
Abstract
Serotonergic pathways are known to play an essential role in the effects generated by antidepressants. Polymorphisms in serotonin receptor and transporter genes have been identified as an important factor. To investigate which of these polymorphisms may be useful to predict clinical outcome, we assessed their effect in a naturalistic clinical study. We studied the influence of the 5-hydroxytryptamine transporter (5-HTT) variable number of tandem repeats (VNTR), 5-HTTLPR/rs25531 and a 5-HTR2A intron 2 SNP with regard to response and side effects in 273 psychiatric inpatients. Main clinical assessments included Clinical Global Impressions ratings, paranoid depression scale self-rating scale and Dosage Record, and Treatment Emergent Symptoms (DOTES) Scale. We found significant associations between 5-HTTLPR/rs25531 S/LG alleles and response and side effects in 100 patients with selective serotonin reuptake inhibitor (SSRI) treatment (p=0.037, CGI-I≤2: 0% vs. 19% and p=0.0005, DOTES cluster c: 0.76 vs. 0.19). 5-HTT VNTR and 5-HTR2A intron 2 polymorphisms were associated significantly with adverse effects in patients with selective and nonselective SRI (5-HTT VNTR 12/12: n=170, p=0.0001, side effect rates: 51% vs. 19% and rs7997012 [A/A]: n=50, p=0.020, side effects rates: 43% vs. 11%). No impact of the polymorphisms on mirtazapine treatment was found. Our study confirms the influence of serotonergic polymorphisms at the receptor and transporter level on SSRI response and side effects, supporting previous reports based on various study designs. The effects were strong enough to be noticed clinically in this naturalistic setting. However, randomized controlled trials are warranted to provide unequivocal evidence of the clinical usefulness of pretherapeutic screening for these polymorphisms.
Introduction
S
Apart from pharmacokinetic variability, different response and side effects under antidepressant treatment may result from interindividual pharmacodynamic differences at the target of these drugs, monoamine neurotransmission.
The serotonin transporter (5-hydroxytryptamine transporter [5-HTT]) is mainly localized in brain stem and subcortical regions (Takano et al., 2011) and regulates reuptake of the neurotransmitter from synaptic cleft into nerve terminals. It is the primary site of action of selective serotonin reuptake inhibitors (SSRIs) and plays a role in the therapeutic mechanism of venlafaxine and tricyclic antidepressants (TCAs) as well. Several polymorphisms have been reported to be linked to the clinical outcome of antidepressants (Porcelli et al., 2011).
A 17 bp repetitive element in the second intron of the 5-HTT gene can occur as a 9, 10, or 12 repeat unit forming a variable number of tandem repeats (VNTR) polymorphism (rs57098334) (Lesch et al., 1994). The 12 repeat variant was shown to cause higher gene expression in vitro (Fiskerstrand et al., 1999) and in vivo (MacKenzie and Quinn, 1999). Additionally, the long allele was reported to be favorable concerning side effects and therapeutic success in patients treated with SSRI (Kim et al., 2000; Min et al., 2009).
A second variable region in combination with a SNP (rs25531) within, causes a length polymorphism in the promoter region (5-HTTLPR rs4795541), which was reported to influence transcription activity (Hu et al., 2006; Parsey et al., 2006; Praschak-Rieder et al., 2007). Both polymorphisms have been subject to various single drug studies concerning their impact on clinical outcome under antidepressant therapy [for detailed review see (Porcelli et al., 2011) and Discussion].
The serotonin receptor 5-HTR2A is one of the two major 5-HTR2 receptor subtypes in the human brain on cholinergic, glutamatergic, and dopaminergic nerve terminals. It is also widely distributed in the periphery (Quirion et al., 1985; Pazos et al., 1987; Aghajanian and Marek, 2000; Leysen, 2004).
5-HTR2A is a therapeutic target of many atypical antipsychotics, which are thought to reduce negative symptoms by antagonism or inverse agonism (Meltzer et al., 1989; Meltzer, 1999). Some antidepressants (mirtazapine, mianserine, nefazodone, trazodone) also show antagonistic effects at the 5-HTR2A receptor (Taylor et al., 1995; Frazer, 1997; Newton and Elliott, 1997), but most of them (TCAs, monoamine oxidase inhibitors, SSRIs) decrease receptor frequency through other mechanisms to reduce negative feedback of the autoreceptor (Gray and Roth, 2001; Yamauchi et al., 2006).
