
Abstract
Background: Epigenetic alterations in the global DNA methylation status may be associated with an increased risk of some cancer types in humans. The methylenetetrahydrofolate reductase (MTHFR) gene is involved in folic acid metabolism and plays an essential role in inherited DNA methylation profiles. The common 677 C>T and 1298 A>C polymorphisms in the MTHFR gene cause the production of a thermolabile enzyme with reduced function and, eventually, genomic DNA hypomethylation. The current preliminary study was designed to determine the association between germ-line polymorphism in the MTHFR gene and differentiated thyroid carcinoma (DTC). Methods: In the current case-control study of 60 thyroid carcinomas (TC); 45 papillary TC, 9 follicular TC, and 6 DTC of an uncertain malignant potential were examined. Genomic DNA was extracted from peripheral blood with EDTA, genotyped by a multiplex real-time polymerase chain reaction. Results: An elevated 2.33-fold risk was observed for DTC in individuals with the 677TT genotype when compared with the control group (odds ratio [OR]: 1.92, 95% confidence interval [CI]: 1.03-3.58). Current DTC patients showed similar results as a control group for the 1298 A>C allele. No significant risk was detected for the homozygous 1298CC genotype (CC vs. AA or AC) (OR: 1.30, 95% CI: 0.73-2.29). Conclusion: The current results are supportive of the hypothesis that the homozygous MTHFR 677TT genotype increases the risk factor of developing thyroid cancer, and further large-scale studies are needed to validate this association.
Introduction
T
In the current case-control study, we aimed at finding a possible role of the germ-line functional gene MTHFR polymorphism in susceptibility to DTC.
Materials and Methods
Patients and clinical diagnosis
Blood samples with EDTA from 60 thyroid cancer patients who had undergone total thyroidectomy and 50 healthy control individuals were used in the current study. In a total of 60 thyroid cancer patients, there were 45 papillary thyroid carcinoma (PTC) (75%), 9 folicullar thyroid carcinoma (FTC) (15%), 6 DTC (10% (11 men (18.3%))), and 49 women (81.7%) with a mean age-min-max; 55.25±3.22 (28-75); 50 healthy adult individuals used as the control group; [21 men (42%), 29 women (58%), and mean age-min-max; 86.60±2.82 (65-77)] were included in the current results. Both groups were genotyped for MTHFR SNPs (C677T and A1298C) and compared. Individuals with any familial cancer history were excluded from the control group.
Mutation analysis
Peripheral blood samples containing EDTA from the patients and the control group were used for genomic DNA isolation. Total genomic DNA was extracted from each peripheral blood sample by the Magna Pure Compact (Roche) and Invitek kit extraction techniques (Invitek®; Invisorb spin blood). Two polymorphic regions of the MTHFR gene (C677T and A1298C) were amplified by a real-time polymerase chain reaction (PCR), LightCycler 2.0 methods (Roche). Briefly, LightCycler FastStart DNA Master HybProbes, master mix (water, PCR-grade, MgCl2, stock solution, Primer mix, and HybProbe mix), and DNA template were used for real-time amplification. The multiple PCR consisted of a denaturation step of 10 min at 95°C; followed by 40 cycles of 5 s at 95°C, 10 s at 55°C, and 15 s at 72°C; and a melting step of 20 s at 95°C, 20 s at 40°C, a continuous mode at 85°C, a cooling step of 30 s at 40°C for MTHFR C677T (rs1801133), and a denaturation step of 10 min at 95°C; followed by 40 cycles of 5 s at 95°C, 10 s at 62°C, and 6 s at 72°C; and a melting step of 30 s at 72°C, 20 s at 95°C, 1 s at 40°C, 30 s at 40°C, and 1 s at 85°C; and cooling step of 30 s at 40°C for MTHFR A1298C (rs1801131). A software program (LightCycler 2.0, Roche) was used for the detection of the mutated and normal genotype profiles of target genes in the current DTC patient and the control groups.
