
Abstract
In this work, we evaluated the frequency of prothrombotic defects associated with deep venous thrombosis (DVT) in southern Chilean subjects. A total of 261 individuals, 87 patients with DVT confirmed by Doppler ultrasonography and 174 controls, were included in this study. Factor V and factor VIII levels, activated protein C (APC) resistance, and lupus anticoagulant detection were assayed by clotting methods. Basal homocysteine was quantified by immunoassay, and the polymorphisms in factor V (F5), methylenetetrahydrofolate reductase (MTHFR), and cystathionine β-synthase (CBS) genes were genotyped by molecular methods. The most frequent defects were APC resistance, hyperhomocysteinemia, and increased levels of factor VIII. We observed a complete absence of the F5 G1691A variant in the studied population, and the frequency of MTHFR C677T polymorphism was significantly different between patients and controls (odds ratio = 3.2; 95% confidence interval, 1.513-6.735; p = 0.016). In addition, subjects carrying the homozygous MTHFR 677TT genotype exhibited higher levels of plasma homocysteine. Our data suggest that the APC resistance is the most important defect in Chilean patients with DVT. However, this phenotype is not associated with the presence of the F5 G1691A variant. In addition, only MTHFR C677T polymorphism constituted a molecular biomarker of DVT in Chilean population.
Introduction
V
In Chile, poor evidence exists about the frequency of classical risk factors in patients with deep venous thrombosis (DVT). In addition, several studies have suggested that the Chilean population present a genetic pool with Amerindian predominance (Moraga et al., 2000; Rocco et al., 2002; García et al., 2006). Thus, the aim of the present study was to evaluate the frequency of classical prothrombotic defects associated with DVT susceptibility in southern Chilean subjects.
Materials and Methods
Subjects
A total of 261 individuals, 87 unrelated patients (40 males and 47 females) with diagnosis of DVT confirmed by Doppler ultrasonography and 174 healthy controls with similar ages, were included in this study. None of the subjects had chronic hepatic diseases or thrombosis secondary to malignant diseases. Demographic data and history of hypertension, diabetes mellitus, hypercholesterolemia, and familial history of thrombosis were assessed in each subject. We calculated the body mass index (body weight [kg] divided by square of height [m]) to assess obesity. The study protocol was approved by the local Ethics Committee, and all subjects gave written informed consent according to the basic principle of biomedical investigation enumerated in the Helsinki declaration.
Functional analysis
Functional analysis was determined from a blood sample collected after overnight (>12 h) fast. Factor V and VIII levels and lupus anticoagulant detection were assayed using clotting methods recommended by the International Society of Thrombosis and Haemostasis. APC functional resistance was detected according to protocol previously described (Quincampoix et al., 2001). Basal homocysteine quantification was determined using fluorescence polarization immunoassay (Abbott Laboratories).
Molecular analysis
Venous blood anticoagulated with ethylenediaminetetraacetic acid was extracted by standardized methods and genomic DNA was purified from blood leukocytes by a procedure described by Salazar et al. (1998). The polymorphisms of F5 G1691A (rs6025) and cystathionine β-synthase (CBS) 844ins68 were identified according to protocols previously described (Bertina et al., 1994; Ramsbottom et al., 1997). The methylenetetrahydrofolate reductase C677T variant (MTHFR, rs1801133) was genotyped with the following primers: 5′-ccgaagcagggagctttgag-3′ (forward) and 5′-aggacggtgcggtgagagtg-3′ (reverse). Each amplification reaction was performed in a final volume of 25 μl containing 50 ng of genomic DNA, 100 nM of each primer, 200 mM of each deoxynucleotide triphosphate, 1 unit of Taq DNA polymerase, and PCR buffer (50 mM KCl, 2 mM MgCl2, 20 mM (NH4)2SO4, 75 mM Tris-HCl, pH 9.0). The fragments were separated on a 3% agarose gel, stained with ethidium bromide, and observed on a UV transilluminator.
