365 beds. Patients have access to CCLS, anxiolytic medications, and technology-based adjuncts such as tablets and VR. Participant recruitment and data collection were conducted from June 29, 2023, to August 3, 2023.
Participants
Patients 6 to 25 years in preoperative and inpatient acute care areas of LPCHS were eligible. Adult caregivers greater than 18 years accompanying these patients were also eligible. Participants were excluded if they had nausea at time of recruitment, a history of severe motion sickness, a history of seizures, vision impairment, hearing impairment, or significant developmental delay. Patients and caregivers with facial abnormalities or injuries prohibiting comfortable use of the headsets were also excluded.
Trained research assistants (RAs) recruited participants through in-person solicitation. Eligible patients and their caregivers were sequentially approached for participation as they were admitted to the hospital or preoperatively. There were no financial payments for participation.
Intervention
Design and software development
The research team developed the game, Wonder Reef, using Unity (Unity, San Francisco, CA) through an iterative process utilizing nonlinear, user-centric design thinking strategies.30,31 The team first informally engaged patients, providers, and caregivers to hear their experiences and motivations about using VR in the hospital setting. After this human-centered approach to understand and define user needs, the team challenged assumptions, ideated, prototyped, and tested according to the Design Thinking process to develop a fully immersive engaging experience. 31 The genre of Wonder Reef was a casual simulation game with active, first-person gameplay to increase user engagement and accessibility, adapt to the dynamic timing of health care, and improve feelings of escape from the hospital setting. 32 Given a health care environment where patients undergo dynamic positioning (e.g., patients are often moved from supine to upright), not having a horizon line was important for decreased shifting orientations, reduced nausea, and improved patient experience. 33 Thus, an underwater setting was chosen. In addition, users were stationary within the VR environment so users with limited physical mobility could participate.
The end product VR program displayed an underwater world with spiral rock structures, sea plants, creatures, and air bubbles (Fig. 1). In this underwater world, participants visualized their controllers as wands and were instructed to direct as many fish as possible to the reef by touching the tip of their wand to swimming fish. Variations of the program displayed the three categories of influential VR elements in series, including environment (realistic vs. fictional), graphics fidelity (8-bit vs. 