
Abstract
Background: MicroRNAs (miRNAs) are small, noncoding RNAs that are critical regulators of various diseases, including cancer, which may represent a novel class of cancer biomarkers. Aims: We hypothesized that microRNA-20a (miR-20a) and microRNA-203 (miR-203), which were altered in lymphatic metastatic tissues, could be directly assayed in the serum and used to detect the lymph node status of cervical cancer patients. Methods: We analyzed serum levels of miR-20a and miR-203 in 80 patients with stage I-IIA of cervical cancer by quantitative real-time polymerase chain reaction assay. Blood samples were collected before surgery and therapy. Logistic regression was used to measure the influence of different variables. Receiver operating characteristic analysis could evaluate the sensitivity and specificity in separating lymph node metastasis (LNM) (+) patients from LNM (−) patients by serum miR-20a and miR-203. Results: We found that the expression level of miR-20a was significantly higher in cervical cancer patients compared to healthy controls (p=0.004), patients with LNM tended to have overexpression of miR-20a (p=0.000), the odds ratio was 1.552. The expression level of miR-203 in cervical cancer patients was also significantly increased in comparison to the healthy patients (p=0.000), while downregulated miR-203 was correlated with LNM (p=0.001), the odds ratio was 0.849. When miR-20a was used for differentiation of LNM (+) patients from LNM (−) patients, the value of the area under the receiver-operating curve (AUC) was 0.734±0.058, the sensitivity and specificity of serum miR-20a were 75% and 72.5%, respectively, the cut-off point was 3.0. But the AUC of miR-203 was only 0.658±0.061, which showed low accuracy, the sensitivity and specificity were 65% and 62.5%, respectively, the cut-off point was 0.13. Conclusion: Our results suggested that the circulating miR-20a may be a potential biomarker for detecting the lymph node status of cervical cancer patients.
Introduction
P
Materials and Methods
Patients and samples
All protocols were approved by the Ethics Committee of the Guangxi Medical University. In total, 80 patients with cervical cancer of stage I-IIA who were diagnosed as having cervical squamous cell carcinoma before any treatments and 20 healthy control subjects from the Department of Gynecologic Oncology, Guangxi Tumor Hospital, were included in our study between 2010 and 2011. Forty patients had LNM, while the other matched 40 patients were without LNM. Patients who had coexisting malignant diseases or recurrence of cervical cancer were excluded. Serum samples were collected before the operation. The median age for patients was 49 years with a range from 25 to 69 years. The mean age for control subjects was 45 years, ranging from 33 to 57 years. After blood was drawn, tubes were kept upright at room temperature for 30 min and then stored in a 4°C refrigerator. After centrifugation at 4000 rpm, 4°C for 10 min, serum was extracted and distributed into aliquots of 0.5 mL per 1.5 mL tube. Then the serum tubes were stored at −80°C freezer. All sera were thawed ≤1 time.
Quantitative real-time polymerase chain reaction
RNA was extracted from serum using the miRcut miRNA isolation kit (Tiangen) according to the manufacturer's instructions. The reverse-transcription reactions were carried out using a MiraMas™ Kit (Bioo Scientific), which contained poly (A) polymerase used for polyadenylation of miRNA. Quantitative real-time polymerase chain reaction (qRT-PCR) was performed using a standard SYBR Green PCR kit (Takara, Japan). The primers were synthesized (Shanghai GenePharma) as follows: miR-20a forwards primer: 5′-TACGAT AAAGTGCTTATAGTGCAGGTAG-3′ miR-203 forwards primer: 5′-TACGAGTGAAATGTTTAGGACCACTAG-3′ U6 forwards primer: 5′-ATTGGAACGATACAGAGAAGATT-3′ Universal reverse PCR primer: 5′-GTCCTTGGTGCCCGA GTG-3′
The 20 μL PCR mixture consisted of 12.5 μL SYBR Green supermix, 3.5 μL RNase-free water, 1 μL forward primers, 1 μL reverse primers, and 2 μL reverse transcribed product. The reaction conditions were 40 amplification cycles of 95°C for 3 min, 95°C for 12 s, and 62°C for 50 s using a BIO-chromo4 (Bio-Rad) Real-Time PCR System. U6 was used as reference for miRNAs. Each sample was analyzed in triplicate. Comparative threshold cycle (CT) method-fold change (2−ΔΔCT) was used to analyze relative changes in gene expression.
