
Abstract
Introduction: Microdeletions in the azoospermia factor region on the long arm of Y chromosome are associated with spermatogenic failure. There are many markers for the diagnosis of Y chromosome microdeletion analysis, but in routine practice only a limited set of markers can be tested. Objective: The objectives of this study were to determine the frequency of Y chromosome microdeletion in idiopathic cases of male infertility in India, to attempt genotype-phenotype correlation, and to evaluate whether markers to be tested for diagnosis of Y chromosome microdeletion should be ethnicity specific. Methods: Microdeletions in the Y chromosome were analyzed in 200 infertile males. The six sequence tag site (STS) markers prescribed by the European Academy of Andrology (EAA) were used initially. Patients in whom no deletions were detected by use of these markers were tested by markers selected from other studies from India. Results: The STS markers prescribed by EAA detected deletions in only 6 (3%) of 200 infertile males. However, markers selected from previous Indian studies showed deletions in an additional 15 (7.5%) of infertile males. Overall, Y chromosome microdeletions were observed in 21 (10.5%) of 200 patients. Of these, 13 were cases of azoospermia and 8 were cases of severe oligospermia. Conclusion: The markers prescribed by EAA alone are not suitable for the diagnosis of Y chromosome microdeletions in infertile males. The protocol for identification of Y chromosome microdeletions in cases of nonobstructive azoospermia/severe oligospermia would have to include a different set of STS markers.
Introduction
I
The total number of markers that have been shown to be deleted in various studies is more than 80 (Najmabadi et al., 1996; Vogt et al., 1996; Foresta et al., 1997; Pryor et al., 1997; Selva et al., 1997; Van et al., 1997; Foresta et al., 1998; Foresta et al., 1999; Simoni et al., 1999; Martinez et al., 2000; Tse et al., 2000; Krausz et al., 2001; Babu et al., 2002; Peterlin et al., 2002; Ambasudhan et al., 2003; Dada et al., 2003; Pedro et al., 2003; Swarna et al., 2003; Thangaraj et al., 2003; Rao et al., 2004; Kumar et al., 2006; Vutyavanich et al., 2006; Mitra et al., 2008). However, in practice, only a limited number of markers can be analyzed. The European Academy of Andrology (EAA) recommended six sequence tag site (STS) markers for detecting Y chromosome microdeletions, which enabled the detection of over 90% of the deletions in the AZF loci (Simoni et al., 1999). We aimed to study the frequency of Y chromosome microdeletion in idiopathic cases of male infertility and to evaluate the utility of EAA recommended STS markers to detect the Y chromosome microdeletions in Indian infertile males. To improve the yield and develop a cost-effective protocol, we also analyzed other markers that have been documented to be deleted among Indian patients (Babu et al., 2002; Ambasudhan et al., 2003; Dada et al., 2003; Swarna et al., 2003; Thangaraj et al., 2003; Rao et al., 2004; Kumar et al., 2006; Mitra et al., 2008). We compared the data with published results from other countries to examine the issue whether the markers to be selected for analysis should be ethnicity specific. We also attempted to establish a correlation between the genotype and phenotype in the infertile males.
Materials
Two hundred infertile males were enrolled in the study who visited the In Vitro Fertilization Unit at the Centre for Human Reproduction, Sir Ganga Ram Hospital, New Delhi, from January 2007 through December 2009. The age range of the patients was 28-36 years and the mean age of the patients was 32.7 years. Of the 200 cases, 150 were azoospermic males and 50 were severely oligospermic males. Individuals were defined as azoospermic when there was complete absence of sperms and as severely oligospermic when sperm count was less than 5 × 106, as per the criteria of the World Health Organization (1999) manual. A written informed consent was obtained from each individual. They were subjected to clinical examination, and laboratory investigations including semen analysis, endocrinological studies, and when available, results of aspiration of sperms from the testis were also documented.
Methods
Peripheral blood samples were collected in EDTA vials from all the 200 subjects and DNA was isolated using salt precipitation method (Miller et al., 1988). The STS markers initially used for analysis were those prescribed by the European Academy of Andrology—AZFa sY84, sY86; AZFb sY127, sY134; and AZFc sY254, sY255 (Simoni et al., 1999). In patients who did not show any deletion, additional STS markers were tested (AZFa sY742, 746, 87; AZFb sY113, 117, 120, 125, 129, 130, 131, 132; AZFc sY146, 148, 149, 153, 156, 158, 243, 269). These have been reported to be deleted among Indian infertile males (Babu et al., 2002; Ambasudhan et al., 2003; Dada et al., 2003; Swarna et al., 2003; Thangaraj et al., 2003; Rao et al., 2004; Kumar et al., 2006; Mitra et al., 2008).
