
Abstract
Amplification and/or overexpression of HER-2/neu has been reported to be associated with poor prognosis in breast cancer. One single-nucleotide polymorphism at codon 655 indicates a guanine-to-adenine substitution (Ile655Val) in the transmembrane domain-coding region of the HER-2/neu gene reported to be associated with increased risk of breast cancer. However, several studies have shown that this association is controversial. In this study, we aimed to evaluate the association between HER-2 codon 655 polymorphisms and breast cancer risk in breast cancer patients. We analyzed the HER-2 codon 655 polymorphisms in paraffin block sections from 58 breast cancer patients and 55 control subjects and evaluated the association of the polymorphic alleles with breast cancer. Following DNA isolation, polymerase chain reaction-restriction fragment length polymorphism analysis was carried out. The polymorphic Val allele was detected in 12.1% of the patients and in 17.3% of the control subjects. When the results of the study were evaluated, no statistically significant correlation was found between HER-2/neu codon 655 polymorphism and breast cancer.
Introduction
Human epidermal growth factor receptor 2 (HER-2/ERBB2/neu/c-erbB-2/EGFR2) gene is located on the chromosome region 17q12-q21; it spans 38 kb and is comprised of 27 coding exons. HER-2/neu is a proto-oncogene encoding transmembrane (TM) tyrosine kinase receptor, a 1255-amino-acid glycoprotein of 185 kDa, p185, which belongs to the HER family (Lee et al., 2008; Tao et al., 2009). There are four members in the HER family: ErbB1/HER-1, ErbB2/Neu/HER-2, ErbB3/HER-3, and ErbB4/HER-4 (Lee et al., 2008). To date, no direct ligand has been identified for HER-2/neu, but several studies suggest that HER-2/neu receptor protein acts as a coreceptor that leads to the formation of homo- or heterodimeric complexes with other family members (Harari and Yardan, 2000; Hudelist et al., 2003). HER-2/neu amplification or overexpression is seen in about 25% of breast cancer cases and has been associated with metastatic phenotype, endocrine therapy unresponsiveness, and poor prognosis (Benusiglio et al., 2005). The TM domain of HER-2/neu plays an active role in HER-2/neu dimerization and activation. A point mutation in the TM domain of the rat homolog neu (Val-6643Glu) induces protein tyrosine kinase activation and oncogenic transformation (Xie et al., 2000; Fleishman et al., 2002; Kamali-Sarvestani et al., 2004; Qu et al., 2008). Although this mutation has not been identified in humans, a common genetic variant in the nearby TM region at codon 655 was identified in the human HER-2/neu gene (Qu et al., 2008). A single-nucleotide polymorphism (SNP) in the TM coding region of the HER-2/neu gene at codon 655, encoding either isoleucine (Ile: ATC) or valine (Val: GTC), has been identified. Xie et al. (2000) first reported that this Ile/Val SNP was associated with significantly increased risk of breast cancer development. However, several studies have shown that this association is controversial (Kuraoka et al., 2003). One reason for these conflicting results might be the considerable differences in the HER-2 codon 655 genetic polymorphism between ethnic groups (Kamali-Sarvestani et al., 2004). In this study, we evaluated the association between the HER-2/neu Ile655Val polymorphism and breast cancer as well as the clinical and demographic parameters of breast cancer patients.
Materials and Methods
Patients and samples
We evaluated HER-2/neu codon Ile655Val polymorphism in paraffin-embedded tissue sections of 58 breast cancer patients with a mean age of 62.5 years (62.5 ± 13.2) and 55 control subjects with a mean age of 44.7 years (44.7 ± 14.9). Demographic and clinical characteristics of the breast cancer patients were obtained from their medical records (Table 1). Clinically, the definition of early onset is when a patient is younger than 46 years of age. To evaluate the relationship of HER-2/neu Ile655Val with the risk of breast cancer and age, the patients were divided into two groups (i.e., >46 and ≤46 years of age).
DNA extraction
Twenty-micrometer-thick sections were cut from each block and DNA extraction from paraffin-embedded tissues was performed using the Nucleospin Tissue Kit (Macheregy-Nagel) according to the manufacturer's protocol.
