
Abstract
Background/Aims: Human serum paraoxonase1 (PON1), a high-density lipoprotein-associated enzyme, prevents oxidative modification of low-density lipoprotein and, thus, arrests the development of atheroma formation, whose major consequence is the development of coronary artery disease (CAD). A single-nucleotide polymorphism (SNP) Q192R in the coding region at pon1 locus is a determinant of PON1 activity. The relationship between PON1 activity and vascular disease may be influenced by the relationship of PON1 activity or PON1 SNP genotype to lipid and apolipoprotein (Apo) levels. The aim of the study is to ascertain the prevalence of PON1 Q192R polymorphism in male and female subjects with and without CAD along with its influence on ApoA-I and ApoB levels in Asian Indians. Methods: Determination of genotypes was carried out in 249 diagnosed CAD cases and in 243 age-, gender-matched asymptomatic controls by polymerase chain reaction-restriction fragment length polymorphism. Fasting plasma Apo-levels were estimated by immunoturbidimetric assay. Results: The genotype frequencies did not differ markedly between the overall CAD and control groups and in male and female subjects, suggesting a lack of any genotype-CAD correlation. ApoB levels were found to be higher in female patients carrying RR when compared with QQ genotypes (p=0.03) with no effect on controls. This may be attributed to the postmenopausal state of the women. Conclusion: PON1 Q192R can be used as the DNA marker test to evaluate the risk of CAD in postmenopausal Indian women with high ApoB.
Introduction
C
Human serum paraoxonase, PON1 is a Ca2+-dependent esterase (EC.3.1.8.1) of 43 kDa comprising 355 amino acids with the gene spanning a length of 27 kb on the long arm of chromosome7 (7q21.3-22.1) (Gan et al., 1991; Hassett et al., 1991; Humbert et al., 1993). PON1 messenger ribonucleic acid expression is limited to the liver, and a portion of the encoded protein is secreted into the plasma (Hassett et al., 1991), where it tightly binds to the high-density lipoprotein (HDL) particles associated with other protein components such as apolipoproteins (Apo)A-I and ApoJ (Blatter et al., 1993; Kelso et al., 1993).
The serum concentrations of HDL and HDL-associated ApoA-I have been long known to have an inverse relationship with the development of atherosclerosis, but the mechanism by which it influences the risk of vascular disease is still under active investigation. The initial focus of attention was on the role of HDL in reverse-cholesterol transport (Gwynne, 1993). However, recent studies have shown that HDL protects against low-density lipoprotein (LDL) peroxidation forming oxidized LDL (ox-LDL) particles (Mackness et al., 1993a) which are considered central to the initiation and progress of atherosclerotic events (Steinberg et al., 1989). Further studies have indicated PON1 as preventing lipid peroxide accumulation on LDL in vitro and in vivo (Mackness et al., 1993b; Watson et al., 1995). This has led to numerous clinical studies designed to assess the relationship of PON1 gene variants, its activity, or both to the coronary risk.
There exist 10- to 40-fold inter-individual variations in both, the PON1 concentration and activity. This is partly explained by the presence of two common genetic polymorphisms identified in the coding region of PON1 gene giving rise to amino acid substitutions at codon 55 (leucine to methionine substitution; L55M) and codon 192 (glutamine to arginine substitution; Q192R). Q192R polymorphism is the major determinant of the PON1 activity polymorphism; however, the position-55 polymorphism modulates its activity (Adkins et al., 1993; Humbert et al., 1993; Blatter et al., 1997). It has been shown that the PON1 R allozyme is less efficient at retarding the oxidation of LDL and HDL than is the Q allozyme because of the decreased hydrolysis of lipid peroxides by the R allozyme (Mackness et al., 1997).This has led to the conclusion that the lower the PON1 activity, the higher will be the accumulation of ox-LDL particles and, hence, the higher the coronary risk.