32-bit), and a motivational character (present vs. not present) (Table 1). Each of the six VR element scenes was approximately 15 seconds, which balanced the need for time to allow fish to swim across the virtual room with the need for brevity to reduce fatigue and increase practicality of use in the hospital setting. The software randomized the order that participants experienced the elements within each category to minimize risk of bias related to order.
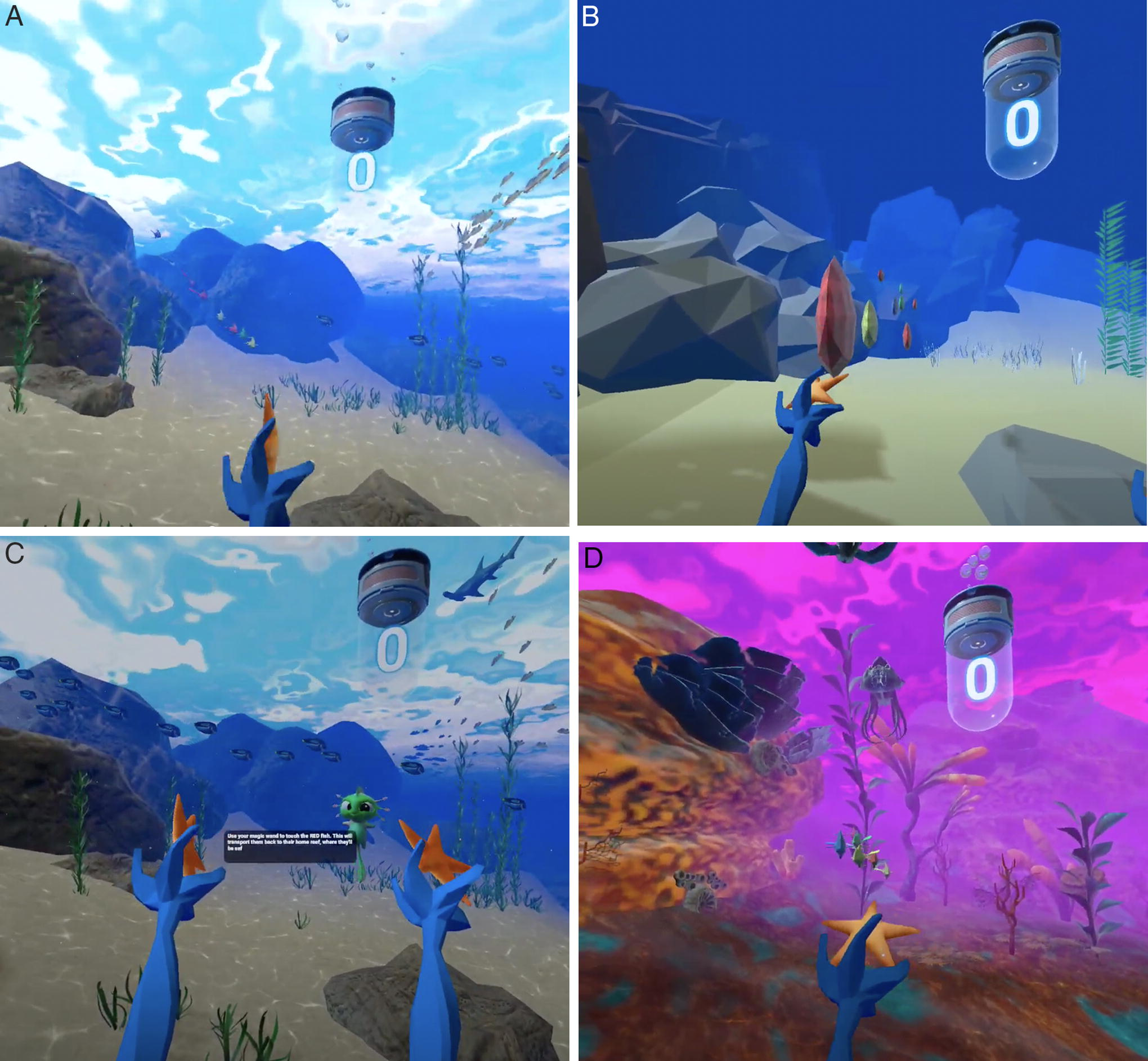
Image captures of VR application scenes displaying different design elements:
Experimental Variables in the Virtual Reality Application
Participants were seated and equipped with an Oculus Quest 2 headset (Meta, Inc., Menlo Park, CA) displaying Wonder Reef (Stanford Chariot Program, Palo Alto, CA). Upon being fitted with the headset, RAs oriented participants to Wonder Reef, and participants interacted with the differing elements in the randomized order. After each of the six VR element conditions, participants completed three questionnaires—Global Perceived Awe (GPA) survey (Supplementary Appendix S1), Perceived Vastness (PV) survey (Supplementary Appendix S2), and Perceived Need for Accommodation (PNA) survey (Supplementary Appendix S3).28,34 At the end of all conditions, participants completed the Game Engagement Questionnaire (GEQ) (Supplementary Appendix S4). 35
Variables
The primary outcome examined the self-reported awe for each of the elements within the three categories—environment, graphics fidelity, and motivational character. The elements within each category were compared to determine which most impacted awe. Group differences between pediatric patients and adult caregivers were also compared. Secondary outcomes compared the three VR categories and differentiated patient and caregiver results in terms of vastness, accommodation, and engagement, which are all related to the feeling of awe.
Measurements
The primary outcome was measured through the GPA survey, a Likert scale measuring eight emotions (awe, anger, disgust, fear, pride, sadness, amusement, joy) on a seven-point scale (Supplementary Appendix S1). 28 Each participant experienced three sets of two contrasting conditions. For example, for the set that measured graphics fidelity, each participant experienced the low resolution and the high-resolution version of the VR application in randomized order. An average low GPA awe score is 2.222 with a standard deviation (SD) of 1.417, whereas a typical awe-inducing experience has an average score of 5.250 ± 1.697. 28 Given 20% primary outcome effect size, ɑ = 0.05, and β = 0.20, the study was powered to enroll 76 pediatric and 76 caregiver participants. To account for dropouts and missing data, we targeted 100 pediatric patients and 100 caregivers.
