
Abstract
Objective: The aim of this study was to investigate the frequency of sister chromatid exchanges (SCEs), the presence of cytostaticity, cytotoxicity, and therefore, the possible genetic instability in patients with chronic renal failure (CRF) in human cultured peripheral blood lymphocytes. Methods: Peripheral blood lymphocytes were cultured from 32 patients with CRF (average 55.2 years) and 18 healthy blood donors (average 44.6 years), and the SCE method was applied afterward. The increase in SCE frequency was evaluated as an immediate DNA damage index, while the reduction in the values of the proliferating rate indices was evaluated as a cytostatic index and the mitotic indices as a cytotoxic index was also measured. Results: A significant increase in the SCE frequencies along with a significant reduction in mitotic indices was observed in patients with CRF compared with the controls. It is notable that there was no significant difference in SCE levels among patients with CRF and cancer, and patients with CRF alone. Conclusions: This study illustrates increased genetic instability in patients with CRF. These results could also be of a great importance in early diagnosis to prognosticate a possible generation of neoplasm in the future.
Introduction
C
Genetic factors, environmental factors, and their interactions are implicated in the development of ESRD. Also, there are a number of candidate genes, which are responsible for the initiation of renal failure or affecting its progression (Buraczynska and Ksiazek, 2001). ESRD patients have an increased risk of carcinoma of the kidney, as a result of development of a disproportionately high number of papillary renal-cell carcinomas (RCCs) (Chudek et al., 1998; Hughson et al., 1999).
RCCs are responsible for the deaths of 3-4% of the patients with ESRD. The clear-cell carcinoma of the kidney shows a deletion of gene sequences in the short arm of chromosome 3 (3p). In contrast to the general population, RCCs with 3p abnormalities represent only a small proportion of the renal carcinomas in ESRD tumors. RCCs that arise in ESRD patients have genetic changes that are similar to those found in sporadic tumors (Hughson et al., 1996a, 1996b).
RCCs display different chromosomal abnormalities according to their morphology; gains of chromosomes 7 and 17 and loss of Y are commonly observed in papillary lesions, whereas loss of 3p sequences (3p21.3 region is among the most frequently lost) and multiple losses of specific chromosomes are found in nonpapillary and chromophobe cell carcinomas, respectively. Also occasional gain of chromosome 16 is observed in papillary tumors (Gronwald et al., 1999; Huebner, 2001). Further, the fragile histidine triad gene is localized at the most common fragile site at chromosome 3p14.2. This fragile histidine triad gene and the p53 tumor suppressor gene are targets of different environmental agents (Chudek et al., 1998; Dreijerink et al., 2001).
Chromosomal fragility is defined as the phenomenon during which automatic mutations (point, structural or numerical) appear or are produced by several natural, chemical, or biological factors in different places of one or more chromosomes, of one or more cells, in increased levels as regards the genetic material of normal cells (Sutherland, 1988; Gisselsson, 2001; Ruiz-Herrera et al., 2002). The fragile chromosomal sites are divided into two groups: the rare and the common ones (Berger et al., 1985). The rare fragile chromosomal sites are hereditary in a codominant way and are called the hereditary fragile regions. The original definition of a fragile site by Sutherland (1979) refers to the rare chromosomal regions with chromosomal fragility. As far as their molecular operation mechanism is concerned, little is known (Ruiz-Herrera et al., 2002). An increased frequency of structural chromosomal aberration can be caused by a high frequency of double-stranded fractures of DNA. In normal cells, DNA breaks and lesions are traced and repaired by a network of elaborate natural mechanisms (Wang et al., 2000; Abraham, 2001). They are thought to be an indication of chromosomal instability that could be the foundation of structural reregulation and/or genetic enrichments. There are many assumptions about the molecular basis of the fragile chromosomal sites, and it is believed that it is mostly the structure of DNA and not the proteinaceous components of the chromosomes which play a part in the fragility of these chromosomal regions. Even if another chromosomal region is involved, it is fairly close to the fragile sites (Sutherland and Hecht, 1985). In the above, some permutable molecules (Hoegerman and Rary, 1986) and an intercalary deoxyribonucleic sequence of heterochromatin are included (Laird, 1987; Laird et al., 1987; Moustacchi, 2000).