Statistical analysis
All data was processed using PASW Statistics 16. As results did not display normal distribution, we chose to analyze the data with nonparametric methods. (Mann-Whitney U test between two groups and Kruskal-Wallis H test for three or more groups). Receiver operating characteristic (ROC) curves were generated to assess the diagnostic accuracy of each parameter; the sensitivity and specificity of the optimum cut-off point were defined as those values that maximized the area under the ROC curve (AUC). The Youden index (J) was used for the identification of the optimal cut-off point, which allowed the selection of an optimal cut-off point under the assumption that sensitivity and specificity were equally weighted (J=Maximum (sensitivity+ specificity−1) (Akobeng, 2007). All p-values were two tailed, and p<0.05 was considered significant. One way of interpreting the AUC curve is that a test with an area greater than 0.9 has high accuracy, while 0.7-0.9 indicates moderate accuracy, 0.5-0.7, low accuracy and 0.5 a chance result (Fischer et al., 2003).
Results
The levels of serum miR-20a and miR-203 in different groups
To define the use of circulating miRNAs as noninvasive markers for monitoring LNM in cervical cancer, we measured miR-20a and miR-203 expression levels in serum by qRT-PCR. The results showed that median fold changes of miR-20a were 0.72 (0.36-2.57) in healthy donors, 1.48 (0.37-5.79) in stage I patients, and 4.61 (2.15-5.52) in stage IIA patients (as in Fig. 1A). The expression level of miR-20a in cervical cancer patients was significantly higher compared to healthy female donors (p=0.004). The median fold changes of miR-20a were 6.56 (3.27-10.89) and 4.41 (1.18-7.29), in LNM (+) patients and LNM (−) patients, respectively. Patients with upregulated expression of miR-20a tended to have LNM (p=0.000) (as in Fig. 1B), there was also significantly overexpression of miR-20a between LNM (+) and LNM (−) in different stages (as in Fig. 1C). While the median fold change of miR-203 were 1.365 (0.338-2.702), 5.367 (1.37-5.441), and 5.4 (1.35-10.81) in healthy donors, stage I patients, and stage IIA patients, respectively (as in Fig. 1D). The level of miR-203 in cervical cancer patients was also significantly higher compared with healthy donors (p=0.005), but the level in LNM (+) patients was lower compared to patients without LNM (p=0.001) (as in Fig. 1E). There was downregulation of miR-203 between LNM (+) and LNM (−) in stage IIA (p=0.0012), but there was no different in stage I (p=0.0867) (as in Fig. 1F).
