
Abstract
Conflicting results have arisen among different ethnic populations with regard to the ability of tumor necrosis factor (TNF) to control the development of bronchial asthma. We examined common TNF polymorphisms (TNFA −1031C>T, TNFA −308G>A, and TNFB +252A>G) to develop a model of the associations between these genetic markers and the development of the disease in Egypt. Amplified DNA from buccal mucosa was genotyped for 240 children using polymerase chain reaction-restriction fragment length polymorphism. Skin prick test, total serum immunoglobulin E levels, and assessment of pulmonary functions were investigated. The onset age for one-third of the asthma patients in our study was between 7 and 10 years. The TNFA −1031C>T and TNFA −308G>A polymorphisms were strongly associated with the risk of asthma (p = 0.007, and p = 0.000, respectively), but the TNFB +252A>G polymorphism was not (p = 0.6). We detected a significant linkage between the +252A>G and −1031C>T, and another between the +252A>G and the −308G>A (p < 0.0001 for both). The −1031C>T and −308G>A polymorphisms were not linked (p = 0.14). The −308A/A genotype was absent, and the −308A allele was expressed only in patients with −308G/A heterozygosity (13%). All but the +252G/A genotype were also strongly associated with the severity of disease. Environmental factors, as genetic variations, clearly influence susceptibility, the onset, progression, and severity of bronchial asthma. More information is needed to develop genetic models of susceptibility for different ethnic populations.
Introduction
B
Approximately 48%-79% of cases of asthma are inherited (Pinto et al., 2008). However, the inheritance does not follow the classical Mendelian patterns—and the mechanism for the development of asthma remains unknown—because of complex interactions between genetic and environmental factors (Bierbaum and Heinzmann, 2007; Yang et al., 2009).
Linkage studies to determine how different genetic loci might influence a person's susceptibility to asthma have frequently included five chromosomal regions: 5q31-32, 6p21, 11q12-13, 16p11-12, and 20p13 (Pinto et al., 2008). Growing evidence supports a role for tumor necrosis factor (TNF, OMIM #191160), located on 6p21, as a multifunctional cytokine T helper 1 (Th1) molecule in the pathogenesis of the disease (Kumar and Ghosh, 2009). TNF is located at 6p21.1-6p21.3, with a physical distance of about 13 kb between the genes for TNFA and TNFB (Fig. 1).