Statistical analysis
The estimate risk was examined by multivariate logistic regression analysis. Mutational variables were analyzed by using Fisher's exact test. Results were given as the mean (standard deviation [SD]). The software SPSS for Windows version 12.0 was used to perform statistical analysis. The Mann-Whitney U and χ2 and chi-square tests were used to analyze the differences between the patients and controls. Odds ratio (OR) and p-values for T- and C-allele frequencies were used to estimate the risk for the MTHFR gene SNPs in current patients with DTC.
Results
The current preliminary case-control study was designed to determine the association between germ-line point mutations in the MTHFR gene and DTC. By the multiplex real-time PCR technique, we evaluated two common SNPs of the MTHFR gene in DTC patients, and the results were compared with the healthy control group (Fig. 1). The estimate risk was examined by multivariate logistic regression analysis. Statistically, the TT homozygous genotype in the 677 C>T SNP was associated with a 2.33-fold significance in the increase of the risk for DTC patients.
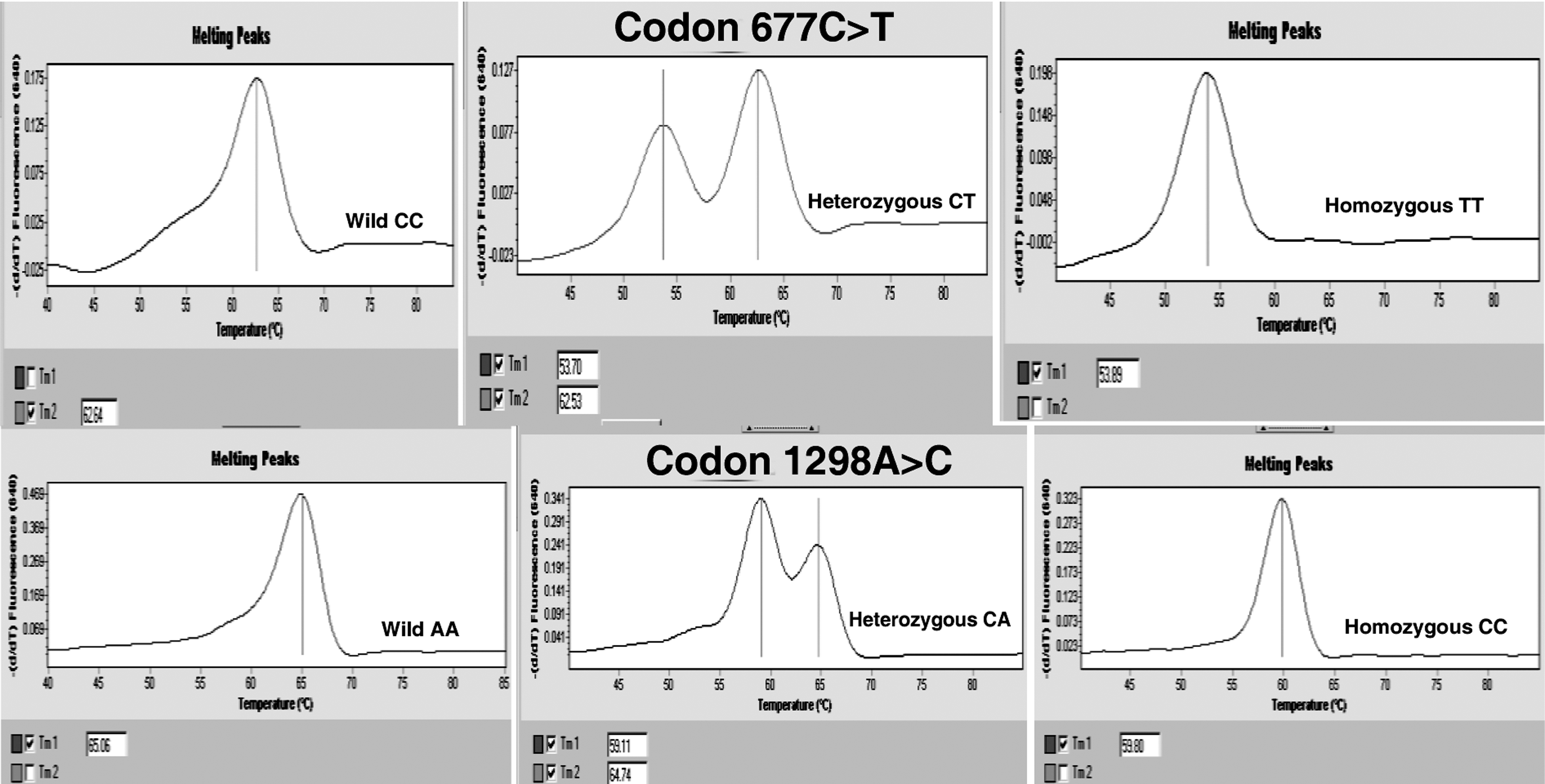
This figure shows real-time—polymerase chain reaction profiles of wild and mutated genotypes for MTHFR 677 C>T and 1298 A>C single-nucleotide polymorphisms in the current differentiated thyroid carcinoma patients.