Polymerase chain reaction/restriction fragment length polymorphism analysis
The polymorphisms at codon 655 of HER-2/neu gene were analyzed using the polymerase chain reaction (PCR)-restriction fragment length polymorphism method. For the HER-2/neu gene polymorphism, genomic DNA was amplified in a 50 μL reaction mixture containing ∼50 ng of genomic DNA, 0.2 nM of the primers (forward: 5′-CCAGCCCTCTGACGTCCAT-3′ and reverse: 5′-TCCGTTTCCTGCAGCAGTCTCCGCA-3′), 0.4 mM of each dNTP, 1 × PCR buffer, 3 mM MgCl2, and 1 U of HotStartTaq DNA polymerase. Thermal cycling conditions for PCR were as follows: initial activation of HotStarTaq DNA polymerase at 95°C for 15 min, followed by 35 cycles at 94°C for 1 min, 58°C for 1 min, 72°C for 1 min, and a final extension of 72°C for 10 min. Amplicons (145 bp) were digested with 5 U BsmA1 (MBI Fermentas) by overnight incubation at 37°C. Restriction fragments were separated on 12% polyacrylamide gels. The gel was stained with ethidium bromide (10 mg/mL) and visualized under ultraviolet light. Restriction fragments were 119 and 26 bp for the Ile allele and 89, 30, and 26 bp for the Val allele, respectively (Fig. 1). Although the 30- and 26-bp fragments were not clearly visualized, each genotype was judged by the presence or absence of the 119- and 89-bp fragments (Fig. 1).
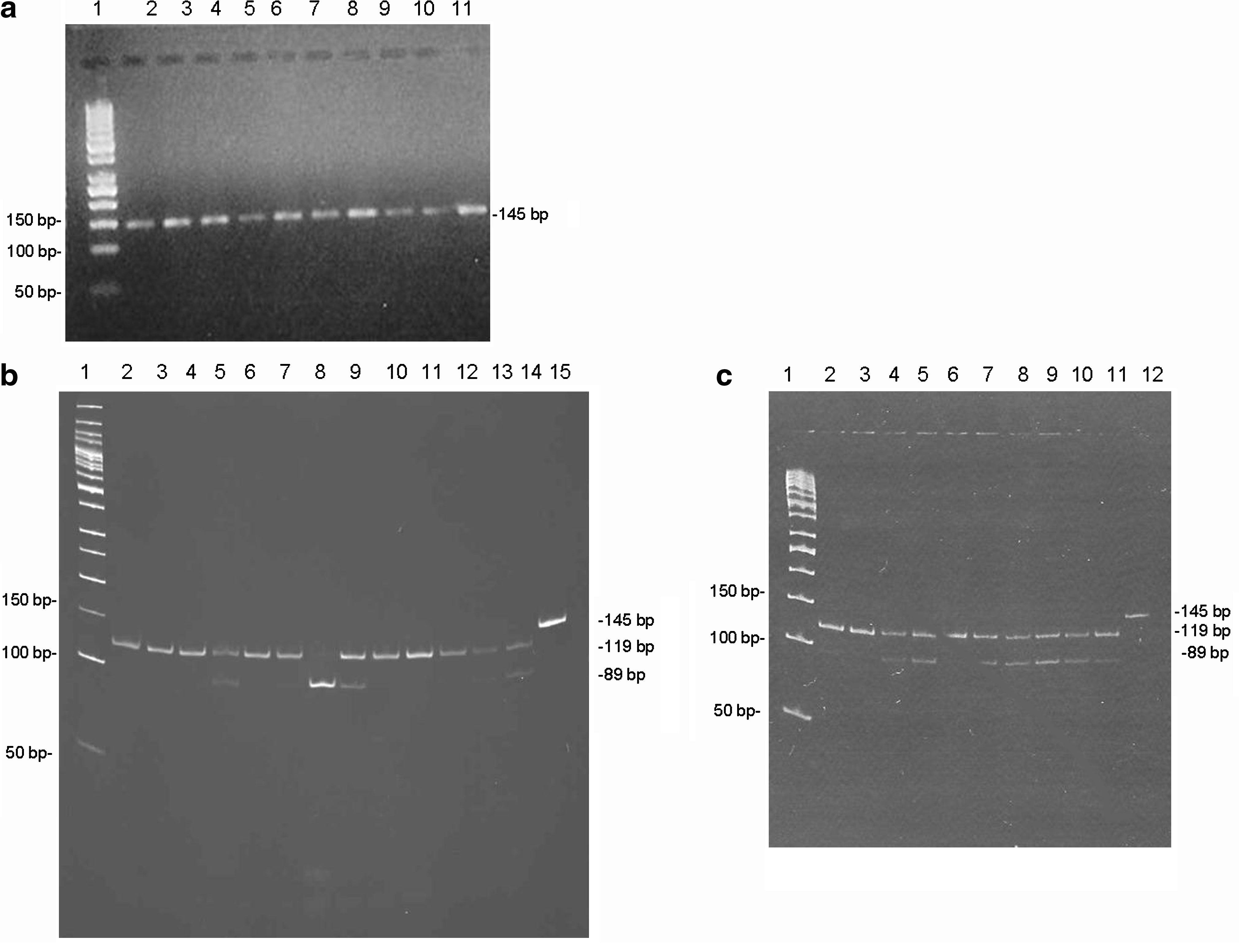
Restriction analysis of HER-2/neu codon 655 gene polymorphisms:
Statistical analysis
The data were analyzed using the Fisher's exact test. Differences at p < 0.05 were considered to be significant. Statistical analyses were performed with SPSS software, Version 11.5. Age 46 years or younger was used as the cutoff point because it has been traditionally used to define early-onset breast cancer and the patients were classified as >46 and ≤46 years of age (Goksel et al., 2004).