Secondary outcomes were measured through the PV survey (Supplementary Appendix S2), PNA survey (Supplementary Appendix S3), and GEQ (Supplementary Appendix S4). 34 ,35 The PV survey measured four aspects of vastness (What I watched provided me with a deep sense of vastness; I felt small in front of what I watched; I felt meaningless in front of what I saw; I felt my sense of self diminish in front of what I saw) on a 7-point Likert scale. 34 Similarly, the PNA survey measured three aspects of accommodation (It was hard to grasp what was going on; I felt confused and bewildered in front of what I saw; I was struck by the VR) on a 7-point Likert scale. 34 The GEQ posed 19 questions investigating immersion, presence, flow, psychological absorption, and dissociation on a 7-point Likert scale. 35
The GPA, PV, and PNA surveys were selected for this study because of its use in seminal work and its high internal consistency for the latter two (Cronbach’s α = 0.77 and 0.81, respectively). 28 The GEQ was chosen because this scale has shown high internal consistency too (Cronbach’s α = 0.85). 35
Bias
To reduce bias, participants were blinded to which VR element was being tested, and the order within categories was randomized. RAs were unable to be blinded to the VR element being tested due to survey administration. Data were analyzed by a statistician blinded to the study outcomes.
Statistical methods
Continuous demographic data were reported as mean ± SD. Categorical variables were reported as percentages. For primary and secondary outcomes, the interaction effects were analyzed using repeated measure ANOVA tests because each participant completed two conditions per category. Within-group and between-group differences were reported. Due to the multiple testing per category,
Results
Participants
A total of 202 participants were recruited, of which 101 were pediatric patients and 101 were adult caregivers. Pediatric patients were 14.4 ± 6.4 years, whereas caregivers were 38.8 ± 12.0 years. Within the patient group, 53.5% were male, 45.5% were female, and 1% chose not to disclose; within the caregiver group, 53.5% were male and 46.5% were female. Among patients, 37.6% had zero previous encounters with VR; among caregivers, 55.4% had zero previous encounters (Table 2).
Participant Demographics
Multiple answers allowed.
VR, virtual reality.
Twenty-three participants did not complete the intervention due to meeting exclusion criteria (n = 3), having inadequate time to complete the intervention (n = 18), or losing interest (n = 2) (Fig. 2). A final cohort of 179 participants were analyzed, of which 88 were patients and 91 were caregivers.
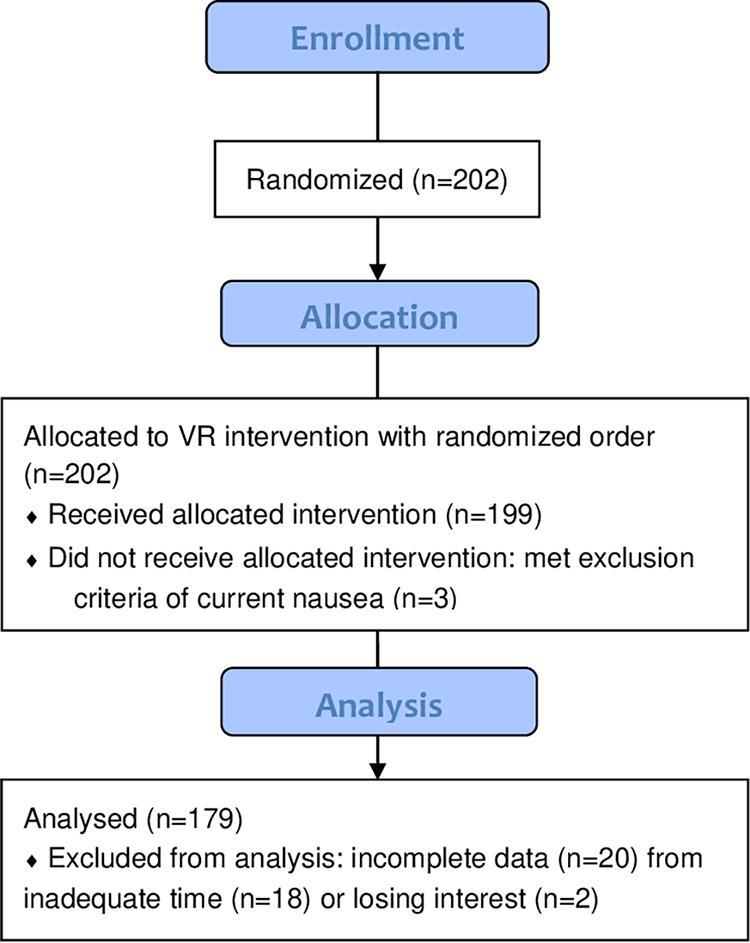
Consolidated Standards of Reporting Trials Flow Diagram of participant enrollment, allocation, and analysis.