The correct assessment of genotypes was evaluated using a homozygous sample for restriction sites as a positive control. In addition, all gels were reread blindly by two persons without any change, and 20% of the analyses were repeated randomly.
Statistical analysis
Statistical analysis was carried out using the Sigma Stat Software, v. 2.0 (Jandel Sci.). The allelic frequencies and genotype distribution were estimated by gene counting. Differences between genotype distribution and allele frequency were tested by χ2 analysis. The odds ratio (OR) for DVT and 95% confidence interval (CI) associated with the analyzed variants were also calculated. Difference in homocysteine levels according to genotypes was evaluated by ANOVA or Student's t-test. A statistical significance of p < 0.05 was considered.
Results
The clinical and demographic characteristics of the patients with diagnosis of DVT enrolled in the study are summarized in Table 1. The frequency of functional defects is summarized in Figure 1. The most frequent abnormalities observed were an APC resistance phenotype (16.1%), hyperhomocysteinemia (13.8%), and factor VIII >150% levels (9.2%).

Frequency of functional prothrombotic defects in patients with deep venous thrombosis.
Number of individuals is given within parentheses.
p-Values from Student's t-test or χ2 test.
The genotype distribution and the relative allele frequency of the analyzed variants are shown in Table 2. An absolute absence of F5 G1691A polymorphism was observed in all studied populations (p = NS). The genotype distribution of the CBS 844ins68 variant was similar in both groups (χ2 = 0.19; p = 0.658). The OR for DVT associated with homozygous status was 1.43 (95% CI, 0.526-3.909; p = 0.478). On the other hand, the genotype distribution and allelic relative frequencies of MTHFR C677T polymorphism were significantly different between patients and controls. The homozygous genotype for MTHFR C677T was more frequent in DVT patients compared with controls (χ2 = 8.78; p = 0.0030). The OR for DVT associated with the homozygous status was 3.2 (95% CI, 1.513-6.735, p = 0.016).
MTHFR C677T: odds ratio = 3.62 (95% confidence interval, 1.513-6.735, p = 0.016). CBS 844ins68: odds ratio = 1.43 (95% confidence interval = 1.526-3.909, p = 0.478).
p-Values from χ2 test.
844ins68 is a 68-bp insertion in exon 8 of CBS gene.
F5, factor V; CBS, cystathionine β-synthase; MTHFR, methylenetetrahydrofolate reductase C677T variant; W, wild type; I, insertion.
Basal homocysteine levels according to genotypes of functional polymorphisms in genes involved in the homocysteine metabolism are shown in Figure 2. In addition, our results show that the homozygous carriers of the MTHFR C677T variant presented higher levels of plasmatic homocysteine (CC = 8.2 ± 2.3 μmol/L, CT = 8.9 ± 2.9 μmol/L, and TT = 14 ± 5.8 μmol/L; p < 0.0001).
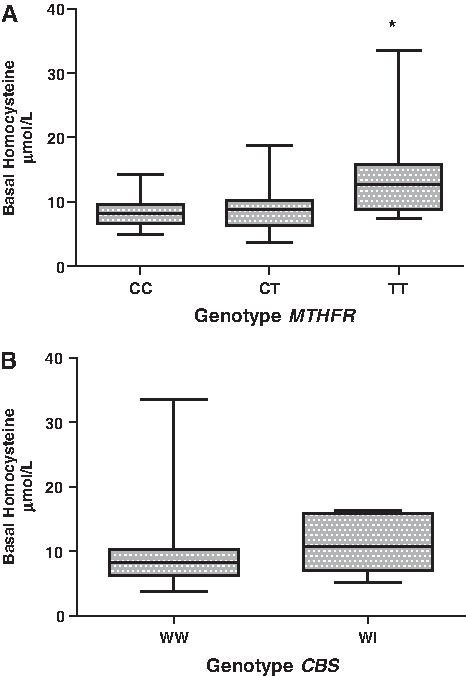
Basal homocysteine levels according to genotypes of the methylenetetrahydrofolate reductase (MTHFR) C677T (
Discussion
Thromboembolic disease constitutes an important health problem in occidental countries and results from the interaction of genetic predisposition and environmental risk factors. In the present study, we examined the frequency of classical prothrombotic defects associated with DVT susceptibility in a southern Chilean population. Our data showed the presence of several risk factors for venous thromboembolism in patients with DVT, including obesity, diabetes, hypertension, and familial thrombosis history. Other studies showed similar results (Samama, 1993; Abdollahi et al., 2003; Petrauskiene et al., 2005). A recent meta-analysis demonstrated a significant association between venous thromboembolism and obesity, diabetes mellitus, hypertension, low high-density lipoprotein cholesterol, and higher levels of triglycerides (Ageno et al., 2008).