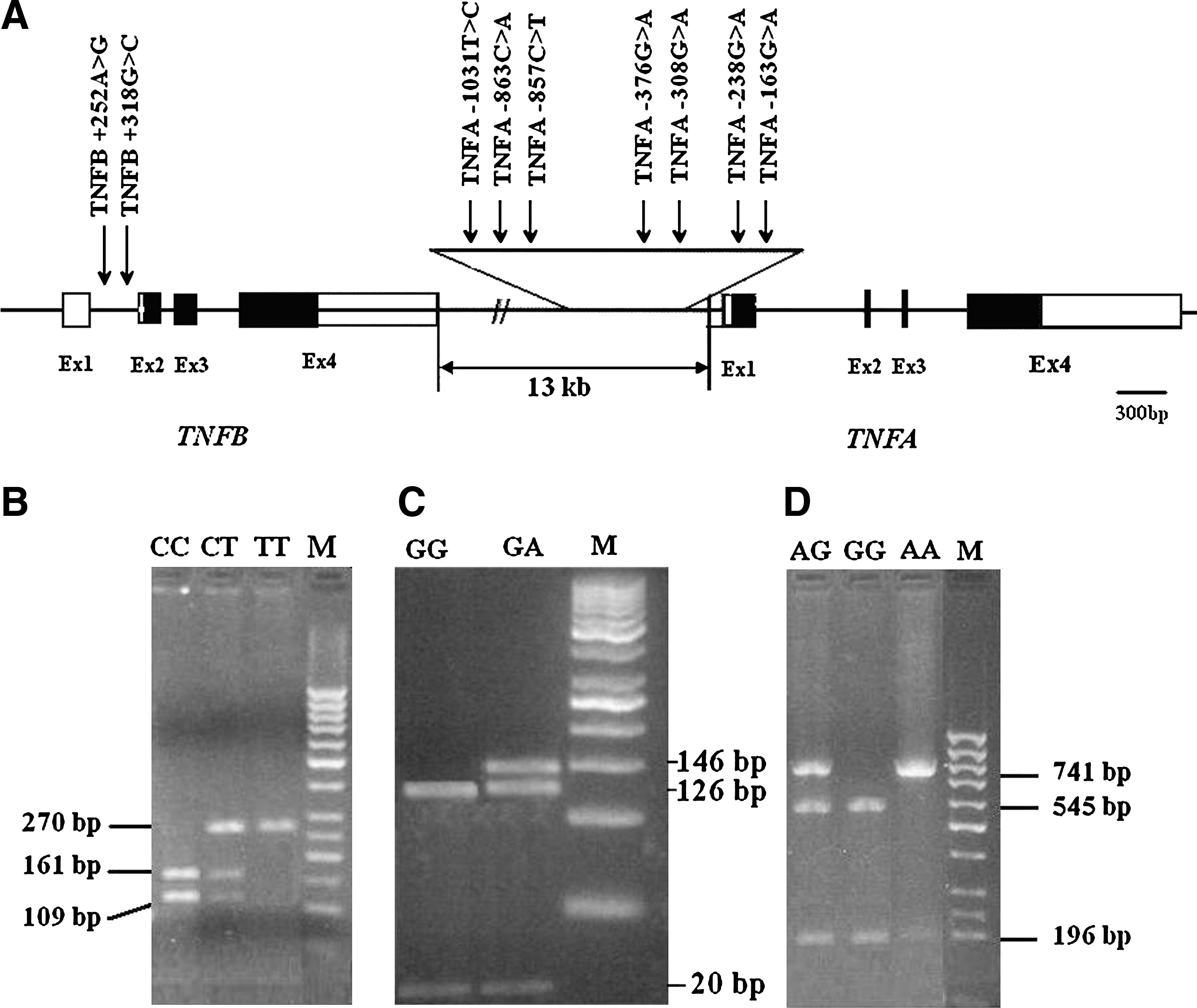
TNFα, β gene polymorphisms and gel patterns.
Several single-nucleotide polymorphisms (SNPs) in both the TNFA and TNFB genes have been shown to be associated with asthma, but results of the studies have been conflicting (Brinkman et al., 1997; Moffatt and Cookson, 1997; Shin et al., 2004; Aoki et al., 2006). Three common polymorphisms have been identified in the promoter of TNFA (−1031C>T, −863C>A, and −857C>T) (Moffatt and Cookson, 1997).
Homozygosity for a +252A>G change in the first intron of the TNFB gene has been shown to be significantly associated with increased risk for myocardial infarction in the Japanese population (Ozaki et al., 2002). This same intronic polymorphism has also been reported to be associated with asthma in Australians (Albuquerque et al., 1998), although in the Spanish not all studies have shown significant associations (Castro et al., 2000).
A recent study among 69 Egyptian patients of Lower Egypt ancestry (Nile Delta region) with asthma reported an association between the TNFA −308G>A polymorphism and susceptibility to asthma. Here we present a broader model for the Egyptian asthma cases regarding three common SNPs: TNFA −1031C>T, TNFA −308G>A, and TNFB +252A>G. We also evaluate age of onset, family history, and severity of the disease in our population.
Subjects and Methods
Study population
We administered a standard Medical Research Council questionnaire on symptoms of bronchitis, as previously described (Cotes et al., 1997), to patients attending the Ain Shams University-Pediatrics Hospital in Cairo. From this population, we recruited 120 asthmatic children, ages 1-15 years, and 120 healthy controls who were matched for age and ethnicity. All our cases and the healthy subjects were living in suburbs of Cairo. The study was approved by the ethics review committee of our institution, and we obtained written informed consent from their parents.