Clinicopathologic data and follow-up knowledge
A total of 60 DTC patients [49F (81.7%) and 11M (18.3%)]; 45 PTC (75%), 9 FTC (15%) and 6 uncertain malignant potential (10%), mean age 55.25±13.22 (28-75), were clinically diagnosed and treated. Peripheral blood-EDTA samples from healthy controls and DTC patients were examined for genotyping in the current study. The subtypes and some clinical characteristics, such as mean age, sex distribution, smoke status, and familial cancer history of patients and control groups, are provided in Table 1. Both smoking status and familial cancer history showed statistical significance in the studied DTC group when compared with the control group (p<0.01). Sixteen of the (26.6%) current DTC patients were heavy smokers (package per a day). This situation was significant (OR: 1.289, 95% confidence interval [CI]: 0.530-3.187) when compared with the control group (Table 1). Twenty-two of the (36.6%) DTC patients reported a familial cancer history. This situation was also statistically significant (OR: 1.648, 95% CI: 0.724-3.747) when compared with the control group (Table 1). The genotype analysis and statistical results for both MTHFR 677 C>T and 1298 A>C SNPs were demonstrated in Tables 2 and 3. The studied DTC patients showed 28 (46.6) CC, 25 (41.7%) CT and 7 (11.7%) TT genotypes for 677 C>T SNP. The C-allele frequency was 0.675, and the T-allele frequency was 0.325 for 677 C>T SNP in the DTC patients (Table 2). An elevated 2.33-fold risk was observed for DTC in individuals with the 677TT genotype (OR: 1.92, 95% CI: 1.03-3.58), (p=0.01).
Chi-square test is significant, p>0.01.
PTC, papillary thyroid carcinoma; FTC, folicullar thyroid carcinoma; DTC (UMP), Well-differentiated thyroid carcinoma of uncertain malignant potential; OR, odds ratio; CI, confidence interval.
Chi-Square test is significant, p>0.01.
SNP, single-nucleotide polymorphism.
The studied DTC patients also showed 22 (36.6) AA, 33 (55.0%) AC, and 5 (8.4%) CC genotypes for a second SNP, 1298 A>C in the MTHFR gene (Table 3). The A-allele frequency was 0.700, and the T-allele frequency was 0.300 for SNP in the patients group. The difference in genotype frequency distribution between the DTC cases and controls was not significant for this SNP (p=0.18), (Tables 1 and 3). Multivariate analysis demonstrated an increased risk of DTC for the 677 C>T homozygous genotype TT for the results presented. Despite some limitations, the results indicated that the individuals with the 677TT genotype had an 11.7% higher risk of having DTC. No evidence of such an association was observed in the DTC patients with the A>C polymorphism at codon 1298 in the current results.