The PCR mixture included 50-250 ng of DNA sample, 1 × PCR buffer, 1.5 μM MgCl2, 200 μM deoxynucleotidetriphosphates (dNTPs), 50 pmol of each primer pair, and 1 U Taq DNA polymerase. Thermal cycling conditions included initial denaturation for 5 min at 95°C followed by 35 cycles at 95°C for 1 min, 55°C for 1 min, and 72°C for 1 min 30 s, with a final extension for 5 min at 72°C. Primer sequences of STS markers used for characterization of deletion breakpoints were selected from previous studies (Babu et al., 2002; Ambasudhan et al., 2003; Dada et al., 2003; Swarna et al., 2003; Thangaraj et al., 2003; Rao et al., 2004; Kumar et al., 2006; Mitra et al., 2008). Serum follicle-stimulating hormone FSH, LH, and total testosterone levels were assayed by ELISA technique. The control group consisted of 100 males who had fathered children.
If the deletion of a marker was detected, the PCR amplification was repeated thrice to rule out failure of reaction. Absence of amplification in three reactions was considered to confirm deletion of the STS marker. With each run, samples of genomic DNA from a female and a normal fertile male (control group) were also tested. The PCR products were then analyzed in 2% agarose gel containing ethidium bromide and visualized under UV light.
Results
Using STS markers recommended by the EAA, only six (3%) of 200 infertile males were detected to carry microdeletions and they were all azoospermic. Using additional STS markers selected from Indian studies, deletions were detected in another 15 cases (7.5%) (Fig. 1). These 15 cases included seven azoospermic and eight oligospermic cases. Altogether Y chromosome microdeletions were observed in 21 cases (10.5%).
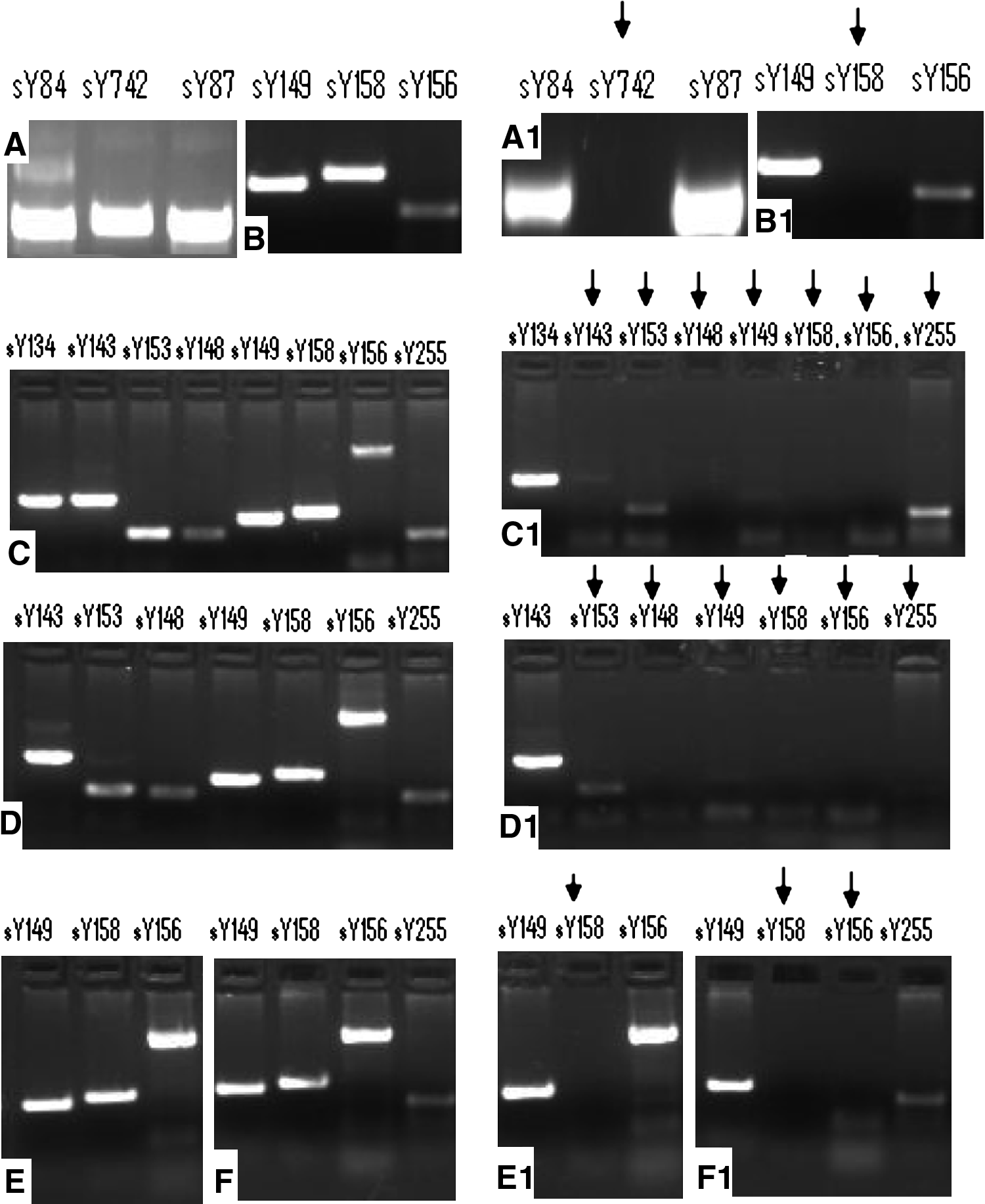
Results of PCR amplification of sets of sequence-tagged sites in Y-chromosome DNA from a normal man
In all the 21 cases found to carry microdeletions, the span of deleted regions included the AZFc region. Deletions restricted only to the AZFc region were detected in 10 cases (47.6%); of these, 8 were severely oligospermic (sperm count between 1 and 4 million) and 2 were azoospermic (1-2 motile sperm high per field through TESA). Deletions