Each asthmatic child underwent a full clinical history, a test for total serum immunoglobulin E (IgE) levels, a skin prick test, and an assessment of bronchial hyperactivity. We recorded the forced vital capacity (FVC), peak expiratory flow (PEF), forced expiratory volume in 1 s (FEV1), and forced expiratory flow between 25% and 75% of the FVC (FEF25-75) for each child. Using the criteria of the Global Initiative for Asthma (www.ginasthma.org) (GINA, 2007), we then classified the children's asthma into four groups according to the severity of their disease and to their PEF levels: mild intermittent asthma, mild persistent asthma, moderate persistent asthma, or severe persistent asthma (Table 1).
PET parameters represented as FVC, average flow 25%-75% of FVC (FEF25-75), and forced expiratory volume at 1 s (FEV1).
Mild intermittent bronchial asthma: symptoms of bronchial asthma ≤2 time/week at day, normal PEF between attacks, and <2 times/month at night (PEF or FEV1/PEF variability, ≥80%/<20%).
Mild persistent: symptoms >2 time/week at day, >2 times/month at night, and attacks affect the activity (≥80%/20%-30%).
Moderate persistent: symptoms of asthma are daily at day and >1 time/week at night and attacks affect activity (60%-80%/>30%).
Severe persistent: symptoms are continuous at day and frequent at night with a limited physical activity (≤60%/>30%).
FVC, forced vital capacity; PEF, peak expiratory flow; PET, pulmonary function test.
Healthy subjects with no clinical asthma, negative on skin prick test and bronchial hyperactivity testing, and with normal total serum IgE levels were used in case/control genotype frequency comparisons.
Detection of the TNFA and TNFB polymorphisms
Genomic DNA was prepared in situ by gently scraping the buccal mucosa for 30 s using a cytobrush, as previously described (Shawky et al., 2004). The buccal cells were then treated directly with diluted NaOH solution, heated, and neutralized with Tris-Cl, pH 8.0. A 2.5-μL volume of these cells typically sufficed for polymerase chain reaction (PCR) amplification.
We selected the following three SNPs to analyze for our study: TNFA −1031C>T, TNFA −308G>A, and TNFB +252A>G (www.snp-genetics.com). Genotyping for the TNFA −1031C>T polymorphism was performed using a PCR fragment amplified by the forward primer 5′-GGGGAGAACAAAAGGATAAG-3′ and the reverse primer 5′-CCCCATACTCGACTTTCATA-3′ (Noguchi et al., 2002). The TNFA −308G>A polymorphism was analyzed using the forward primer 5′-GAGGCAATAGGTTTTGAGGG
For PCR amplification, DNA was added to a 15-μL reaction mixture containing 0.5 μM of each primer, 200 μM of each dNTP, 67 mM Tris-HCl, 16 mM (NH4)2SO4, 0.01% Tween-20, 1 mM MgCl2, and 0.45 U Taq DNA polymerase. All amplifications, except for the one for the −1031C>T site, contained a final concentration of 4% dimethylsulfoxide. We performed 35 rounds of PCR using annealing temperatures of 55°C, 59°C, and 58°C for the −1031C>T, −308G>A, and +252A>G polymorphisms, respectively. Incubation conditions were performed as described by the manufacturer (Fermantas, GmbH) (Fig. 1).
Data analysis
Possible associations between genotypes, or pulmonary function test parameters with clinical severity of the disease were analyzed using the Mantel-Haenszel χ2 test for linear association (SPSS 10.1 for VAX/VMS; SPSS Inc.).
