
Abstract
Background and Aim: One candidate gene for colorectal cancer (CRC) susceptibility is exonuclease 1 (EXO1). It is a member of RAD2 nuclease family, which plays a major role in mismatch repair, DNA replication, and recombination. Single-nucleotide polymorphisms are shown to be related with cancer incidence. The aim of the present study was to examine the association between the L757P polymorphism at exon 13 of the EXO1 gene and the risk of CRC in Iranian patients. Methods: In this case-control study, 90 cases and 98 healthy control samples were analyzed genetically. The EXO1 polymorphism, P757L, was analyzed by polymerase chain reaction-restriction fragment length polymorphism. The obtained polymorphisms were examined for the relationship with CRC risk and also clinicopathological characteristics. Results: Our findings showed that patients with the Leu/Leu genotype have a reduced risk of CRC (adjusted odds ratio [OR] = 0.192, 95% confidence interval [CI]: 0.040-0.921) when the Pro/Leu and Pro/Pro genotypes were blended and they were considered as the reference. The Leu/Leu genotype also showed a reduced risk (adjusted OR = 0.168, 95% CI: 0.034-0.816) when the Pro/Pro genotype was a reference; nevertheless, the Pro/Leu genotype did not reveal a significant association with CRC at the same status (adjusted OR = 0.686, 95% CI: 0.367-1.284). Conclusions: Our results provide evidence diagnosing that the Leu/Leu genotype of EXO1 showed an inverse association with CRC. In addition, despite other investigations, we could define a significant association between the Leu allele and CRC (p = 0.001).
Introduction
C
The gene exonuclease 1 (EXO1; MIM #606063) belongs to the MMR system and also to the RAD2 nuclease family. It is located at chromosome 1q42-q43, contains 1 untranslated exon followed by 13 coding exons, and encodes an 846 amino acid protein (Schmutte et al., 1998; Wilson et al., 1998). EXO1 is a DNA-specific 5′-3′ nuclease binding to both MSH2 and MLH1, and it participates in DNA mismatch repair and recombination functions of MLH1 (Kim et al., 2007). The DNA repair mechanisms are essential in preventing tumor initiation and progression, and mutations or defects in the DNA repairing systems are thought to be essential for tumorigenesis (Alam et al., 2003; Peltomäki, 2003). Defects in nuclease function have been associated with complex phenotypes, such as genetic instability and elevated cancer risk.
Potentially functional polymorphisms in EXO1 might contribute to alter CRC risk by influencing the repair activity of EXO1 (Tsai et al., 2009).
It is therefore rational to hypothesize that single-nucleotide polymorphisms (SNPs) in EXO1 may be associated with the risk of CRC. In an investigation, Wu et al. (2001) determined 12 missense SNPs in the EXO1 gene; one of them is the P757L polymorphism in exon 13. Although polymorphisms in several genes have been studied in relation to CRC (Orimo et al., 2000; Toffoli et al., 2003; Adleff et al., 2004), few surveys have been conducted to determine the association between polymorphisms in the EXO1 gene and CRC risk (Wu et al., 2001; Bau et al., 2007, 2008; Chiu et al., 2008; Jin et al., 2008; Wang et al., 2009).
We sought to identify a relationship of P757L polymorphism at exon 13 of the EXO1 gene with CRC and clinicopathological findings.
Materials and Methods
Patients and controls
All patients with CRC were diagnosed, using the pathology report. They had been registered in the cancer registry unit of the Research Center of Gastroenterology and Liver Disease, Shahid Beheshti Medical University, Tehran, Iran, from October 2007 until January 2009. Control individuals were selected in the same time from subjects who referred to the hospital base with negative pathology reports.
Samples and DNA extraction
Peripheral blood samples from 90 patients with CRC and 98 healthy individuals were obtained. Genomic DNA of patients and controls was extracted from lymphocytes using a phenol-chloroform standard protocol (Sambrook and Russell, 2001).
The characteristics of the 98 healthy controls and 90 CRC patients are shown in Table 1.
SD, standard deviation.
The clinicopathological staging and histological classification were according to the criteria of the UICC Tumor-Node-Metastasis Classification of Malignant Tumors (TNM), 6th edition, 2002, Colon and Rectum (ICD-O C 18-C20).
All the patients provided signed informed consent. All procedures were approved by the ethics committee of the Research Center for Gastroenterology and Liver Diseases.