A promising new polymorphism has been linked to clinical outcome of the antidepressant citalopram [5-HTR2A intron 2 (rs7997012) (McMahon et al., 2006; Horstmann et al., 2010; Kishi et al., 2010)]. In a former study, an influence of this SNP on side effects in patients on olanzapine therapy was shown (Laika et al., 2009).
Taken together, there are some promising polymorphisms in serotonergic pathways that have been repeatedly associated with the clinical outcome of antidepressant therapy in single drug studies. However, the results have been inconclusive so far and more research is needed before any of these polymorphisms can be recommended for patient care. Since many of these associations have been reported in highly controlled patient populations atypical for every day care, we sought to examine whether an influence of any of these variants would be detectable in a naturalistic setting; thus, supporting their possible clinical relevance and the potential benefit of pharmacogenetic screening.
Patients and Methods
This explorative study included 273 psychiatric inpatients who were suffering from psychiatric diseases that required antidepressant therapy for at least 4 weeks. The design of the study was open and drug dosage could be adjusted as clinically indicated. Sedatives, mood stabilizers, antipsychotics, and nonpsychotropic medication were allowed as comedication. All prescribed drugs were administered at defined time points and under the supervision of the nursing staff. The treating psychiatrist and the patients were blind to genotype.
Patients younger than 18 years, patients suffering from organic disorders (international classification of diseases [ICD]-10: F0), substance-related disorders (ICD-10: F1), pregnancy, and breast-feeding were excluded from the study. No patients admitted to the hospital by law or authority direction were included. The study was approved by the local ethics committee and followed the principles of the Helsinki declaration. Patients were informed of the aims of the study and gave written informed consent which could be withdrawn at any time.
Patient data, including demographic data, smoking habits, weight, diagnosis, medical anamnesis, as well as drug treatment and length of hospitalization was determined at admission to the hospital and/or after 4 weeks in a structured interview and collected from medical charts. Changes in drug therapy, as well as concomitant medication were recorded during the first 4 weeks. Psychopathological state and response were assessed at admission to hospital as baseline and 4 weeks thereafter by means of the paranoid depression scale (PD-S) (Zerssen, 1976) self-rating scale (by patients) and the Clinical Global Impressions Scale (CGI) by the attending physician (Guy, 1976a). The PD-S self-rating scale consists of a P-scale to assess paranoid symptoms and a D-Scale to rate anxious-depressive symptoms. Patients were labeled as responders if their global improvement (CGI-I) was rated as very much improved or much improved after 4 weeks of treatment.
The treating psychiatrist also assessed the adverse drug events after 4 weeks of therapy according to the Dosage Record and Treatment Emergent Symptoms (DOTES) Scale (Guy, 1976b), including a rating (none, mild, moderate, marked) for each of the single items. The scale includes 30 single items and is organized in five clusters: cluster a (mental side effects), cluster b (neuromuscular symptoms), cluster c (anticholinergic/gastrointestinal symptoms), cluster d (cardiovascular symptoms), and cluster e (other symptoms). Side effects were evaluated as “positive” for an overall side effects rating of moderate/marked and probably caused by the drug.
5-HTT polymorphisms (5-HTT VNTR, 5-HTTLPR, 5-HTT rs25531 A/G) and the 5-HTR2A intron 2 SNP were examined by thermocycler assay, respectively, real-time PCR cross validated with RFLP methods and gel electrophoresis (Popp, 2006; Laika, 2009). The HWE of the analyzed genetic variations was checked and the obtained frequencies were compared to published literature (5-HTT VNTR: p=0.933, 5-HTTLPR: p=0.639, rs25531: p=0.258, 5-HTR2A intron 2: p=0.085).
The effect of the polymorphisms in serotonergic pathways was assessed for those patients exposed to the mode of action of antidepressant drugs and independent from the patients' exact diagnosis, history, or comedication in this naturalistic setting. Patients were divided into medication groups as displayed in Figure 1.