The association of variation in plasma lipoprotein traits with PON1 Q192R variants remains unsettled. The variation in PON1 was significantly associated with the variations in the plasma concentration of ApoB-related traits such as LDL, non-HDL, HDL-C, and ApoB itself in Canadian genetic isolates (Hegele et al., 1995). However, a majority of the studies in other populations show no such correlation with plasma lipoproteins such as plasma HDL-C, LDL-C, total cholesterol, and triglycerides (Antikainen et al., 1996; Herrmann et al., 1996). Studies carried out in Singaporean racial groups (Indians and Chinese) and in native Indians have also not found such a correlation (Sanghera et al., 1997; Pati and Pati, 1998). Recently, ApoA-I and ApoB have been proposed as relatively more sensitive indices of the risk of vascular disease than any cholesterol index (Walldius et al., 2001; Meisinger et al., 2005). Pathophysiologically based evidence and technical advantages of measuring Apos, especially ApoB, compared with LDL and HDL-C, also favor their clinical use in the routine assessment and treatment of dyslipidemias (Marcovina et al., 1993; Scharnag et al., 2001; Sniderman, 2002). Hence, these biomarkers would be better suited compared with the conventional lipid markers for genotype-phenotype analysis.
The current study was undertaken to ascertain the prevalence of PON1 Q192R polymorphism in male and female subjects with and without CAD along with its influence on ApoA-I and ApoB. To our knowledge, this is the first study that has been carried out in an admixture of the Asian Indian population wherein the impact of Apos on PON1 genotypes and disease risk will be evaluated.
Materials and Methods
Study subjects and enrollment
A DNA bank was prepared at Cumballa Hill Hospital & Heart Institute, Mumbai, India, in the year 2000-2002. Four hundred and ninety-two subjects from this data bank were included for the present case-control study. The study was approved by the Institutional Ethics Committee. Two hundred and forty-nine consecutive patients (mean age±standard deviation [SD], 57.5±10.6 years, 192 men and 57 women) who were admitted for coronary investigations or treatment comprised the case group. Among the CAD cases, 73% underwent diagnostic coronary angiography; 21%, for percutaneous transluminal coronary angioplasty; and 6%, for coronary artery bypass graft surgery. Acute myocardial infarction (AMI) had occurred in 33% of the cases and was assessed by typical electrocardiogram (ECG) changes (Minnesota code 1.1 or 1.2 in ECG) and by changes in levels of serum cardiac enzymes in circulation. Nearly 35% of the cases were diagnosed with diabetes mellitus, and around 43% were hypertensive.
The control group consisted of two hundred and forty-three unrelated, healthy individuals with an age range of 30-83 years (mean age±SD, 56.9±11.0 years,190 men and 53 women) who were drawn at random from the general population. None had a history that was suggestive of CAD or CVD or AMI, the presence of which was excluded by the Rose angina questionnaire (Rose et al., 1977). This group also had individuals with a history of diabetes mellitus or hypertension or a family history of CVD.
A standard questionnaire was filled for all subjects after having obtained their written informed consent. The questionnaire documented information on their demographic and socioeconomic status; family history of CVD, diabetes, and hypertension among first-degree relatives; or any other significant illness, lifestyle and other established coronary risk factors, details of current medication, tobacco use (smoking and/chewing), and alcohol drinking. A dietary recall of 24 h was also obtained from the subjects.
Estimation of Apos
Stored plasma (−80°C) that was aspirated at the time of blood collection was used for the analysis. Fasting EDTA plasma concentrations of ApoA-I and ApoB (preferentially ApoB100) were analyzed using an immunoturbidimetric assay (Orion Diagnostica) with calibration traceable to the International Federation of Clinical Chemistry primary standards. The coefficient of variation was found to be 5.51% for ApoA-I and 0.1% for ApoB assay. The assay is based on the measurement of immunoprecipitation in the liquid phase, and turbidity is measured using a clinical chemistry analyzer at a wavelength of 340 nm.