of the AZFc region combined with AZFb region were detected in nine infertile males (42.8%), of which seven were azoospermic males (sperm count 1-2 motile sperm high per field on TESA) and two were having Sertoli cell only syndrome (SCOS). Deletions of AZFc combined with AZFa region were observed in two azoospermic males with SCOS (9.5%). The deletions observed in these two cases had a normal intervening region between the two markers (Fig. 2).

Y chromosome deletion map of azoospermic/severe oligospermic men generated by STS markers. Black solid line shows the region with no deletion. Thin black line shows deletion and extents of deletion. SCOS, Sertoli cell only syndrome; TESA, testicular sperm aspiration; STS, sequence tag site.
None of the control men showed deletions of the 27 STS markers spanning the entire AZFa, AZFb, and AZFc regions.
Among 150 azoospermic males, interstitial deletions of Yq11 were recorded in 13 (8.6%) patients; in 50 severely oligospermic males, deletions were observed in 8 (16%) patients (p-value <0.05). FSH level in patients with deletions was found to be mildly elevated (of 11 ± 2.7 mIU/mL) when compared with subjects with no deletions (6 ± 1.5 mIU/mL) (Table 1). All the patients had normal serum hormone levels (LH, prolactin, and total testosterone).
Mean ± SD: FSH = 11 ± 2.7; LH = 3.5 ± 0.6; prolactin = 5.1 ± 2.1; testosterone = 29 ± 6.9; free testosterone = 4.6 ± 0.7.
AZF, azoospermia factor.
Discussion
Deletions in the Y chromosome have emerged as an important cause of male infertility. In most studies, the frequency of Y chromosome deletions increases with the severity of spermatogenic defect (Foresta et al., 1997; Pryor et al., 1997; Seva et al., 1997; Van et al., 1997). Generally, about 15% of azoospermic males and 5%-10% of oligospermic males show deletions in Y chromosome (Foresta et al., 1999). However, in the present study, the frequency of Y chromosome microdeletions was high in oligospermic males when compared with azoospermic males (8.6% vs. 16%, respectively; p-value <0.05). It is likely that the oligospermic cases in our study belonged to the very severe group and were close to the azoospermic group.