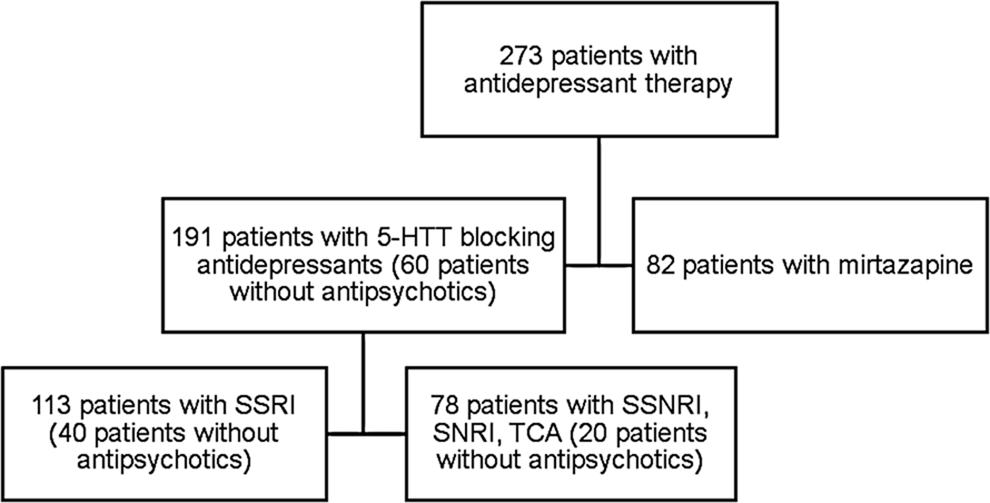
Medication groups. SSRI, selective serotonin reuptake inhibitor; SSNRI, selective serotonin norepinephrine reuptake inhibitor; SNRI, selective norepinephrine reuptake inhibitor; TCA, tricyclic antidepressant; 5-HTT, 5-hydroxytryptamine transporter.
As many atypical antipsychotics target 5-HTR2A, analyses for the intron 2 polymorphism concerning clinical outcome of antidepressants were done in medication subgroups that consisted of patients receiving selective and nonselective SRIs but no antipsychotic drugs.
Dependent variables were PD-S D scores, CGI scores, DOTES sum scores, overall side effects rating and objective available data (length of stay).
To assess differences in daily dose, relative doses were calculated based on the daily dose as defined by the WHO for each drug (World Health Organization, 2010).
According to the previous findings, patients with the 5-HTT intron 2 VNTR homozygous variant with 12 alleles were assessed versus the subjects with heterozygous genotype and those with two shorter alleles (9/10 or 10/10 genotype).
The high expression variant LA (i.e., 5-HTTLPR L-allele in combination with rs25531 A-allele) of the 5-HTT promoter polymorphism was compared to the 5-HTTLPR S-allele and the LG variant (i.e., 5-HTTLPR L-allele in combination with rs25531 G-allele).
Statistical analysis was performed using PASW Statistics 18. Two-tailed p-values<0.05 were considered to be of statistical significance. Fisher's exact test and the chi square test were used to analyze categorical variables. Associations between ordinal variables were analyzed using Kendall rank correlation coefficient. As the analyzed quantitative variables were non-normally distributed, they were compared by nonparametric tests (Mann-Whitney U-test or Kruskal-Wallis test). Odds ratios (OR) and Cohen's d effect size were calculated to quantify the strength of the significant relationships. Due to the explorative nature of this study, no correction for multiple testing was made and all shown p-values are nominally significant.
Results
Data were available for 273 Caucasian inpatients receiving psychoactive therapy. A subpopulation of 191 patients was treated with 5-HTT-blocking antidepressants (64 males, 127 females, age 18-89, and 77 smokers). Eighty-two patients were medicated with mirtazapine (35 males, 47 females, age 19-81, and 27 smokers).
The antidepressant drugs acting mainly via 5-HTT are listed in Table 1. Information about additional psychoactive medication is indicated in Figure 2 and other comedication is listed in Table 2.