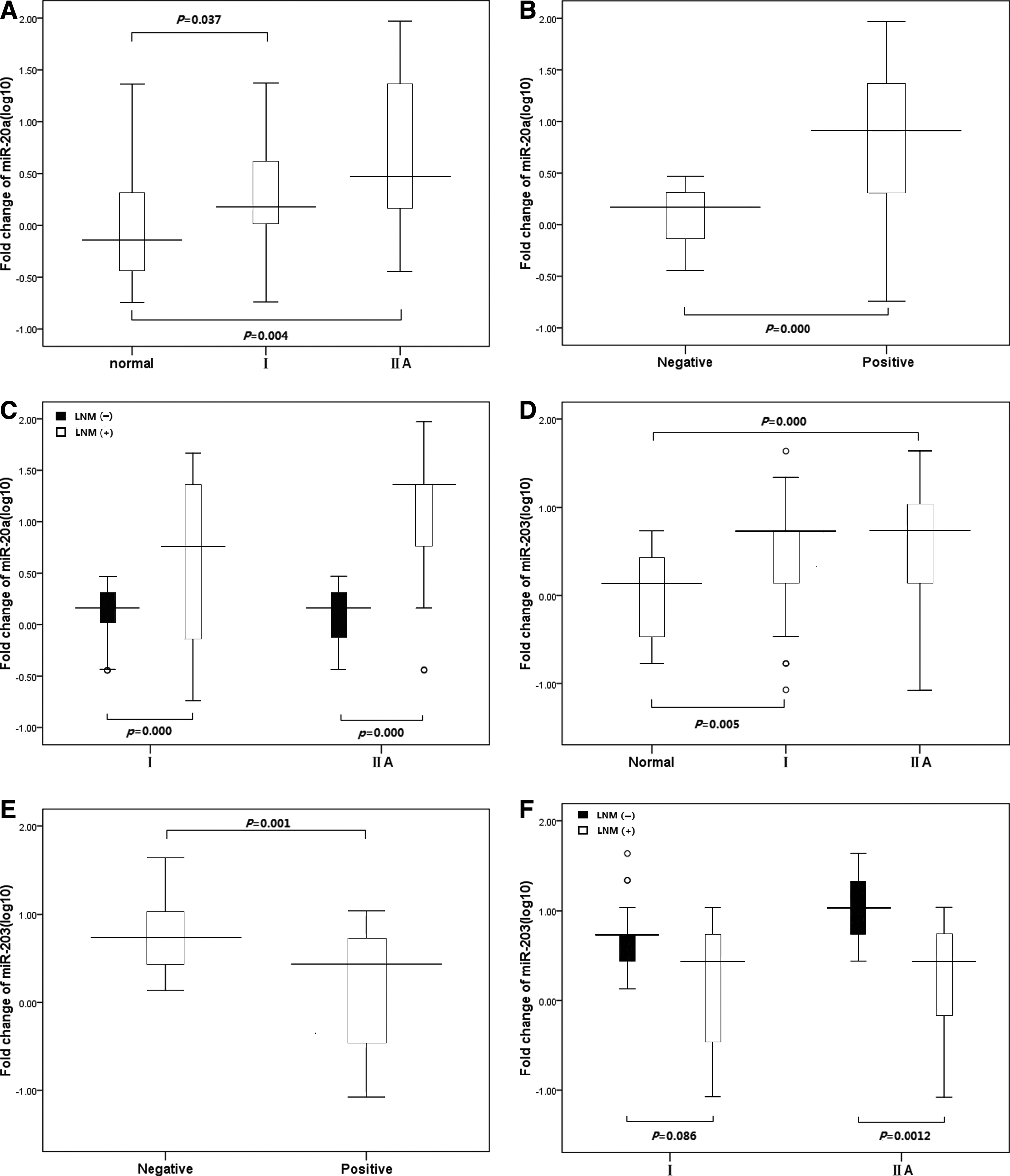
Expression of miR-20a and miR-203 in 80 patients with cervical cancer. MiR-20a and miR-203 were measured by quantitative real-time polymerase chain reaction. Data was presented as log10 of fold-change. Kruskal-Wallis H test was used to define the difference among normal controls and stages I-IIA of cervical cancer patients. The Mann-Whitney test was performed to examine the difference between patients of lymph node metastasis (LNM) (−) and LNM (+).
