
Abstract
Tourniquets are often used to provide a bloodless operating field. However, they carry the risk of adverse effects caused by DNA damage from the free radicals generated during postischemic reperfusion of the blood. The aim of this study was to evaluate the cytogenetic damage caused by postischemic reperfusion on peripheral lymphocytes of five women and six men undergoing total knee arthroplasty “bloodless” operation using samples received before, during, immediately, and 1 h after the operations. The sister chromatid exchange assay was applied to peripheral blood lymphocyte cultures and the levels of sister chromatid exchanges were analyzed as a quantitative index of genotoxicity, along with the values of mitotic index and proliferation rate index as qualitative indices of cytotoxicity and cytostaticity, respectively. We observed that postischemic reperfusion induced cytogenetic damages specifically through reperfusion. DNA effects were most pronounced after tourniquet release and declined afterward without returning to preischemic baseline values. Our findings suggest the presence of a functional association between postischemic reperfusion and cytogenetic damage that may have important clinical implications.
Introduction
P
Lymphocytes have been used to monitor the systemic effects of stress response (Vamvakopoulos, 1995) to exogenous (Vakalis et al., 1999; Georgopoulou et al., 2000; Sioutopoulou et al., 2006; Satra et al., 2009) or endogenous (Vamvakopoulos et al., 1992; Nomikos et al., 2001, 2009; Athanassiou et al., 2009) stimuli at either the molecular (Vamvakopoulos et al., 1977, 1980) or chromosomal (Vamvakopoulos et al., 1993a, 1993b; Vamvakopoulos and Sioutopoulou, 1994) level.
Sister chromatid exchanges (SCEs) are related to DNA replication and provide a very sensitive and rapid method for DNA damage detection induced by physical, chemical, or biological mutagens (Lialiaris et al., 1988; Akritopoulou et al., 2009), antimutagenic agents and carcinogens, and/or defects in DNA repair (Lialiaris et al., 1990, 1992, 2009; Ozturk et al., 2008; Digkas et al., 2010a). SCE assay is the basis for assessment of genotoxicity index, cytostaticity index (proliferation rate index [PRI]), and cytotoxicity index (mitotic index [MI]) (Digkas et al., 2010b).
The aim of this study was to perform comparative follow-up evaluation of cytogenetic damage on peripheral lymphocytes of patients undergoing tourniquet-assisted limb surgical operation.
Materials and Methods
We studied 11 patients, 5 women and 6 men aged between 60 and 75 years, with a mean age of 69 years. Peripheral blood was sampled four times for each patient. The first blood sample was collected at 24 h before the operation of total knee arthroplasty (Fig. 1). The second sample was collected during the first hour of tourniquet application and the third was taken immediately after the release of tourniquet. The last sample was collected at 1 h after tourniquet release. The operations lasted for 100-120 min, and 6 h after the release of tourniquet and Esmach, the patients received a preventive anticoagulant, low-molecular-weight heparin injections.

Application of Esmach and Turniquet.
Peripheral blood lymphocyte cultures were prepared in universal containers by adding 11 drops of whole blood to 5 mL Chromosome Medium B (Biochrom KG). The cultures were subsequently infused with 100 μL 5′-bromo-deoxyuridine (BrdU) to a final concentration of 6 μg/mL and incubated at 37°C for 72 h. After 70 h, 50 μL colcemide (10 mg/mL) was added for 2 h, harvested by centrifugation, exposed to hypotone KCl (0.075 M) at 37°C for 17 min, washed 3-4 times with FIX solution (1 acetic acid : 3 methanol), and smeared on microscopic slides following standard procedures.
Chromosome preparations were stained using the Fluorescence plus Giemsa technique. The slides were immersed in Hoechst solutions for 20 min, overlaid with 4-5 drops of Mclivain's buffer (pH 8), covered with cover slips, exposed to ultraviolet radiation for 1 h and 30 min, and stained with 5% Giemsa for 12 min (Goto et al., 1978).
Scoring was performed in a blind fashion and three indices were evaluated: (a) SCEs, which is a qualitative and quantitative index of genotoxicity; (b) PRI, which is a qualitative index of cytostaticity; and (c) MI, which is a qualitative index of cytotoxicity.