The frequency of Y chromosome microdeletions has been reported from a number of developed countries such as the United States, Germany, France, Paris, Japan, Denmark, Spain, Taiwan, Slovenia, Finland, and Hong Kong as well as from some developing countries such as India, Brazil, Iran, Egypt, and Thailand (Najmabadi et al., 1996; Vogt et al., 1996; Pryor et al., 1997; Lin et al., 2000; Tse et al., 2000; Krausz et al., 2001; Bor et al., 2002; Aho et al., 2003; Ambasudhan et al., 2003; Pedro et al., 2003; Swarna et al., 2003; Thangaraj et al., 2003; Rao et al., 2004; Kihaile et al., 2005; Omrani et al., 2006; Vutyavanich et al., 2006; Viswambharan et al., 2007; Abol et al., 2009; Sheikh et al., 2009). These data are summarized in Table 2. The reported frequency of deletions has a wide variability (0.9%-55.5%) (Van et al., 1997; Foresta et al., 1998; Foresta et al., 1999; Rao et al., 2004). It is likely that the difference of frequency of Y chromosome microdeletions is related to sample size, differences in inclusion criteria for enrolling subjects into the study, and the number of markers tested. For example, in a study conducted by Foresta et al. (1998), 18 azoospermic males with Sertoli cell only syndrome, a highly specific group, was screened for Y chromosome microdeletion and deletions found in 55.5% of the cases. In their subsequent study of 130 infertile males, who were azoospermic/severely oligospermic (110) and moderately oligospermic (20), Y chromosome microdeletions were present in 28 cases (25.4%), but no deletions were found in moderately oligospermics males (Foresta et al., 1999). The former study had a homogenous group of patients, and maybe the frequency of Y chromosome microdeletion is higher in such cases. In contrast, in the latter study, despite a larger sample size, the patients included belong to different groups—azoospermia, severe oligospermia, and moderate oligospermia. Therefore, increasing the sample size with lack of homogeneity in enrolled patients may result in reduced frequency of microdeletions. This has also been reiterated by two other independent studies conducted by Rao and his associates in India and Van and his group in Germany (Van et al., 1997; Rao et al., 2004). In the study conducted by Rao and his associates, they enrolled 251 infertile males, which included 104 azoospermia, 41 severely oligospermia, 49 mild oligospermia, and 57 oligoasthenoteratozoospermics, and found a very low frequency of microdeletions. Van et al. (1997) in a group of 171 infertile males (13 azoospermia, 79 severely oligospermia, 52 mild oligospermia, 27 moderately oligospermia) detected microdeletions in only 0.9%. The low frequency of deletions in both these studies may be due to inclusion of large number of mild as well as moderate oligospermic males. The higher the number of patients with azoospermia, Sertoli cell only syndrome, or severe oligospermia, the better are the chances of detecting Y chromosome microdeletions; in contrast, if the patients have sperm count more than 8 millions/mL, the chance of having Y chromosome microdeletions decreases markedly.
Azoo, azoospermics; oligo, oligospermics; OAT, oligoasthenoteratozoospermics; NA, not applicable; EAA, European Academy of Andrology; STS, sequence tag site.
In the present study, the most commonly deleted region of Y chromosome is the AZFc region. Indeed, all the 21 infertile males showed deletions in this region. Previous studies also demonstrated a high frequency of deletions of the AZFc region (88.8%), when compared with AZFa and AZFb regions (Martinez et al., 2000; Peterlin et al., 2002). This may be due to the presence of many repetitive sequences in this region (Kawaguchi et al., 2001). The AZFc region alone was involved in 47.6% of individuals with deletions. A varying frequency of deletion of AZFc alone (44.4%, 27.5%, and 38.4%) has been reported in infertile men in different studies (Foresta et al., 1999; Martinez et al., 2000; Thangaraj et al., 2003).
We did not observe deletions of AZFb region alone in any of the infertile men analyzed. However, such deletions have been reported with a frequency of 11.1%, 14.1%, and 21.1% (Foresta et al., 1999; Martinez et al., 2000; Kumar et al., 2006). Deletions of AZFb combined with deletions of AZFc were observed in 42.6% of the cases in the present study. Such combined deletions were also observed in other studies with a frequency of 44.4%, 44.8%, 33.3%, and 25% (Martinez et al., 2000; Pedro et al., 2003; Thangaraj et al., 2003; Mitra et al., 2008).