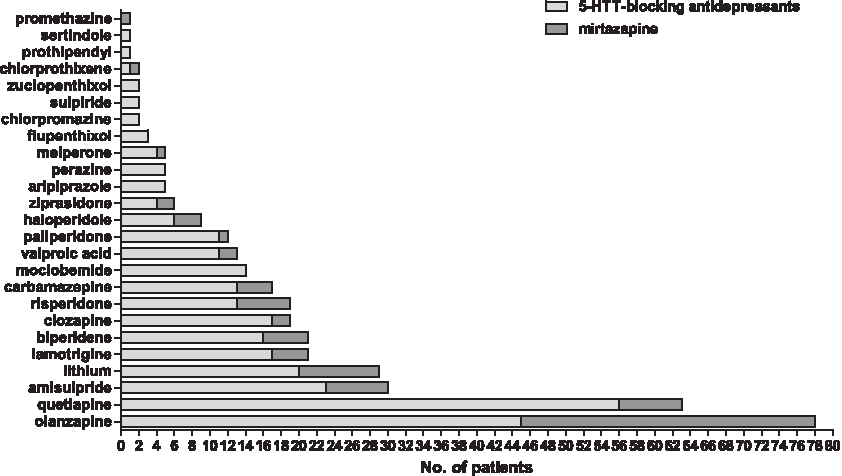
Additional psychoactive medications of the study populations.
5-HTT, 5-hydroxytryptamine transporter; SSRI, selective serotonin reuptake inhibitor; SSNRI, selective serotonin norepinephrine reuptake inhibitor; SNRI, selective norepinephrine reuptake inhibitor; TCA, tricyclic antidepressant.
ACE, angiotensin converting enzyme.
Baseline characteristics separated by medication group are displayed in Tables 3 and 4. Subjects with 5-HTT blocking antidepressants received significantly higher relative defined daily doses, had lower age of onset and longer hospitalization time than those with mirtazapine (p<0.001).
Mann-Whitney U-test.
BMI, body mass index; CGI, Clinical Global Impressions Scale; DOTES, Dosage Record and Treatment Emergent Symptoms; IQR, interquartile range; PD-S, paranoid depression scale.
ICD, international classification of diseases.
No significant baseline differences were observed for the different genotypes in patients with 5-HTT blocking antidepressants (Table 5).
Patients without antipsychotics.
Kruskal Wallis test.
Mann-Whitney U-test.
Chi2 test.
Fisher's exact test.
VNTR, variable number of tandem repeats.
Mirtazapine-treated patients differed in their smoking habits by 5-HTTLPR/rs25531 genotype (p=0.026). No other significant genotype dependent baseline differences were found in this subgroup (Table 5).
CGI scores were available for 233 patients. In 186 patients, PD-S D scores have been assessed and for 245 subjects DOTES scores could be obtained. Results of associations between these variables and genotypes are shown in the sections of several medication groups.
SSRI, SSNRI, SNRI, TCA (n=191)
In accordance with preliminary analyses in a subsample of the investigated set (n=44) (Popp et al., 2006; 2010), patients with two 5-HTT VNTR 12 alleles displayed higher rates of moderate to marked side effects.
51% of homozygous 12 allele carriers suffered from moderate to severe side effects. In contrast, only 19% of heterozygous genotypes (9/12 or 10/12) and 19% of patients with 9/10 or 10/10 genotype were affected by side effects (Table 6). Patients did not differ significantly in their hospitalization time by genotype (68 days vs. 65 days vs. 52 days, p=0.349).
Chi2 test.
Fisher's Exact test.
Two 5-HTT VNTR 12 alleles were significantly associated with higher rates of anorexia, weight change and headache (cluster e) (p=0.009). At a trend level, this genotype was associated with more neuromuscular adverse effects (cluster b) (p=0.056). No differences were found for other DOTES clusters concerning this 5-HTT VNTR (cluster a: p=0.857, cluster c: p=0.111, cluster d: p=0.434).
No significant differences between response or the PD-S D value changes by genotype were observed (Tables 7 and 8).
Patients were labeled as responders if their global improvement (CGI-I) was rated as very much improved or much improved after 4 weeks of treatment.
Fisher's exact test.
Chi2 test.