All indices were evaluated in all samples obtained for each patient after the various treatments. Mean SCE values were evaluated from 20 well-spread second-division metaphases, which consisted of 46 chromosomes (Fig. 2). To establish the PRI, 200 cells were counted and the following formula was used: PRI = (M1 + 2M2 + 3M3+)/(M1 + M2 + M3+), where M1 is the number of cells in the first division, M2 in the second, and M3+ in the third and subsequent divisions.
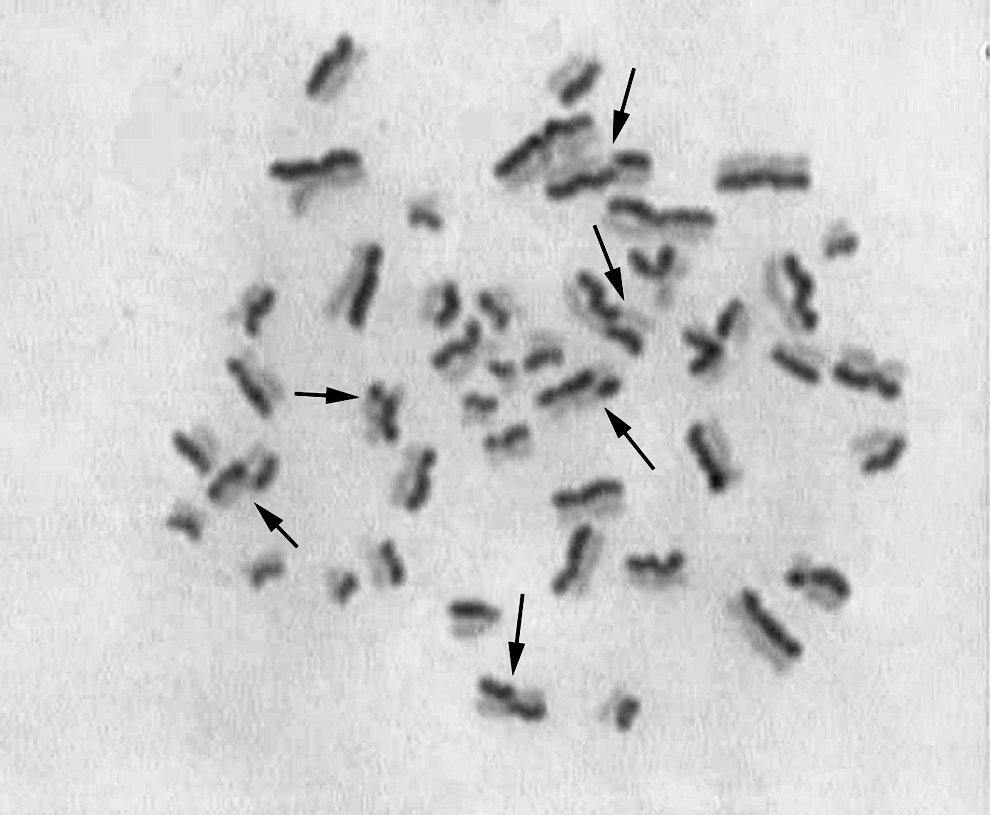
Second-division metaphase, where all chromosomes have in total one light- and one dark-stained chromatid. Sister chromatid exchanges can be counted only in these metaphases. Black arrows show sister chromatid exchanges.
MIs were derived by dividing the number of metaphases to the number of interphase nuclei of peripheral blood lymphocytes in each sample.
To compare various treatments, logarithmic transformation of SCE values was performed with the use of one-way analysis of variance and the Duncan test as far as pairwise comparisons were concerned. The evaluation of MI and PRI was based on χ2 test. A probability p < 0.05 was considered statistically significant (Maskaleris et al., 1998).
Results
Using the indices of the first sample, obtained prior to individual exposure to potential genotoxic agents, as a control, we concluded that SCEs did not increase significantly (p > 0.05) during tourniquet application (Table 1). On the contrary, SCEs of lymphocytes of the third sample were significantly higher (p < 0.05) from those of the other samples, suggesting induction of genotoxic phenomena by tourniquet application and release. An hour after tourniquet release, SCE levels returned to near those counted before the application of tourniquet.
The SCE frequency was based on 230 second-division metaphases. For the PRI 1200 metaphases and for the MI 22,000 activated cells were scored, respectively, for each culture. Results were based on 11 experiments with the same culture protocol.
p < 0.05 versus all the others.
p < 0.05 versus 1 and 2.
SCEs, sister chromatid exchanges; SEM, standard error of the mean; PRI, proliferation rate index; MI, mitotic index.