Genetic screening for PON1 Q192R polymorphism of exon 6
DNA stored in 10 mM Tris-HCl, 1 mM EDTA buffer (TE buffer), pH 8.0 at −80°C was used for genetic screening. PON1 genotyping for Q192R polymorphism was carried out using standard polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) methodology. PCR was carried out using a set of primers (Sigma-Aldrich) that was designed to amplify a 199bp DNA fragment encompassing the polymorphic region of Q192 (C
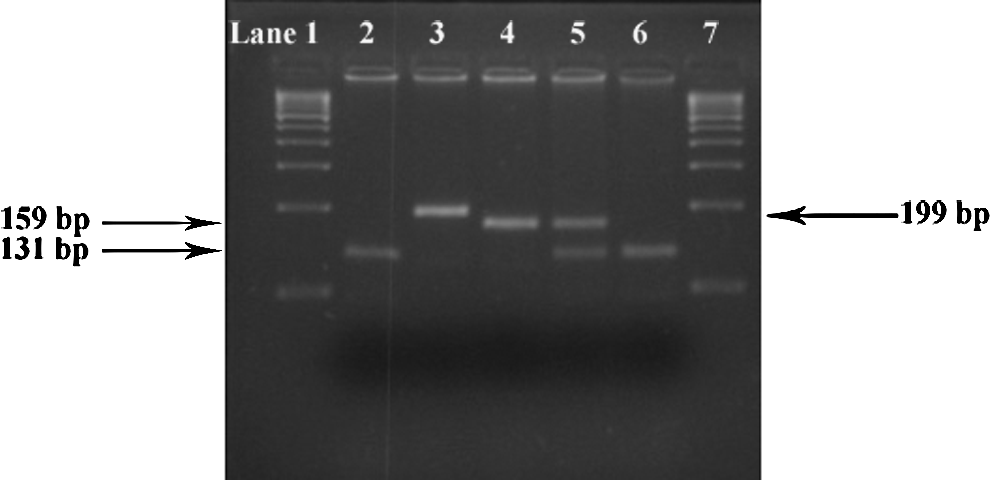
Detection of PON1Q192R by RFLP with RE Sau3AI on 3.5% agarose. Lanes 1, 7: marker 100 bp DNA ladder; lane 2: PCR product digested with RE: positive control: 131 bp+40 bp+28 bp; lane 3: undigested PCR control: 199 bp; lane 4: wild-type allele (QQ) cut by RE: 159 bp+40 bp; lane 5: heterozygote (QR) cut by RE: 159 bp+131 bp+40 bp+28 bp; lane 6: minor allele (RR) cut by RE: 131 bp+40 bp+28 bp. Note: 40 and 28 bp fragments run-off from the gel. PON1, paraoxonase1; PCR, polymerase chain reaction.
Statistical analysis
The allele and genotype frequencies of PON1-192 were calculated by direct counting. The conformity of genotype distribution to the Hardy-Weinberg equilibrium was determined using a chi-square goodness-of-fit test. A comparison of genotype frequencies in cases versus those in controls was evaluated by a chi-square test for a 2×2 contingency table. Odds ratio (OR) with 95% confidence intervals (95% CI) was used to test any association between genotype and disease. Student's t-test (continuous variables) or Pearson's chi-square test was applied for group comparison variables. One-way analysis of variance was performed for comparing the distribution of ApoA-I and ApoB among different PON1 genotypes of the study groups. All the statistical analyses were performed using IBM SPSS version 19.0 (SPSS, Inc., Chicago, IL).
Results
The general characteristics of the population under study are summarized in Table 1. Subjects were well matched for age, gender, body mass index, and smoking history. Known cases of diabetes, hypertension, and a family history of CVD were more in the CAD group. In contrast to healthy men, CAD male patients had significantly lower plasma ApoA-I levels (mean±SD g/L, 1.63±0.48 vs. 1.52±0.45; p=0.03, Table 1). A similar trend was observed when both the gender groups were combined for ApoA-I levels (p=0.02). On the other hand, ApoB levels were comparable for individual gender groups and for combined genders when compared between the two groups (Table 1). Female patients had higher ApoB and ApoA-I levels than the male patients (Table 1). A similar trend was seen in controls for ApoA-I levels, which were significantly higher in women than in men (mean±SD g/L, 1.92±0.52 vs. 1.63±0.48; p<0.0001, Table 1).
p<0.0001 values considered extremely significant.
Data available only for 241 CAD cases.
Data available only for 242 CAD cases.
Data available only for 240 CAD cases.
Data available only for 242 controls.
p<0.05 values considered significant.
—, signifies no value; BMI, body mass index; CVD, cardiovascular disease; HT, hypertension; NIDDM, non-insulin-dependent diabetes mellitus; MI, myocardial infarction; ApoA-I, apolipoprotein A-I; ApoB, apolipoprotein B; SD, standard deviation; CAD, coronary artery disease.