Logistic regression and ROC analyses
Logistic regression and ROC analyses were subsequently used to assess the odds ratio and sensitivity and specificity. Using miR-20a to distinguish LNM (+) patients from LNM (−) patients, the odds ratio was 1.552 (95% confidence interval [CI] 1.137-2.118), the AUC was 0.734±0.058, Youden index was 0.475, when the cut-off value was set to the optimal point of 3.0, sensitivity was 75%, and specificity was 72.5% (as in Fig. 2A). For miR-203, the odds ratio was 0.849 (95% CI 0.752-0.957), and the AUC was 0.658±0.061, low accuracy, Youden index was 0.275, when the cut-off value was set to the optimal point of 0.13, sensitivity was 65%, but specificity was 62.5% (as in Fig. 2B).

Receiver operating characteristic (ROC) analysis curve of miR-20a and miR-203 to distinguish LNM (+) patients from LNM (−) patients.
Discussion
Early stage cervical cancer has a relatively favorable prognosis which can be controlled by radical surgery or (chemo-) radiotherapy in most patients. LNM is the most important risk factor in surgically treated patients for recurrence or failure to survive. The detection of LNM has gained an increasingly important role in the treatment of the cervical cancer. However, there is still a high rate of missed diagnoses of the incidence of lymph node micro-metastasis. At present, the various methods for detecting LNM, such as CT, MR, and PET-CT, all have low sensitivity and specificity. Recently, many works indicated the surprising and exciting discovery that serum contains a large amount of stable miRNAs derived from various tissues/organs. In the healthy donors' serum, miRNAs usually come from blood cells, but in the patients' serum, miRNAs originate from microvesicles, exosomes, and apoptotic vesicles (Esquela-Kerscher and Slack, 2006; Lawrie et al., 2008; Taylor and Gercel-Taylor, 2008). Exosomes derived from tumor cells contain miRNA signatures characteristic of the biopsied tumor (Valadi et al., 2007). Interestingly, exosomal miRNAs are not found in samples from healthy control subjects. This might be the reason that many aberrant expressions can be found in the serum in cervical cancer patients and can be influenced by cancer-dependent variables, such as tumor stage, treatment, and prognosis-related factors. So the expression profile of these miRNAs showed great promise as novel noninvasive biomarkers for diagnosis of cancer and other diseases. Circulating miRNAs may have a putative role in cell-to-cell signaling and modulating gene expression at distant targets, which could affect disease progression, these exciting possibilities await exploration. Discoveries of these characteristics have opened up a new field in the molecular diagnosis of cancer. The high specificity of miRNAs compared with mRNAs indicates that these small molecules can serve as highly informative cancer biomarkers (Waters et al., 2012; Kawaguchi et al., 2013).
In spite of the growing evidence highlighting its relevance in various cancers, very few studies have systematically explored the role of the miRNAs in cancer with LNM. In this study, we performed a test on serum specimens from 80 cervical cancer patients. Two candidate miRNAs (miR-20a and miR-203), which were reported in cervical cancer cells and tissues studies but scarcely in serum, were examined to detect whether circulating miRNAs were associated with LNM of cervical cancer. Results showed miR-20a was significantly overexpressed in cervical cancer with LNM, while miR-203 was under expressed. miRNA-20a is known to belong to the miR-17-92 cluster, which is the most extensively studied cluster that has an oncogenic function. It comprises seven miRNAs, which reside in intron3 of the C13orf25 gene at 13q31.3 (Ota et al., 2004). This cluster is widely expressed in healthy tissues and is important for the regulation of the immune, hematopoietic systems, and lung development (Lu et al., 2007; Ventura et al., 2008; Xiao et al., 2008). However, it is situated in a chromosomal region that is commonly amplified and, therefore, is usually overexpressed in many kinds of tumor types (Huang et al., 2012; Kang et al., 2012; Wang et al., 2012). Huang et al. (2012) reported that miR-20a downregulated Fas expression in osteosarcoma; thus, contributing to the metastatic potential of osteosarcoma cells by altering the phenotype and allowing survival in the FasL (+) lung microenvironment. Kim et al. (2012) found that the high expression of miR-20a in advanced gastric carcinoma tissues may be a high risk factor associated with tumor penetration through serosa, LNM, distant metastasis, and poor long-term survival. Thus, we deduced miR-20a may play a role in the metastatic process. It also was confirmed as a novel diagnostic tool in cancers, such as large B-cell malignancies and nasopharyngeal carcinoma (Fassina et al., 2012; Zeng et al., 2012).