Results
We investigated the allele and genotype frequencies of HER-2/neu Ile655Val polymorphism in both breast cancer patients (n = 58) and normal controls (n = 55). The frequencies of HER-2/neu genotype in the breast cancer subjects and the control subjects are shown in Table 2. Among the breast cancer patients, 44 of the 58 (75.9%) women had Ile/Ile genotype and 14 (24%) had Ile/Val genotype. We did not detect Val/Val genotype in the patient group. On the other hand, among the 55 control patients, 37 (67.3%) women had Ile/Ile, 17 (30.9%) had Ile/Val, and 1 (1.81%) had Val/Val genotype. The genotype frequencies of HER-2/neu polymorphism were not significantly different between the breast cancer cases and controls (p > 0.332). The frequencies of the variant Val and wild-type Ile alleles were 12.1% versus 17.3% and 87.9% versus 82.7% in the patient and control groups, respectively. The frequencies of the variant allele were similar in the patient and control groups and the differences between the frequencies were not statistically significant (p > 0.346).
p < 0.05 was accepted as statistically significant.
Discussion
In our study, we examined whether the risk of breast cancer is associated with the Ile/Val SNP of HER-2/neu TM domain coding region at 655 and the progression of the disease. In this study, we did not observe a significant difference in the genotype distribution of the patients with breast cancer when compared with the control group. Xie and colleagues (2000) were the first to demonstrate that the Val allele was linked to an increased risk of breast cancer among women in Shanghai, China, particularly among women younger than 45 years of age. Similarly, Lee and colleagues (2008) reported a 2.24-fold increase in breast cancer risk associated with the Val allele in patients who were <45 years of age. Our results are in accordance with previous reports on German (Wang-Gohrke and Claude, 2001), Iranian (Kamali-Sarvestani et al., 2004), and Turkish (Akisik and Dalay, 2004) populations. Our null results for younger women and women with a positive family history of breast cancer do not concur with findings of Montgomery and colleagues (2003), which showed a threefold increased risk among Australian women <40 years of age. Wang-Gohrke and Claude (2001) reported a twofold increased risk among German Caucasians with a first-degree family history of breast cancer. Similarly, Millikan and colleagues (2003) reported twofold increased risk of breast cancer associated with the Val/Val and Ile/Val genotypes compared with Ile/Ile genotype among women who were both <45 years of age and reported to have a positive family history of breast cancer. We were unable to examine the HER-2/neu polymorphisms in younger women because of the small number of patients. Only five cases in our study were 46 years of age or younger. The discrepancy between our results and the results of the previous reports suggesting an association with HER-2/neu polymorphisms might be explained by population stratification bias or significant variation of the Val allele in ethnic groups (Keshava et al., 2001). Further, when our patients were stratified according to demographic and clinopathological data, such as menopausal status, family history, lymph node metastasis, distant metastasis, and local recurrence, no significant differences were observed. In conclusion, our study suggests that HER-2/neu Ile655Val gene polymorphism is not associated with the development of breast cancer and the Val allele of the HER-2/neu gene may not have the potential to be a genetic marker for tumor prognoses. It will be necessary to confirm our results on HER-2/neu polymorphism in a larger group of patients.
Footnotes
Acknowledgment
This study was supported by the Baskent University Research Fund (project number: KA08/166).
Disclosure Statement
No competing financial interests exist.