The genotype distribution for both the genders in CAD as well as control groups is shown in Table 2. The genotype frequencies for the population were in accordance with the Hardy-Weinberg equilibrium (p>0.05). The genotype frequencies and allele frequencies did not differ markedly between the overall CAD and control groups and between male and female subjects. The overall minor “R” allele frequency was found to be 0.39 in controls and 0.43 in CAD cases with no association between this variant and CAD [OR=1.12 (0.77-1.61); p=0.56, Table 2]. In case of men, the percentage of RR genotypes was higher in CAD cases (22.9%) as compared with the controls (14.2%), although this difference did not reach statistical significance [OR=1.7 (0.95-3.06); p=0.074, Table 2]. Gender played no significant role in genotype-disease correlation.
Overall genotype distribution of PON1 alleles (Q and R) among the gender groups for controls and CAD cases was insignificant (all p-values>0.05).
—, signifies no value; OR, odds ratio; CI, confidence interval; PON1, paraoxonase1.
Table 3 shows the distribution of mean±SD values for ApoA-I and ApoB among different PON1 genotypes in male and female subjects of both the study groups. The difference in the mean concentrations of ApoA-I and ApoB was not statistically significant for the overall control group as well as for the individual gender groups when compared across QQ, QR, and RR genotypes of the PON1Q192R polymorphism (Table 3). In CAD cases, male and female subjects did not contribute to any significant change in ApoA-I levels when compared among PON1 genotypes. However, ApoB levels were found to be higher in female patients carrying the risk “R” allele when compared with wild type (p=0.03, Table 3). No significant data were obtained on comparing the ApoB levels of PON1 genotypes in male patients.
A statistically significant difference observed across the PON1 genotypes in the CAD female group only when compared with ApoB levels (p<0.05); confirmed by one-way ANOVA.
ANOVA, analysis of variance.
Discussion
CAD is more prevalent in Asian Indians than in Chinese, Japanese, and Caucasian whites. The characteristics of CAD in Indian patients are well recognized to be different from those of other ethnic groups of the world, particularly Caucasian whites (Jha et al., 1993; Enas, 2000). India is recognized to have an ethnically diverse population (Bamshad et al., 2001). Since the distribution of PON1 frequency is ethnicity dependent, the data cannot be extrapolated from other populations.
Several studies have been conducted in different ethnic groups of the Indian population to demonstrate the association between the PON1 Q192R polymorphism and coronary risk. A case-control study carried out in residents of New Delhi has found the frequency of the QR genotype to be higher in Indian CAD patients than in controls, independent of their diabetes status (Pati and Pati, 1998). “R” allele frequency was also found to be higher in CAD subjects (0.45) than in controls (0.17). Though a statistically significant difference was observed, the population did not follow the Hardy-Weinberg frequencies of distribution law. This was not the case in our study group, which did not find any genotype-disease correlation but followed the Hardy-Weinberg frequencies of distribution law. Similar studies carried out in North Indians of Lucknow have also found that the Arg “R” allele is a significant risk factor for CAD. The association was stronger in the sub-sample of smokers, suggesting the plausible role of the environment (Agrawal et al., 2009). This supports the fact that the interaction between PON1 activity and smoking augments CAD risk. The present study cohort included very few control and CAD male smokers. Hence, the risk of CAD occurrence in a male smoker population in our current study is minimal. Another study reported in Andhra Pradesh state constituting mainly the South Indian cohort showed the PON1 Q192R polymorphism to possibly serve as one of the DNA biomarkers for detecting T2DM patients with CAD risk (Bhaskar et al., 2011). This finding could be influenced by consanguinity, which is a common feature in Andhra Pradesh. It is a well-known fact that consanguinity leads to the accumulation of mutations in a gene pool. This is the first study that analyzes the association between Q192R, CAD, and Apo levels in an admixture of the Asian Indian population.
PON1 frequency is well known in most populations of the world, but not all have found an association between Q192R polymorphism and coronary disease. It has been detected in Asian Indians (Dravidian ancestry) from Singapore (Sanghera et al., 1997), North-American Caucasian whites (Serrato and Marian, 1995; Bhattacharyya et al., 2008), Japanese (Odawara et al., 1997), and native Chinese (Osei-Hyiaman et al., 2001) but not in Chinese Singaporeans (Sanghera et al., 1997), Italians (Ombres et al., 1993), Koreans (Hong et al., 2001), Spanish (Ferre et al., 2002), and British Caucasians (Robertson et al., 2003). A meta-analysis of 43 studies by Wheeler et al. (2004) has shown an overall association between the Q192R polymorphism and CAD to be weak and of uncertain relevance. This is in agreement with our current study. The differences in the findings can also be explained by the differences in the study design, gene environment and gene-gene interactions, and other unknown or unestablished risk factors.