Diseases that show a significantly increased fragility in cellular genetic material are Fanconi's anemia Bloom syndrome, which is associated with male subfertility, Weiner syndrome, ataxia telangiectasia, xeroderma pigmentosum, multiple sclerosis, hyperparathyroidism, and asthma (Moustacchi, 2000; Abraham, 2001; Gisselsson, 2001; Taylor, 2001; Honma et al., 2002; Chudek et al., 2007; Lialiaris et al., 2009). However, apart from the above mentioned diseases, the fragility of the genetic material is also induced by biological, natural, and chemical environmental mutation factors (Lialiaris et al., 1990; Mourelatos et al., 1995; Maskaleris et al., 1998; Raptopoulou et al., 1998; Papachristou et al., 2006; Mpountoukas et al., 2008). This phenomenon can be studied and its severity can be estimated through the method of sister chromatid exchanges (SCEs).
The fragility of chromosomes in patients with renal failure and/or renal cancer was evaluated with the simultaneous determination of three cytogenetic parameters: (a) the levels of SCEs, (b) the proliferation rate index (PRI), and (c) the mitotic index (MI) in human lymphocyte cultures. The method of SCEs has been proposed as a very sensitive, simple, and rapid method for detecting mutagens and/or carcinogens, antimutagenic agents, and monitoring genetic diseases that are characterized by chromosome instability, while its application is very useful for monitoring and improving chemotherapeutic techniques in vitro and in vivo. Further, the other two indices, PRI and MI, are useful indicators of the cytostatic and cytotoxic properties of various agents (Carrano and Natarajan, 1988; Das, 1988; Lialiaris et al., 2007; Öztürk et al., 2008; Papachristou et al., 2008; Karapidaki et al., 2009a, 2009b). Elevated SCEs were found in ESRD patients compared with the healthy donors (Pernice et al., 2006). It is imperative that we develop a clearer understanding of the pathogenesis of nephropathy so that individuals at risk can be identified and treated at earlier, potentially reversible, stage of their illness (Satko et al., 2005).
Mitomycin C (MMC) is a known antineoplastic agent that can enhance the frequency of SCEs. It has also been demonstrated that MMC can induce SCEs in human peripheral lymphocytes (Littlefield et al., 1983; Papachristou et al., 2006). So we used MMC to evaluate the sensitivity of CRF patients' DNA.
Materials and Methods
Heparinized blood samples were obtained from 32 patients with CRF (average 56.2 years), 18 of them also had cancer, and 18 healthy blood donors were used as controls (average 44.6 years), none of whom was under any medication or was a smoker. Cultures of peripheral lymphocytes were prepared in universal containers by adding 11 drops of whole blood to 5 mL of chromosome medium B (Biochrom KG). These were incubated at 37°C for 72 h. Cells were allowed to proliferate for at least two mitotic cycles, in the presence of BrdU at a final concentration of 5 μg/mL. MMC at a final concentration of 15 ng/mL was added at the beginning of the culture period. After 70 h, 0.5 μg/mL of colcemide was added for 2 h, and at the end of the incubation period cultures were harvested. Cultures were maintained in the dark to prevent or minimize photolysis of BrdU. The chromosome preparations were stained by a modified fluorescence plus giemsa technique (Lialiaris et al., 1987; Maskaleris et al., 1998).
Scoring was performed in a blind fashion, and cells on the first, second (Fig. 1), and third and subsequent mitotic divisions were counted. To establish the PRI, 200-400 cells for each culture were counted, and the following formula was used: PRI = (M1 + 2M2 + 3M3+)/N, where M1 is the percentage of cells in the first division (both chromatids dark staining), M2 in the second (one chromatid light and one dark staining of each chromosome), and M3+ in the third and subsequent divisions (a portion of chromosome with both chromatids light staining), and N is the total number of cells counted, that is, M1 + M2 + M3+.