The frequencies of deletions in the AZFa region are, in general, less when compared with AZFb and AZFc regions (Peterlin et al., 2002). This may be due to the small size of AZFa (800 kb) region when compared with AZFb (3.2 Mb) region and AZFc (3.5 Mb) region. In our study, two patients showed deletions in the AZFa region and both of them had Sertoli cell only syndrome. In these cases, deletion involved the AZFa region and the AZFc region but with a normal intervening sequence. Similar findings have also been reported by two other independent studies (Kamp et al., 2001; Thangaraj et al., 2003). It is interesting that none of the azoospermic men studied showed the deletion of sY84 and/or sY86. Surprisingly, these two markers have been recommended by the EAA for the detection of microdeletion in the AZFa region (Simoni et al., 1999).
We attempted to make genotype-phenotype correlations by comparing the size of deletion in the Y chromosome and the sperm count. It was observed that if the deletion was very large and covered entire AZFb and AZFc regions (sY113, 117, 120, 125, 127, 129, 130, 131, 132, 133, sY134, 143 of AZFb and sY153, 148, 149, 156, 254, 255, 158, 160 of AZFc), it was associated with the phenotype Sertoli cell only syndrome (SCOS). When AZFb and beyond were missing, there was predictably no detectable completion of spermatogenesis. Therefore, deletion of functional members of the RBM gene families or other genes found in AZFb region (EIF1AY, PRY, TTY2) and DAZ gene family in AZFc region might contribute to the enhanced severity of spermatogenetic defect observed in patients whose deletions are very large and cover the entire AZFb and AZFc regions (Chai et al., 1997). If deletions involved a small part of the AZFb region (sY143) and the AZFc region (sY153, 148, 149, 156, 158, 254, 255, and 160), it was associated with 1-2 motile sperm high per field on TESA (Table 1; Fig. 2). If the deletion involves only the AZFc region (sY156, 158, 148, 149, and 153), a sperm count between 1 and 4 million was observed (Table 1; Fig. 2). The absence of these markers indicates deletion of the AZFc region, which removes all copies of the members of the DAZ gene family. The DAZ gene family is the most important candidate gene for male infertility in the AZFc region and consists of four functional copies including DAZ1, DAZ2, DAZ3, and DAZ4 arranged in two clusters. Deletions in DAZ genes may have different effects: partial or complete deletions in the AZFc region may result in different phenotypes varying from oligozoospermia to azoospermia, so there may be a chance for retrieving sperm from testis and TESE/ICSI can be attempted in these patients (Mirzajani et al., 2010).
In all 21 infertile males with deletions of Y chromosome, FSH levels were found to be mildly elevated (11 ± 2.7 mIU/mL when compared with subjects with no deletions, 6 ± 1.5 mIU/mL) (Table 1). However, the value of FSH was not as high as that observed in patients with testicular failure.
The STS markers prescribed by the European Academy of Andrology claim to detect over 90% of the microdeletions in the AZF loci (Simoni et al., 1999). However, in the present study, only 3% of subjects with deletions were identified using the STS markers recommended by EAA. Using STS markers selected from Indian studies, microdeletions were observed in another 7.5% of the infertile cases. A study conducted in the Egyptian population also reports a lower frequency of detection of Y chromosome microdeletion, wherein 100 infertile men were screened and deletion was found only in 4 cases (4%) (Sheikh et al., 2009). Another independent study was carried out in the same population who reported absence of microdeletions in their study (40 cases) and compared their finding with other published reports (Abobakr et al., 2009). The authors explain why they failed to identify any Y chromosome microdeletion, which could be due to the fewer number of STS markers, heterogeneity of markers used among different studies, and also ethnic variations (Abobakr et al., 2009).
Only four of six STS makers (sY127, sY134, sY255, sY254) recommended by the EAA showed a deletion frequency of 2.8%-4%. Of 16 markers that were used in Indian studies and not included in the EAA, six STS markers (sY113, sY143, sY148, sY153, sY156, sY158) showed deletion with a frequency range of 2.6%-6.8% (Table 3). Thus, it is clear that the use of markers recommended by the EAA alone are not enough to screen the deletions in Y chromosome in Indian subjects and additional markers should be used. We suggest that each country should examine Y chromosome microdeletions in a large number of sample with homogenous phenotypes and using large number of STS makers, which will eventually identify markers specific for their population to increase the detection of Y chromosome microdeletions.
STS markers are EAA recommended.
Footnotes
Acknowledgments
The authors thank Drs. M. Kochar, S. Mittal, K.K. Ghautam, and G. Majumdar, who referred the patients, and Dr. S. Kohli for technical advice. K. Singh, J. Singh, and D. Gupta are thanked for valuable technical assistance.
Disclosure Statement
No competing financial interests exist.