The prevalence of CAD in Indians is much lower in younger women (below 65 years) when compared with the age-matched men. This has led to the fallacy wherein CAD is considered the disease of men. CAD has now become the significant cause of disability and concern among Indian women (Enas et al., 2001). In the present study, we have determined the prevalence of the PON1Q192R polymorphism in male and female subjects with or without CAD, irrespective of their age. We have found that RR genotypes were more frequent in CAD male patients as compared with healthy males (23% vs.14%), although the difference was not statistically significant (OR=1.7, 95% CI: 0.95-3.06; p>0.05). No such trend was observed in women. There was a lack of genotype-disease correlation when gender groups were considered. However, there is need for more studies to be carried out in other ethnic regions of India involving a greater number of patients with regard to the gender groups. At present, no such data considering the gender groups are available for the people living in this country.
In the present study, a significant difference was observed in ApoB levels among female patients across the PON1 genotypes. This may be attributed to two reasons: the first being the postmenopausal state of the women. The mean age of the CAD female patients and control women was 60.9±8.4 years and 59.3±9.1 years, respectively. Natural menopause confers a three-fold increase in the risk of CAD (Kannel and Wilson, 1995). It is known that postmenopausal women are at a similar risk of developing CAD as are men of the same age rather than the premenopausal women (Stampfer et al., 1989). Menopause usually occurs between 45-50 years and on an average, 47 years (Padubidri and Daftary, 2004). In view of these findings, the women can be considered to be in their postmenopausal state with a greater CAD risk. The second interesting finding was that the highest ApoB level was found in the RR genotype across the PON1 genotypes of female CAD patients. The estrogen level drops drastically in women after menopause, which is followed by an abnormal increase in LDL-C levels and its associated ApoB levels (Matthews et al., 1989; Kalavathi et al., 1991). High ApoB, however, reflects a high number of atherogenic lipoprotein particles as very LDLs, intermediate-density lipoproteins, and LDL, each containing a single molecule of ApoB. This may lead to competition at the ApoB receptor, the LDL receptor, of peripheral cells (Chan and Watts, 2006). Since such a competition will prolong the residence time of pro-atherogenic LDL particles in the circulation, it may lead to a greater opportunity for them to undergo oxidation or any other chemical modifications. The ox-LDLs are known to promote a series of atherosclerotic events through lipid-laden macrophage foam cell formation and inflammatory responses (van Tits et al., 2011). “R” allele of PON1 is found to have low efficiency at retarding the peroxidation of LDLs than “Q” allele (Mackness et al., 1997). Considering all the facts just mentioned, postmenopausal women carrying the “RR” genotype can be considered susceptible to a higher coronary risk. In contrast to women, PON1 alleles did not contribute to any significant effect on both ApoA-I and ApoB in the male subjects in our study. To the best of our knowledge, this is the first study that demonstrates the correlation between ApoB and RR genotype-associated coronary risk in Indian women. However, large prospective studies are warranted in other ethnic groups of India that involve a greater number of postmenopausal women to determine the role of PON1 anti-oxidant activity and genotypes in view of lipoprotein levels in CAD patients.
In conclusion, though the PON1192R allele was not significantly associated with CAD in Asian Indians, ApoB levels were associated with the PON1 “R” allele in Indian CAD women. Hence, it can be concluded that PON1Q192R can be used as a DNA marker test to evaluate the risk of CAD in women with high ApoB in Asian Indians. This study will hopefully assist in designing the future genetic and phenotypic studies that investigate the underlying causes of CAD in Asian Indians.
Footnotes
Acknowledgments
The work was supported by the Baun Foundation Trust (BFT) at Cumballa Hill Hospital and the Heart Institute, Mumbai, and consumable grant was awarded to Chetana Deshpande by the University Grant Commission (UGC), Government of India. Deshpande was supported by the UGC fellowship and BFT. The authors thank researchers and medical staff of the Cumballa Hill Hospital and the Heart Institute for their help in conducting this study.
Author Disclosure Statement
No competing financial interests exist.