PRI was not affected significantly (p > 0.05) by tourniquet application. It is important to mention that lymphocytes appeared less capable to enter mitotic cell cycle immediately after tourniquet release, as shown by PRI value of the third sample, which was the lowest.
Similarly, MI did not change significantly (p > 0.05) during tourniquet application. Immediately after tourniquet release and 1 h later, MI values were significantly lower (p < 0.05) than those of the first sample (control). They remained stably low for at least 1 h, according to the result of the fourth sample, indicating the difficulty of lymphocytes to overcome the cytotoxic effect of tourniquet.
Discussion
The tourniquet is a very useful tool that provides a bloodless operating field and is of vital importance in emergency cases when injuries are extreme, as in combat fields (Estebe et al., 1996; Westman et al., 2007; Sambasivan and Schreiber, 2009; Tien et al., 2009). However, it carries a high risk of adverse effects, because its improper and either tight or prolonged application may cause injuries in the muscles and nerves, limb loss and death due to increased bleeding (Hatzipantelis et al., 2001; Starnes et al., 2006; Kragh et al., 2008). The optimal period of tourniquet application is of major importance for the recovery of the tissue, as shown by the negative correlation between time of tourniquet application and the recovery peak of oxyhemoglobin in a rat model (Kim et al., 2009). Clinical studies showed that tourniquet application resulting in ischemia affected severely the skeletal muscles, leading potentially to muscle atrophy during immobilization following orthopedic surgery (Appell et al., 1993). Albani et al. (2000) reported that the short ischemic period during aortic clamping and the subsequent reperfusion resulted mainly in ultrastructural changes in patients with reparative abdominal aortic aneurysm.
Ongoing efforts aim to reduce or extinguish the cytotoxic effects of tourniquet application. N-Acetylcystein treatment, which is thought to protect organs against free radicals, may increase the risk of remote kidney injury (Mazzon et al., 2001; Sehirli et al., 2003; Laisalmi-Kokki et al., 2009). Akyol et al. (2006) reported that propofol and caffeic acid phenylethyl ester prevented tourniquet application-dependent lung injury in a rat model, indicating that these two agents may have protective effect in injury caused by ischemia-reperfusion. Clinical studies propose the usage of propofol anesthesia in ischemia-reperfusion injury during tourniquet-using surgery because of its antioxidant properties (Aldemir et al., 2001). Two other studies on rats showed that Urtica dioica, an annual perennial herb, and zinc aspartate attenuate ischemia-reperfusion injury (Cetinus et al., 2005; Atahan et al., 2007). It has also been found that allopurinol and vitamin E diminish the occurrence of edema and oxidative stress in postischemic skeletal muscle (Appell et al., 1997).
Tourniquet-induced ischemia and subsequent reperfusion alters glutathione metabolism, indicating that oxidative stress occurred during tourniquet application (Westman et al., 2007). Experiments in rat dorsal root ganglion showed upregulation of neuronal growth factor and NT3 mRNA expression and transient downregulation of neurotrophil receptors within 4 h and 1-2 h after tourniquet application, respectively. The first is a sign of acute response to protect dorsal root ganglion neurons that lost material because of tourniquet application, whereas the second is a result of neurotrophins deprivation caused by the same cause, which interrupted retrograde deprivation (Abe et al., 2004).
Willy et al. (2000), using cell gel-electrophoresis technique, found that tourniquet induced genotoxic effects in human leukocytes through ischemia-reperfusion injury, presumably as a response to oxidative stress during reperfusion. In this study, we showed that tourniquet usage had genotoxic and cytotoxic effects on peripheral lymphocytes, which is in agreement to the study by Willy et al. We also showed that oxidative stress had a toxic effect on cells and that the low MI values of cells remaining 1 h after tourniquet release suggested that their damage might be irreversible, driving them to apoptosis.
Study of more samples collected for longer periods after tourniquet release would better dwell on the dynamics of lymphocyte mitotic cycle, whereas study of different time durations of tourniquet application would resolve whether genotoxicity is affected in a time-dependent manner just like edema and oxidative stress of skeletal muscle cells (Duarte et al., 1997). In conclusion, our study revealed that tourniquet application increased chromosome fragility and disturbed cell kinetics, and its highest level of damage was reached immediately after reperfusion.
Footnotes
Disclosure Statement
No competing financial interests exist.