Our results showed that the most frequent abnormality in Chilean patients with a diagnosis of DVT was APC resistance. Interestingly, the APC resistance phenotype is not associated with the presence of the F5 G1691A variant, the most common inherited prothrombotic defect. In general, the APC resistance phenotype is related to the presence of factor V Leiden polymorphism (Bertina et al., 1994; Buchanan and Rodger, 2003). This result is in accordance with a recent study realized in southern Chile that described a lower frequency of the F5 G1691A variant (Palomo et al., 2005). These apparently contradictory results may be explained by the genetic background of the Chilean population. According to several studies, the Chilean population presents a genetic pool with Amerindian predominance (Moraga et al., 2000; Rocco et al., 2002; García et al., 2006). In addition, Zivelin et al. (1997) have demonstrated that factor V Leiden polymorphism presents a founder effect in the White population. This evidence explains the higher frequency in Caucasian populations in contrast to populations with other genetic backgrounds. This finding suggests the need to search for novel variants in the F5 gene that promote the APC resistance phenotype and constitute a thrombosis risk factor in populations with a similar genetic background.
In addition, our data also show that the subjects carrying the MTHFR 677TT homozygous genotype have a higher risk of DVT. This finding provides evidence about the importance of this variant as a molecular biomarker of venous thromboembolism in Chilean subjects. In a recent meta-analysis (n = 8364 cases), it was shown that Asian and Latin American individuals carrying the 677TT genotype have a 60% increased risk of thrombosis (OR = 1.60; 95% CI, 1.27-2.02) (Den Heijer et al., 2005). On the other hand, the genotype distribution of the 844ins68 polymorphism in the CBS gene was similar in patients and controls (p = NS). Similarly, a recent study done in 6793 participants of the U.S. population showed that the Mexican Americans had a lower prevalence of the CBS 844ins68 variant than did non-Hispanic black subjects (Yang et al., 2008).
When we compared the plasma homocysteine levels according to different genotypes for the analyzed variants in homocysteine pathway genes, we observed that the MTHFR C677T homozygote carriers presented higher homocysteine levels. Similarly, other studies confirmed a positive association between this functional variant in the MTHFR gene and higher levels of homocysteine (Guéant-Rodriguez et al., 2006; Yang et al., 2008). However, we did not observe an association between the CBS 844ins68 polymorphism and the presence of hyperhomocysteinemia.
In summary, our data demonstrated that the APC functional resistance, basal homocysteine, factor VIII quantification, and lupus anticoagulant detection should be included in the basic thrombophilia study in our population. In addition, only the MTHFR C677T variant constituted a molecular biomarker of DVT in Chilean population. The total absence of the F5 G1691A confirms the poor utility of molecular detection of this SNP in our population and suggests the need to search for novel variants in the F5 gene that promote the APC resistance phenotype in the Chilean population.
Footnotes
Acknowledgments
This study was supported by grants from Dirección de Investigación, Universidad San Sebastián (DIUSS No. 5005), and Dirección de Investigación y Desarrollo, Universidad de La Frontera (DIDUFRO DI09-1007), Chile.
Disclosure Statement
None of the authors has a relationship with a for-profit company or institution. No competing financial interests exist.