Genotyping
Genotyping analysis was performed by polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP). PCR was conducted with the forward primer 5′-CAG AAT GGT CTT AAA ATG GGT GT and the reverse primer 5′-TTC AGA ATA AGA AAC AAG GCA AC, which were prepared according to the published sequence of the EXO1 gene (accession number: AAC32259). Amplification conditions were 5 min of initial denaturation at 94°C, followed by 30 cycles of 30 s at 94°C, 30 s at 63°C, and 30 s at 72°C and then a final extension of 10 min at 72°C. The 255-bp PCR product was digested for 6 h at 37°C with MnlI (Fermentas) according to the following conditions: PCR products 10 μL, MnlI-digestion releases 153- and 102-bp fragments for the Pro allele, and a single 255-bp fragment for the Leu allele (Fig. 1). To confirm the RFLP results, 10 samples were sequenced randomly (result not shown).
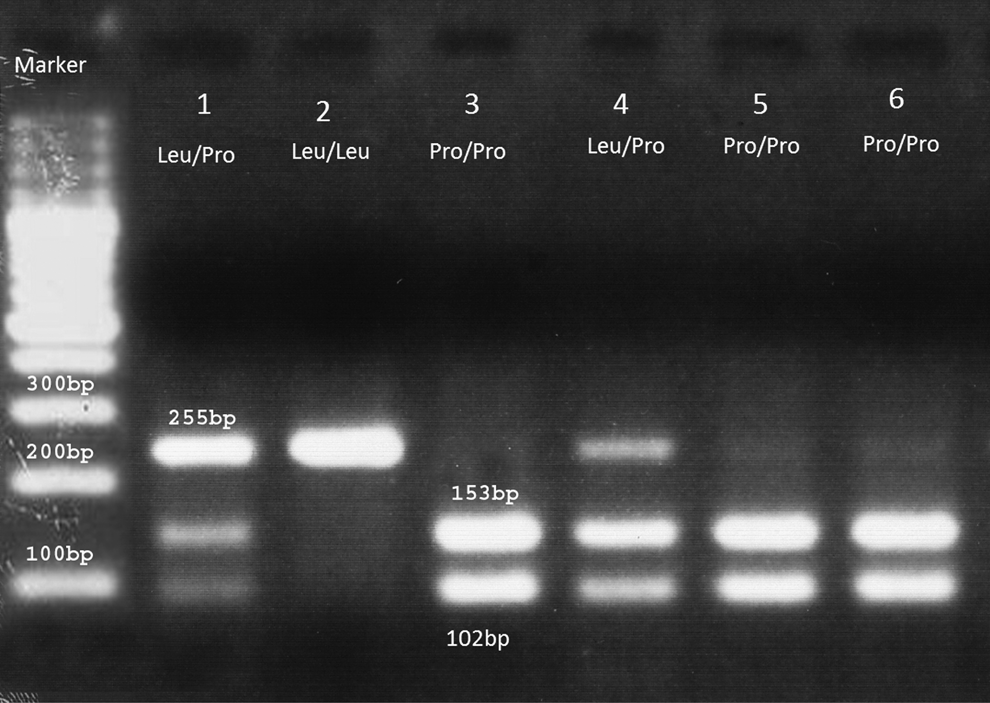
Polymerase chain reaction-restriction fragment length polymorphism analysis results. 1, Leu/Pro; 2, Leu/Leu; 3, Pro/Pro; 4, Leu/Pro; 5, Pro/Pro; 6, Pro/Pro.
Statistical analysis
Unconditional logistic regression analysis was performed to estimate adjusted and unadjusted odds ratio (OR) and 95% confidence interval (CI) as a major of association of the genotypes with the risk of CRC. OR and 95% CI were adjusted for age, sex, and smoking status. In CRC patients the association between the clinicopathology features and genotypes were examined using chi-square test.
Hardy-Weinberg equilibrium was evaluated for patients and cancer-free controls using the chi-square test. Data were recognized as significant when the statistical p value was <0.05. All the statistical analyses were carried out using SPSS version 13.
Results
We evaluated the P757L genotypes using PCR-RFLP. Digestion of the PCR product of 255 bp with the MnlI enzyme led to a single fragment of 255 bp for the Leu allele and two fragments of 153 and 102 bp for the Pro allele (Fig. 1). As demonstrated in Table 2, our findings strongly suggest that patients with the Leu/Leu genotype have a decreased risk of CRC (adjusted OR = 0.192, 95% CI: 0.040-0.921) when the Pro/Leu and Pro/Pro genotypes were combined and considered as the reference. The Leu/Leu genotype also showed a reduced risk (adjusted OR = 0.168, 95% CI: 0.034-0.816) when the Pro/Pro genotype alone was defined as the reference; however, the Pro/Leu genotype did not reveal an association with CRC at the same status (adjusted OR = 0.686, 95% CI: 0.367-1.284).