In the recent study, miR-203 had significantly low expression in cancer tissues compared to nontumor counterparts (Viticchiè et al., 2011; Takeshita et al., 2012; Gu et al., 2013), while there was also upregulation of miR-203 in pancreatic adenocarcinoma and breast cancer (Ikenaga et al., 2010; Madhavan et al., 2012), which is sufficient to induce a mesenchymal to epithelial transition with inhibition of cell proliferation, migration and invasiveness. We think the differential expression of miRNAs may be the result of tissue-specific differences (Baffa et al., 2009). Madhavan D found that circulating miR-203 can indicate circulating tumor cells status; miR-203 was overexpressed in pancreatic adenocarcinoma samples compared with normal pancreas, which indicate that miR-203 expression maybe a new prognostic marker (Madhavan et al., 2012). Subsequently, our study found that in using miR-20a to distinguish LNM (+) patients from LNM (−) patients, the odds ratio was 1.552 (95% CI 1.137-2.118), the AUC was 0.734±0.058, when the cut-off value was set to the optimal point of 3.0, sensitivity was 75%, and specificity was 72.5%, which indicates moderate accuracy, while using miR-203 the odds ratio was 0.849 (95% CI 0.752-0.957), the diagnostic information was below our expectations: the AUC was 0.658±0.061, when the cut-off value was set to the optimal point of 0.13, sensitivity was 65%, but specificity was 62.5%, low accuracy. So our results demonstrated miR-20a, but not miR-203, maybe an independent factor for LNM of cervical cancer, patients with upregulated expression of miR-20a tended to have LNM.
Surprisingly, miRNAs, particularly serum miRNAs, are resistant to RNaseA digestion and other harsh conditions, which potentially explain the stability of serum miRNAs. It was reported that intracellular miRNAs could be well preserved in the extracellular environment for at least 2 months after cell lysis. Beside serum, significant amounts of miRNAs have been found in extracellular human body fluids, including urine, saliva, and semen. The stability might be due to bonding to the Ago protein, a part of the RNA-induced silencing complex, which provides protection of miRNA (Turchinovich et al., 2012). Even so, there is a long way to go before circulating miRNAs are used to detect cancer; one of the crucial problems is the efficient and reproducible extraction of small amounts of miRNAs from plasma or serum. Therefore, higher yields of miRNAs have been consistently obtained from whole blood samples compared with matched serum or plasma samples and lower quantification cycles were performed in whole blood compared with matched serum and plasma samples in qRT-PCR experiments (Heneghan et al., 2010). On the other hand, the levels of a circulating miRNAs might be significantly higher or lower in various diseases, future studies may focus on combining the expression profiles of circulating miRNAs from all common diseases to obtain specific biomarkers for unique disease detection.
Above all, we suppose that miR-20a and miR-203 may play an important role in the malignant process of cervical cancer, especially invasion and metastasis, which could lead to poor prognosis. We observed that circulating miR-20a level could distinguish cervical cancer patients with LNM from nonmetastatic patients. Therefore, we hypothesized that the quantitative detection of the miR-20a in the serum could be useful as a clinical biomarker for screening LNM in the early stage of cervical cancer patients. Although our observations are promising, and miR-20a analytical characteristics reached values for clinical utility, our findings warrant further studies with a large cohort of patients to validate and develop the serum biomarker as a critical tool for cervical cancer.
Footnotes
Acknowledgment
This work was supported by Natural Science Foundation of Guangxi, China (Nos. 2011GXNSFA018184, 2013GXNSFBA019132 and 2013GXNSFBA019130).
Author Disclosure Statement
No competing financial interests exist.