Discussion
Thyroid cancers of a follicular cell origin account for the majority (95%) of all thyroid cancers and represent the most common type of endocrine neoplasia. DTC is the most common malignancy of the thyroid gland and involves some molecular ethiological parameters, such as point mutations in the proto-oncogenes of BRAF V600E, KRAS, RET, functional genes of MTHFR, MDR1, and epigenetic alterations of several tumor suppressor gene abnormalities (Schulz and Hoffmann 2009; Fard-Esfahani et al., 2011; Moura et al., 2011; Vineis et al., 2011). The genetic parameters may contribute to the individual differences in the epigenetic regulation of cancer susceptibility, drug efficacy, and cytotoxicity. The functional MTHFR gene catalyzes the conversion of 5,10-methylenetetrahydrofolate (5,10-methylene-THF) to 5-methyl-tetrahydrofolate (5-methyl THF) and plays a crucial role in folate metabolism and systemic methyl sources. Therefore, a decrease in 5-methyl THF in the MTHFR dysfunction and/or hypofunction leads to a decrease of the available SAM, which results in DNA hypomethylation and may play a critical role in carcinogenesis (Goyette et al., 1998; Weisberg et al., 1998; Liu et al., 2011; Tsai et al., 2011; Zacho et al., 2011). Reduced enzyme activity (∼50-60%) was reported by Dong et al. for the individuals with heterozygous profiles for both the 677 C>T and 1298 A>C alleles (Dong et al., 2010). Curtin et al. suggest that folate supplementation may affect the initiation and progression of methylated rectal tumors in men in the presence of a variable MTHFR gene and produce endogenous/exogenous hormonal effects (Curtin et al., 2011). Lu et al. claimed that the individuals carrying MTHFR 677CC genotypes have protective effects with regard to esophageal squamous cell carcinoma. They also claimed that patients with high folate consumption showed a better survival rate when compared with the individuals with a low folate intake (Lu et al., 2011).
In the current preliminary study, we aimed at finding a possible linkage between a homozygous mutated (T allele) MTHFR gene and DTC. Genomic DNA was extracted from peripheral blood and genotyped by real-time PCR methods. The presented results report the allele frequency of two polymorphic codons in the systemic functional gene of MTHFR in Turkish DTC patients. Preliminary results of the current study showed that a polymorphic T allele in the 677 C>T codon in the MTHFR gene may be associated with a high risk of thyroid cancer in humans. These data suggest that MTHFR 677 C>T SNP may play a pivotal role in the development of DTC in humans, and the results should be supported by larger studies in different ethnic populations. Subic et al. have reported that the association with etiological factors, such as the MTHFR 677 C>T genotype with high alcohol intake, solely or in interaction, has an impact on oral cancer risk (Supic et al., 2011). Hustad et al. have claimed that thyroid dysfunction affects the folate and homocysteine metabolisms in the presence of MTHFR 677 C>T gene polymorphism by the modifying riboflavin cofactors synthesis (Hustad et al., 2004). Smoke and genetic susceptibility of MTHFR are the two suspected factors most closely associated with DTC according to the presented results. The same results were speculated by Rouissi et al. for tobacco, polymorphic MTHFR, MTR, MTRR genotypes, and bladder tumor stage association (Rouissi et al., 2011). Folates are common constituents in DNA synthesis, replication, repair, and DNA methylation reactions, as reported by Wang et al. (2008). Metabolic functional enzymes such as MTHFR, methionine synthase, and thymidylate synthase play a crucial role in folate metabolism and DNA methylation processes. Altered methylation status, such as hypo DNA methylation, may induce genomic instability and promote cancers due to variable MTHFR enzyme activity (Momparler and Bovenzi, 2000; Sato and Meltzer, 2006).
The current results indicated that individuals with the 677TT genotype had an 11.7% higher risk of having DTC than those with the 1928CC genotype. Furthermore, patients carrying both copies of the variant alleles (TT) showed a 2.33 times higher risk of developing DTC than their control counterparts. Although the A1298C polymorphism was not associated with DTC risk, a significant interaction with smoking and familial cancer history was observed in the current DTC patients.
In conclusion, the C677T polymorphism was significantly associated with DTC risk. It is also possible to speculate that the person with homozygous T-alleles in the MTHFR gene has a risk of developing epigenetic-mediated DTC due to the reduced activity of the MTHFR enzyme and diminished methyl sources. Our results should be supported by large-scale studies of representative DTC patients.
Footnotes
Author Disclosure Statement
There is no conflict of interest statement.