Primary outcome: Global perceived awe
Fictional and realistic environments did not have an impact on GPA results for patients (
Effect of VR Design Elements on GPA, PV, and PNA
GPA, Global Perceived Awe; PNA, Perceived Need for Accommodation; PV, Perceived Vastness; VR, virtual reality. Bold values indicate P < 0.05.
Secondary outcome 1: Perceived vastness
For patients, PV was lower in the realistic condition than in the fictional environment condition (
Between 32-bit and 8-bit graphics fidelity, there was no difference for patients (
The change in motivational character presence did not have an impact on PV for patients (
Secondary outcome 2: Perceived need for accommodation
The change in environment had an impact on patients’ PNA (
The change in graphics fidelity had a marginal impact on patients (
The change in motivational character presence did not have an impact on PNA for patients (
Secondary outcome 3: Engagement
Caregivers showed increased level of game engagement compared with pediatric patients (p = 0.002, Cohen’d = −0.472). Pearson’s correlation demonstrated that all measures of awe used (GPA, PV, PNA) were positively correlated with engagement (Table 4). GPA was weakly correlated with game engagement for patients and caregivers (
Correlation between GPA, PV, and PNA with Engagement
GPA, Global Perceived Awe; PNA, Perceived Need for Accommodation; PV, Perceived Vastness. ***P < 0.001.
Discussion
Self-reported awe among VR elements for both patients and caregivers revealed no differences between the elements within each category. However, in the context of environment, patients reported more awe compared with adult caregivers regardless of whether it was fictional or realistic. Regarding vastness, the results indicated an increase for patients when exposed to a fictional environment, whereas higher graphics fidelity increased vastness for caregivers. With respect to accommodation, a fictional environment increased the sense in patients. Regarding engagement, caregivers exhibited higher levels of engagement than patients. All measures of awe were positively correlated with increased engagement for both adult caregivers and pediatric patients, most significantly with PV.
When examined by participant group, these results underscore age-related differences in the likelihood of experiencing awe while using VR. Pediatric participants demonstrated a greater propensity toward awe in response to VR. The presence of a fictional environment significantly enhanced their sense of awe, amplifying the PV of the VR scene and increasing their need for accommodation. When designing VR software for this age, particularly in hospital settings, incorporating fictional settings would be more likely to elicit awe. Conversely, adult caregivers exhibited a higher level of awe in response to higher graphics fidelity within, enhancing their sense of vastness. Therefore, for adult audiences, prioritizing graphics fidelity may improve awe. This distinction of the impact of VR elements on different age groups highlights the importance of tailoring software design to the audience’s age. Given the resource-intensive nature of software development, the identification of specific VR factors that contribute positively or negatively to awe experiences is pivotal.39–41 For instance, the insignificant influence of a motivational character on awe in both patients and caregivers suggests that this element may be deprioritized during application development, allowing developers to allocate resources more efficiently.
The clinical implications of these findings hold particular significance for health care practitioners, since increased awe in pediatric patients and their caregivers improves engagement in medical care, anxiety relief, and the patient experience.22–24 Awe predicts greater well-being, less stress, and less somatic health symptoms like body pains and trouble sleeping.22,23 Notably, these improvements held when controlling for trait awe and baseline well-being, suggesting that these changes are driven by daily experiences and not by individual dispositions. To elucidate these awe pathways benefitting mental and physical health, five awe factors have been modeled—(1) neurophysiology shifts of increased vagal tone, decreased sympathetic arousal, reduced inflammation, and decreased oxytocin, (2) diminished sense of self, (3) enhanced prosociality, (4) increased integration into social networks, and (5) elevated sense of meaning. 24 All five contribute to decreased stress, anxiety, depression, and increased emotional, social, and psychological well-being. 24 With the increasing prevalence of pediatric anxiety, identifying effective and safe treatments that increase awe is imperative. 42 VR is a valuable anxiolytic adjunct, and because awe is predictively associated with anxiolysis and engagement, these results highlight the differential impacts of specific VR elements on awe experiences.22–24 For pediatric patients, the choice of a fictional environment in VR software emerges as significant in enhancing awe, whereas the effect of high graphics fidelity is marginally significant. For adult caregivers, the significance of high graphics fidelity in inducing awe is notable, whereas conclusions regarding the impact of the environment and motivational characters are less clear. These insights provide clinicians with valuable guidance when selecting VR applications for patients and caregivers. Thoughtful consideration of content that is most effective in inducing awe can enhance the therapeutic benefits of VR experiences.