CI, confidence interval; OR, odds ratio.
When the genotype Pro/Leu was the reference, genotypes Pro/Pro and Leu/Leu did not demonstrate significant risk for CRC (OR = 1.585, 95% CI: 0.839-2.881 and OR = 0.264, 95% CI: 0.054-1.303).
Further, Pro allele frequencies in cases and controls were 82.2% and 71%, respectively, whereas Leu allele frequencies in cases and controls were 17.8% and 29%, respectively (p = 0.001). Therefore, the results showed a significant correlation between Leu allele frequency and CRC (p = 0.001; Table 2).
The genotypes Pro/Pro, Pro/Leu, and Leu/Leu were detected in 60 (66.7%), 28 (31.1%), and 2 (2.2%) of 90 cancer patients and in 51 (52.0%), 37 (37.8%), and 10 (10.2%) of 98 healthy controls, respectively (Table 2).
The distributions of genotypes in cases and controls fitted to the Hardy-Weinberg equilibrium (0.542 and 0.401, respectively).
Although we could find a significant association between tumor grades and genotypes (p = 0.033), nevertheless, there was no significant difference between genotypes and tumor characteristics including size (p = 0.098), location (p = 0.650), and TNM stage (p = 0.773; Table 3).
TNM, tumor node metastasis.
Discussion
EXO1 is the only exonuclease involved in the human MMR system, playing a critical role as both 5′-3′ and 3′-5′ nucleases and contributing to the overall integrity of the MMR process (Genschel et al., 2002; Liberti and Rasmussen, 2004). Because EXO1 plays a distinctive role in the MMR system, the EXO1 gene has gained a great interest as a potential risk factor in CRC (Jagmohan-Changur et al., 2003; Thompson et al., 2004).
To find a potential biomarker of CRC, in this study, we selected one SNP of the EXO1 gene and investigated the associations with susceptibility to CRC in a population of Iran.
Interestingly, our findings were similar to previous work by Yamamoto et al. (2005). They defined the Leu/Leu genotype to cause a reduced risk of CRC (adjusted OR = 0.398, 95% CI: 0.183-0.866) when they used a combination of the Pro/Leu and Pro/Pro genotypes as the reference. In addition, they also found that the Leu/Leu genotype had a decreased risk when the Pro/Leu genotype was the reference (adjusted OR = 0.373, 95% CI: 0.164-0.850). Despite our results, the findings did not show an increased relative risk of CRC for the Leu allele (p = 0.197).
The result contradicted our hypothesis and maybe this polymorphism might alter the capability of mismatch repair activity of exonuclease 1 protein or its interaction with other proteins working in this system. To determine the clinicopathological factors affecting the prognosis, factors of Pro/Leu +Pro/Pro and Leu/Leu subgroups were analyzed similarly to Table 2. These results show that EXO1 polymorphism might affect the behavior of CRC, but no association was observed in clinicopathological factors.
Also, on the other hand, the main reason behind this finding is related to the effect of proline via an induced kink and a reduced tendency to form the coiled coil structure in the EXO1 protein. Proline tends to destabilize alpha-helices because proline residues does not have a backbone hydrogen bond and does have steric constrains. Hence, they cannot take part in hydrogen bonding to proton acceptors such as backbone carbonyl oxygen atoms (Woolfson and Williams, 1990). Also, in several mutagenesis studies in which leucine or isoleucine residues were replaced with proline, significant disruption in the domain was not shown (Chang et al., 1999). As a consequence of this, EXO1 cannot be involved in the complex with MMR proteins to protect DNA. Thus, the polymorphism might impact on susceptibility to risk of CRC through partial repair.
In conclusion, our findings indicated that Leu/Leu genotype has a protective effect against CRC. Among different clinicopathological features, only tumor grade has a significant association with genotype (Table 3). Therefore, cancer susceptibility will be lower in people who carry a Leu/Leu genotype. On the basis of the recent findings, EXO1 polymorphism might influence in prognosis regardless of clinicopathological factors.
Footnotes
Disclosure Statement
No competing financial interests exist.