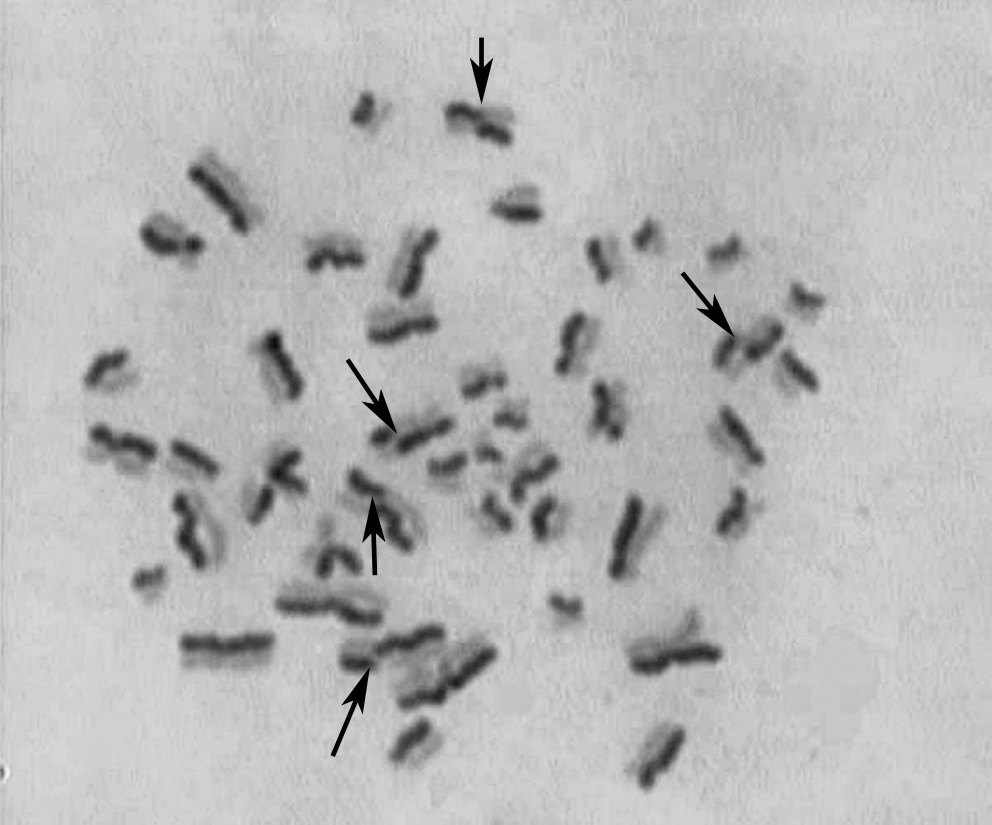
Second division metaphase, where all chromosomes have in total one light and one dark stained chromatid. Sister chromatid exchanges can be counted only in these metaphases. Black arrows show single sister chromatid exchanges.
Also, mean SCE values were evaluated only in suitable second division metaphases (20-35 metaphases for each culture), because only in these metaphases we were able to observe and count accurately the SCEs.
In addition, MIs were measured, which means the observed number of metaphases per thousand interphase nuclei. For this purpose, 2000-4000 activated lymphocytes were determined for each culture.
Statistical evaluation of MI and PRI was based on the χ2 test. For the SCE frequencies, the analysis of variance procedure and the Duncan test were used to compare the differences between groups and subsequently to calculate the pairwise comparisons (Lialiaris et al., 1992; Maskaleris et al., 1998; Mpountoukas et al., 2008). A p value <0.05 was considered as statistically significant (Maskaleris et al., 1998).
Results
Our findings illustrated that patients with CRF or renal cancer have a significant (p < 0.05) increase in mean SCE frequencies having 9.23 SCEs/cell, compared with the controls having mean SCE frequencies of 4.61 SCEs/cell (Table 1A). The percentage of the increase of the SCE levels in patients was around 100.2%. As far as the PRI and the MI are concerned, both were reduced compared with the controls. The proliferating rate index was reduced slightly in patients, with a percentage of 2.8%, compared with the controls, a fact that indicates a mild cytostaticity (Table 1B).
p < 0.01 versus controls and MMC of healthy donors.
p < 0.05 versus controls of healthy donors, of patients, and versus MMC of controls.
p < 0.01 versus controls and MMC of healthy donors.