Results
Population study and phenotypic data
Our study included 120 patients with asthma. The age of onset ranged from 1 to 15 years (mean = 8.3 years; standard deviation = 3.6 years). The largest percentage of cases (33.3%) had an age of onset between >7 and 10 years, and the next largest percentage (26.7%) had an age of onset between >5 and 7 years. We identified a positive family history of asthma in 72 (60%) of the cases. The rest were considered sporadic cases. The gender distribution among the patients was fairly equal, with 64 (53%) being female and 56 (47%) being male. All patients with asthma were living in the suburbs of Cairo (Fig. 2).
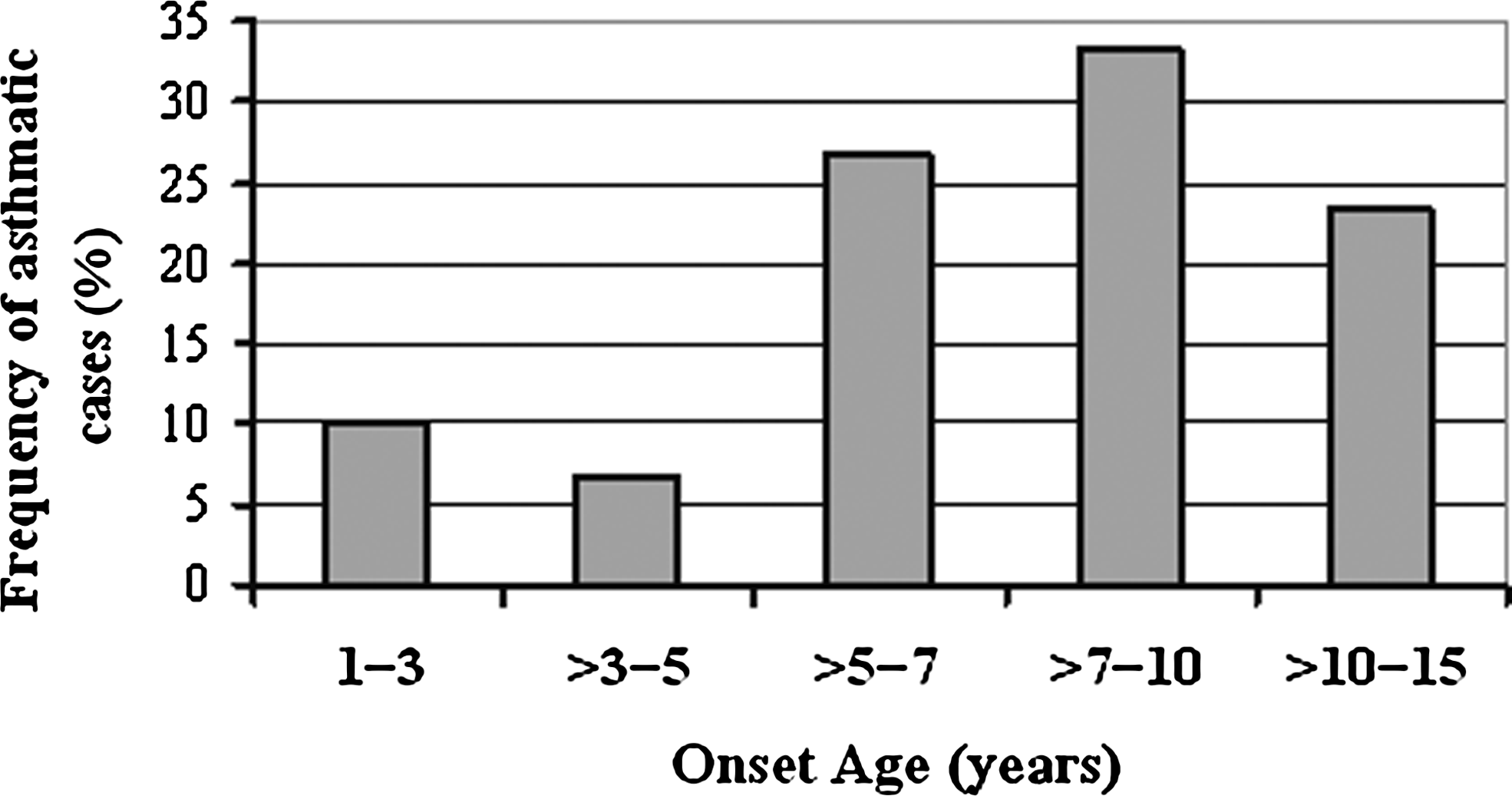
Asthmatic cases with maximal frequencies at >5-10-year-old intervals.