Difference between scores after 4 weeks and baseline (median [IQR]).
Mann-Whitney U-test.
Kruskal Wallis test.
When comparing all subjects with the 5-HTT VNTR 12/12 genotype, those patients treated with 5-HTT-blocking antidepressants suffered more frequently from side effects (Table 6). Concordantly, they tended to stay longer in hospital than patients with the same genotype and mirtazapine as antidepressant medication (68 days vs. 53 days, p=0.082).
The investigation of 5-HTTLPR on side effect rates in patients, which received predominantly 5-HTT-blocking antidepressants displaying the following: 5-HTT LL: 18% (n=67), LS: 38% (n=73), SS: 40% (n=30), Chi2 test, p=0.015, n=170.
In this study, we considered the additional impact of rs25531 on 5-HTT in vitro expression (Praschak-Rieder et al., 2007).
In contrast to 5-HTT VNTR genotype, no significant associations were observed between 5-HTTLPR/rs25531 and the occurrence of side effects in this medication group (Table 6).
No significant influence of the polymorphism on response or PD-S D score change was found (Tables 7 and 8).
SSRI (n=113)
Patients treated exclusively with SSRIs suffered more often from moderate to severe adverse effects when they carried two 5-HTT VNTR 12 alleles (53%). In contrast, 16% of the subjects with heterozygous genotype and 29% with two short alleles (9/10 or 10/10 genotype) were impaired by adverse effects (Fig. 3, OR: 6.1 and 2.7, 95% confidence interval: 2.2-17.0 and 0.8-9.5). No significant differences were found for single DOTES clusters (cluster a: p=0.293, cluster b: p=0.217, cluster c: p=0.956, cluster d: p=0.947, cluster e: p=0.183).
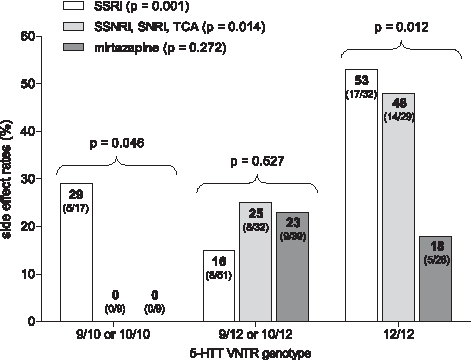
5-HTT VNTR: Side effect rates.
Despite a trend to shorter treatment time for patients with short 5-HTT VNTR alleles:
9/10 or 10/10: 43 days, 9/12 or 10/12: 69 days, 12/12: 74 days, p=0.067, n=113, no significant variation of response (Fig. 4) or PD-S D score after 4 weeks of treatment was observed amongst the genotypes (p=0.191).
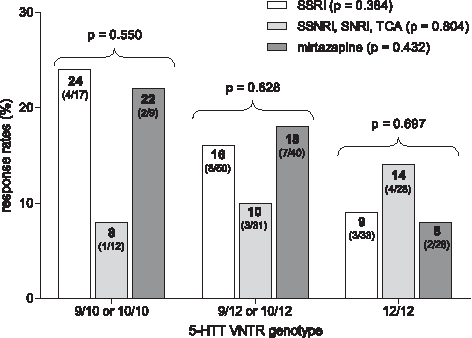
5-HTT VNTR: Response rates.
Side effect rates did not differ significantly between 5-HTT SS, SLG, LGLG genotype in patients receiving solely SSRI as antidepressant medication (Fig. 5), but DOTES sum scores tended to be higher in patients with 5-HTT SS, SLG, LGLG genotype (n=100, p=0.067). There was a highly significant correlation between gastrointestinal side effects (cluster c) and 5-HTT S or/and LG alleles (Fig. 7, Kendall's tau [τ] coefficient: 0.3, effect size: 0.8). No correlations were found between other side effect clusters and 5-HTT S or/and LG alleles (cluster a: p=0.908, cluster b: p=0.121, cluster d: p=0.592, cluster e: p=0.512).

5-HTT LPR/rs25531: Side effect rates.