SCEs, sister chromatid exchanges; MMC, mitomycin C.
On the other hand, MI was reduced significantly (p < 0.01) in CRF and renal cancer patients compared with the controls, with a percentage of 64.4%, which reflects a high cytotoxicity. Also, it is important to be mentioned that these three cytogenetic indices had no significant difference among the patients with CRF and those with CRF and renal cancer. (Tables 1A and 1B).
Finally, MMC showed a statististically significant increase of SCEs (p < 0.05) in CRF patients in comparison to healthy donors treated with the same MMC concentration. Each culture with MMC demonstrated a highly statistically significant increase compared with the control cultures of healthy donors and patients.
Discussion
An increase in the levels of chromatid exchanges in metaphase chromosomes directly reflects DNA damage (caused by various agents) and consequently indicates the failure of prereplicative repair mechanisms to achieve full recovery of the damaged site, thus leading to double-strand breaks. Such breaks are repaired by postreplicative mechanisms such as homologous recombination and nonhomologous end joining (Lialiaris et al., 1987, 1988; Mourelatos et al., 1987; Sonoda et al., 1999; Johnson and Jasin, 2000).
High micronuclei frequencies in long-term hemodialysis and advanced CRF patients may result from decreased DNA repair, which reflects genomic damage and may contribute to the increased cancer incidence in these patients (Stopper et al., 1999). Numerical and structural abnormalities of karyotype were observed in patients undergoing chronic peritoneal dialysis, such as hyperdiploidy and hypodiploidy (Dimkovic et al., 1994).
A patient with renal neoplasm showed trisomy of chromosomes 5, 16, and 20 and deletion of chromosome Y (Buraczynska and Ksiazek, 2001). The chromosome (p14.2; q24.1) translocation t(3;8) has been associated with hereditary renal cancer. Based on the cytogenetic analysis, the 3p14 region has been independently implicated as harboring a tumor suppressor gene critical to kidney and lung cancer development (Boldog et al., 1993; Ishikawa et al., 1993).
In our study, we studied the genetic stability of the nucleic DNA of patients suffering from CRF using the method of SCEs. Chromosomal fragility is defined as the phenomenon during which automatic mutations (point, structural, or numerical) appear or are produced by several natural, chemical, or biological factors in different places of one or more chromosomes, of one or more cells, in increased levels as compared with the genetic material of normal cells (Gisselsson, 2001; Ruiz-Herrera et al., 2002). The method of SCEs has been proposed as a very sensitive, simple, and rapid method for detecting mutagens and/or carcinogens, antimutagenic agents, and monitoring genetic diseases that characterized from chromosome instability (Carrano and Natarajan, 1988; Das, 1988; Lialiaris et al., 2008, 2009; Mpountoukas et al., 2008; Karapidaki et al., 2009a).
The findings show that the DNA of patients with CRF is prone to have damage to its structure as a result of the inability of metatranslational repair mechanisms to fix them, which is easily considered with a glance at the very high levels of SCEs measured to metaphases of peripheral lymphocytes of patients. These results were confirmed from the simultaneous increase of SCEs in cultures treated with the MMC. Further, a cytostatic and cytotoxic action of MMC on CRF patients was observed compared with the controls. The high frequency (a doubling effect) of SCEs in chromosomes of CRF patients is also noticed compared with that of the chromosomes of healthy donors. The inability of CRF patients' lymphocytes to promote their own mitotic cycle, which is demonstrated by the low PRI and MI, shows that they get over the damage happening during DNA synthesis with difficulty. A combination of spontaneous or induced genotoxic, cytotoxic, and cytostatic effects on CRF patients can lead us to improve a new diagnostic process to identify the genetic instability in peripheral blood lymphocytes of CRF patients. These findings show a new way that helps in indicating the SCE assay for premature diagnosis of neoplasm generation in patients with CRF. Further, any medication should be prescribed for these patients in consideration of genetic instability.
Footnotes
Disclosure Statement
No competing financial interests exist.