Ninety-five percent of asthma patients had elevated levels (>72%) of total serum IgE (unpublished data). The mean values for FVC, PEF, FEV1, and FEF25-75 decreased significantly as the severity of asthma increased. This inverse correlation was statistically significant for all four measures of pulmonary function (p < 0.05) (Table 1).
Associations between TNF polymorphisms and asthma
By comparing the genomic DNA of 120 asthma patients with that of 120 healthy controls, we evaluated possible associations between the genotypes at the TNFα −1031C>T, TNFα −308G>A, and TNFβ +252A>G loci and asthma. The genotypes at −1031C>T, and −308G>A were each strongly associated with the risk of asthma (χ2 = 9.94; p = 0.007 and χ2 = 70.2; p = 0.000, respectively). The genotype at +252A>G was not associated with asthma in our population (χ2 = 1.1, p = 0.6) (Table 2).
TNF, tumor necrosis factor.
Although the +252A>G polymorphism was not associated with asthma, it was strongly linked to the other two SNPs (χ2 = 25.9; p = 0.000002 for −1031C>T and χ2 = 24.6; p = 0.000004 for −308G>A). In contrast, the −1031C>T polymorphism was not linked to the −308A>G polymorphism (χ2 = 3.9, p = 0.13). The −1031T/T genotype was more frequent in asthma patients than in healthy controls (Table 2).
Associations between TNF alleles and asthma
For TNF −1031, we compared the frequency of the C allele (occurring in the C/T and C/C genotypes) and the frequency of the T allele (occurring in the T/T and C/T genotypes) in patients with asthma. We found that the C allele made up 16.7% of all alleles and that the T allele made up 83.3% of all alleles. The difference between these two frequencies was statistically significant (χ2 = 53.3; p < 0.00001). The −1031C allele was significantly associated with low serum TNFα concentrations. The distribution of the C- and T-alleles in this polymorphism was not significantly different in cases compared to healthy controls (p = 0.15, and p = 0.56, respectively) (Table 2).
Similarly, when we examined the −308 genotype in the patients with asthma, the percentage of G alleles was significantly higher than the percentage of A alleles (86.3% vs. 13.7%, p < 0.00001). We found no significant differences between the percentage of G alleles and the percentage of A alleles when we compared the patients with asthma to the healthy controls (p = 0.25 and p = 0.86, respectively). We also found that the −308A/A genotype was absent in our Egyptian population.
Our results were slightly different for the TNFβ +252A>G polymorphism. When we examined the DNA of our patients with asthma, we found no significant differences between the frequency of the A allele and the frequency of the G allele (60% vs. 62.5%, p = 0.24). We also found no significant differences when we compared the frequencies of these alleles between our patients with asthma and our controls (p = 0.97, and p = 0.96, respectively) (Table 2).
SNPs and severity of disease
Almost all of the genotypes in the SNPs, TNFA −1031C>T, TNFA −308G>A, and TNFB +252A>G, were strongly associated with various forms of the phenotypes (p > 0.001). The exceptions were the −1031T/T genotype, which was only moderately associated with severity of disease (p = 0.003), and the +252G/A heterozygous status, which was not significantly associated with severity (Table 3). The genotype −1031T/T was the most frequent in patients with severe asthma.
Discussion
Based on the results of our study, we now have a model of common TNF haplotypes, including TNFA −1031C>T, TNFA −308G>A, and TNFB +252A>G, in the associations between these genetic markers and the development of the disease in the Egyptian population.