There were several limitations. First, the exclusion of patients under 6 years due to incompatibility with the headset limits generalizability to younger children. Similarly, the age of included patients was broad, which may have obscured differential findings within different age groups. However, analyzing the data by subgroups would have reduced statistical power or required a much larger sample, which was outside of the scope of this study. Second, the underwater theme, first-person gameplay, and VR modality of this application introduced potential limitations in terms of generalizability. Participant responses to this specific application may limit the applicability of the results to a more diverse range of immersive experiences (e.g., space environment as opposed to underwater, augmented reality as opposed to VR). Nonetheless, it is important to understand key parts of effective VR gameplay in the hospital setting. Third, the study was conducted at a single institute in Northern California. The cultural and demographic characteristics of those at LPCHS may differ from other regions, limiting external validity. Fourth, while the surveys were previously validated, they may not capture all nuances of engagement and awe. The number of measures was limited to mitigate survey fatigue, but it introduced the possibility that some aspects of participant experiences may not have been fully captured. Fifth, as GPA showed minimal differences between VR elements, the majority of conclusions were dependent on secondary outcomes of PV and PNA. PV and PNA are documented themes comprising awe, but it should be noted that there were minimal changes with self-reported awe. 21
Conclusion
This study revealed that a fictional environment had a pronounced effect in increasing awe among pediatric patients, while heightened graphics fidelity was more impactful in eliciting awe in caregivers. The presence of a motivational character did not demonstrate an influence on awe for either patients or caregivers. The development of motivational character features in VR applications may not be as worthwhile an investment as the development of fictional environments and the enhancement of graphics fidelity.
Next steps involve investigating additional VR attributes that may influence awe, such as the presence of sound, the choice between a first-person and third-person perspective, and the distinction between active and passive engagement. Additionally, different themes will be explored beyond the underwater environment to assess the generalizability of the findings.
Footnotes
Acknowledgment
The authors would like to thank Faith Collins, Ahtziri Fonseca, Brian Ko, Maria Menendez, Man Yee Suen, Janet Titzler, Craig Yamaguchi, and Michelle Zuniga-Hernandez for their assistance with this study.
Authors’ Contributions
E.M.H.: Conceptualization, Methodology, Software, Investigation, Data Curation, Writing—Original Draft, Writing—Review and Editing, Visualization, Project Administration, and Funding Acquisition. F.A.: Software, Investigation, Review, and Editing. B.S.-K.L: Investigation, Review, and Editing. R.B.: Investigation, Review, and Editing. A.G.: Investigation, Review, and Editing. L.Z.: Formal Analysis, Data Curation, Visualization, Review, and Editing. S.F.: Investigation, Review, and Editing. M.R.: Investigation, Review, and Editing. S.T.R.: Software, Resources, Supervision, Funding Acquisition, Review, and Editing. E.W.: Software, Resources, Supervision, Funding Acquisition, Review, and Editing. O.R.: Conceptualization, Methodology, Software, and Investigation. T.J.C.: Conceptualization, Methodology, Software, Resources, Writing—Review and Editing, Supervision, Project Administration, and Funding Acquisition.
Author Disclosure Statement
The authors S.R., E.W., and T.C. are on the board of a nonprofit (Invincikids, Inc) that seeks to distribute immersive technology to hospitalized children at no cost. They receive no compensation for their roles at Invincikids, Inc. The Stanford Chariot Program has received philanthropic donations from Meta Inc., and Magic Leap, Inc. S.R. has received consultation fees from Apple, Inc. All other authors declare no competing interests or conflicts of interest.
Funding Information
This research was supported by an internal grant from the Medical Scholars Research Program from Stanford University School of Medicine and the Stanford Chariot Program.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.