In our population, most of the patients with asthma were 5-10 years old at the time of onset. The cases that occurred in 1-3 year olds may have been due to the genetic traits of the parents' immune systems. By 3-5 years, the children may have acquired their own immunity (rather than from breastmilk), demonstrated by the decline in frequency of asthma in this age group. Over time, the immune systems of the children were likely affected adversely by increasing environmental factors, accounting for the spike in asthma frequency among school-age children (ages 5-10 years). Our interpretation is similar to that from other recent studies, suggesting that the increase in prevalence over time can be attributed to early environmental exposures acting on pre-existing asthma-susceptible genotypes (Carpe et al., 2010). At ages 10-15, the body's immune response against allergens with protease activity (Pichavant et al., 2005) or other deleterious effects (Shakib et al., 2008) may reflect an ongoing evolution of human beings with their environment. Basically, exposure to microorganism during early developmental stages forces the immune response toward a Th1 type, which is protective against asthma (Carballido et al., 1992; Aebischer and Stadler, 1996); Th1/Th2 polarization has become the hallmark to explain the causes of asthma (Colavita et al., 2000) and it has dominated the field of asthma genetic research for the last two decades.
Sixty percent of our asthma patients had a family history of the disease. This frequency was similar to that from a previous study (Salam et al., 2004). Because 40% of asthma patients did not have a family history of the disease, this finding also supports the involvement of both environmental and genetic factors in the development of bronchial asthma.
In our study, 93% of the children with asthma were living in random home-blocks, which likely exposed them to higher-than-normal levels of bacteria, fungi, and protein allergens. Having a shortage of healthy green areas, homes that are too close together, or more than five family members living in humid rooms are among the factors that may have contributed (Dunstan et al., 2005).
The female/male ratio of our asthma patients was 1.4:1. This is consistent with previous studies showing that female/male ratios for immune diseases can range from 10:1 to 1:3, with similar severity between the sexes (Lockshin, 2006). Thus, men and women respond similarly to the infection and to vaccination, arguing against intrinsic sex differences in immune response. Endogenous hormones could cause sex discrepancy if their effect is a threshold off-on switch rather than quantitatively variable. X-inactivation and imprinting could cause sex discrepancy. In adults, other possibilities may include chronobiologic differences and pregnancy and menstruation biologies in which men differ from women (Lockshin, 2006).
TNFA −376G>A and TNFA −163G>A polymorphisms have been reported in patients with asthma from some studies (Brinkman et al., 1997). However, the frequency of these polymorphisms is <2% in the Egyptian population (unpublished data), so we did not examine them in our study.
The rare TNFA −1031C allele was significantly associated with low serum TNFα concentrations. Thus, we propose that the −1031C>T polymorphism affects the binding of nuclear protein(s) to the promoter of the TNFα gene and its expression. This leads to variation in serum TNFα levels, and consequently to the severity of the asthma.
The TNFA −308G>A polymorphism, with an allele frequency of 0.16 in Caucasian individuals, has been well studied for possible associations with immune-mediated diseases. Our finding of the absence of the −308A/A genotype in our Egyptian population was consistent with other reports from Belgium, Taiwan, China, Japan, and Mexico (Huang et al., 1997; Louis et al., 2000; Wang et al., 2004; Aoki et al., 2006; Jiménez-Morales et al., 2009). The highest frequency of the −308A/A genotype that has been reported is 4% (Moffatt and Cookson, 1997; Louis et al., 2000; Winchester et al., 2000; Zhu et al., 2000; Witte et al., 2002; Beghé et al., 2004; Shin et al., 2004). The frequency we reported for the heterozygous TNF −308G/A genotype (13%) was in agreement with the frequency found in previous studies of healthy Egyptians (Zedan et al., 2008) and of various other ethnic populations (Louis et al., 2000; Winchester et al., 2000; Zhu et al., 2000; Witte et al., 2002; Beghé et al., 2004). The −308A allele has been correlated with an increase in transcription activity and secretion levels of this cytokine (Wilson et al., 1997; Jeong et al., 2004; Glossop et al., 2005). However, in Italian, Belgian, Japanese, and Korean populations, the −308A allele has been reported either to be protective or to not be associated with asthma (Louis et al., 2000; Padyukov et al., 2001; Shin et al., 2004).
In our study, the TNFB +252A>G polymorphism was not associated with asthma. However, we cannot exclude the possibility that it might still make a minor contribution to susceptibility, perhaps by influencing the expression of TNFβ in coordination with other mutations in TNFα or β. The +252G allele has been associated with a lower TNFβ response and the +252A allele with a higher response (Messer et al., 1991). It is possible that intron 1 of the TNFβ gene, which contains the NcoI polymorphism, includes a regulatory element that affects TNFA gene expression (Albuquerque et al., 1998). The failure of another study to find an association between this polymorphism and asthma (Noguchi et al., 2002) was not due to sample size.
Several genes, including ADAM33 (20p13; OMIM #607114), DPP10 (2q12.3-q14.2; OMIM #608209), PHF11 (13q4.1; OMIM #607796), GPRA (7p15-p14; OMIM #608595), TIM-1, PDE4D (5q12; OMIM #600129), OPN3 (1q43; OMIM #606695), and ORMDL3 (17q21.1; OMIM #610075), have been implicated in the susceptibility to and pathogenesis of atopy and asthma (Pinto et al., 2008; Hancock et al., 2009; Agrawal and Shao, 2010), and can probably used in our Egyptian model. Genome-wide association studies are also being used to identify novel gene variants that are associated with disease. Results of the first three genome-wide association studies on asthma have identified ORMDL3, IL1RL1, and PDE4D as susceptibility genes (Boezen, 2009).
During the past decade, the major goal of immunotherapy for asthma has been to direct the immune response to a type 1 response, or immune tolerance (Agrawal and Shao, 2010). In Egypt, monotherapy with inhaled corticosteroid is the most common therapy for all levels of asthma severity. This condition was not so odd in various ethnic populations irrespective of the physician classification of asthma severity, as leukotriene receptor antagonists were rarely used and high-dose inhaled corticosteroid or add-on long-acting beta2-agonist was prescribed even in intermittent and mild disease (Thomas et al., 2010). However, our results imply that treatment strategies directed against TNF may also be effective in managing asthma.
Despite the fact that environmental factors clearly influence the onset, progression, and severity of this disease, family studies indicate that genetic variation also influences susceptibility. Egypt has been the interest of many conquerors since the times of the ancient Pharaohs till the Arab-Isreali conflict, including the Osmani Empire, the French campaign, and British domination. As a consequence, much social intermarriage between those populations and the Egyptian community toughened the heterogeneity, the pleiotropy, and variable expressivity of the allergic airway disease.
Conclusion
To our knowledge, our study is the first to describe an Egyptian model of the relationships of the three common polymorphisms—TNFA −1031C>T, TNFA −308G>A, and TNFB +252A>G—with bronchial asthma. Our findings support previously reported associations between the TNFA, B genes and asthma or asthma-related phenotypes in other ethnic populations. The significance of genetic variants in the TNF loci with respect to asthma susceptibility is complicated because these loci are in linkage disequilibrium with some major histocompatibility complex (MHC) alleles. These observations sustain the need for replication of studies of susceptible genes among all ethnic groups, especially those with a high degree of heterogeneity, such as the Egyptian community.
Footnotes
Acknowledgments
We wish to thank the staff of Hospitals of Ain Shams University-Cairo, for providing the clinical records and samples. We also thank the families of the asthma patients for their willingness to collaborate with us in this research.
Disclosure Statement
The authors declare that no competing financial interests exist.