Additionally, these patients responded less often and less pronounced to the treatment (Figs. 6 and 8, Kendall's tau [τ] coefficient: 0.2, effect size: 0.7, OR: 9.7, 95% confidence interval: 0.6-169.3) and stayed longer in hospital compared to carriers of at least one LA-allele (141 days vs. 55 days, p=0.003).
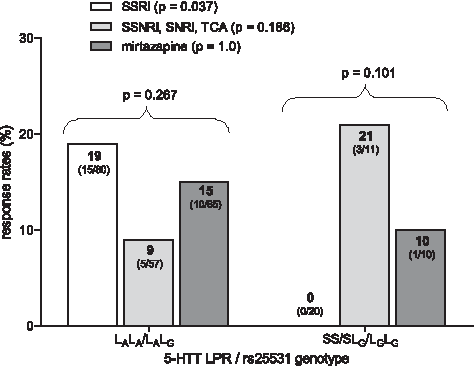
5-HTTLPR/ts25531: Response rates.
Concordantly, PD-S depression score after 4 weeks of treatment tended to be higher in patients with SS, SLG, LGLG genotype compared to LA-allele carriers (19 vs. 12, p=0.053).
Comparing all patients of the study population with a 5-HTT SS, SLG or LGLG genotype, those receiving only SSRIs as antidepressant therapy, suffered from more gastrointestinal side effects at a trend level (Fig. 7, Kendall's tau [τ] coefficient: 0.2, effect size: 0.1), tended to have higher CGI-S ratings after 4 weeks of treatment (Fig. 8, Kendall's tau [τ] coefficient: 0.2, effect size: 0.6) and stayed significantly longer in hospital than patients with mirtazapine treatment (141 days vs. 101 days, p=0.007).
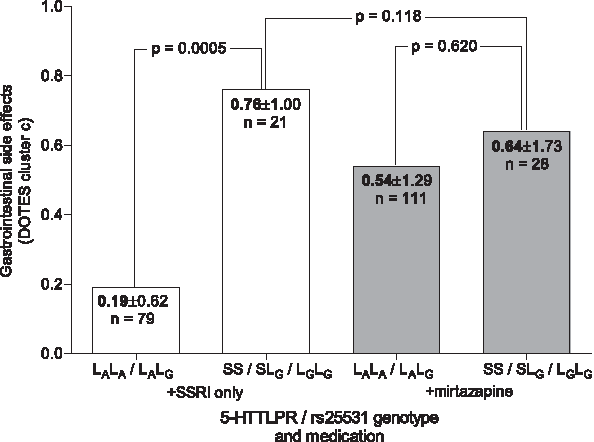
5-HTTLPR/rs25531: Gastrointestinal side effects.

5-HTTLPR/rs25531: CGI-S scores after 4 weeks.
We assessed whether the combination of a 5-HTT SS, SLG, or LGLG genotype with two 5-HTT VNTR 12 alleles is linked to higher risk to experience more frequently moderate or marked adverse effects compared to only one of the genotypes. However, the combination of both alleles was not associated with higher side effect rates (55% for both alleles vs. 53% for 5-HTT VNTR 12/12 and 43% for 5-HTT SS, SLG, or LGLG).
SSNRI, SNRI, TCA (n=78)
Subjects of this subgroup displayed significantly higher side effect rates when they had a 5-HTT VNTR 12/12 genotype (Fig. 3). Patients with two long alleles suffered more frequently from neuromuscular adverse effects (cluster b), weight change, anorexia, and headache (cluster e) compared to other genotypes (p=0.035, p=0.024). Additionally, they tended to have more gastrointestinal side effects (cluster c, p=0.071). No associations were found for other DOTES clusters (cluster a: p=0.375, cluster d: p=0.220).
No significant impact of this polymorphism on response rates and on PD-S D score change was detected in this medication group (Fig. 4, p=0.216).
Nothing was found concerning the influence of 5-HTTLPR/rs25531 on treatment outcome in this patient subgroup (Figs. 5 and 6).
Mirtazapine (n=82)
Eighty-two patients who received mirtazapine did not differ significantly in response, PD-S D score change or the occurrence of adverse effects concerning their 5-HTT VNTR or 5-HTTLPR/rs25531 genotype (Tables 7, 8, and 6).
SSRI, SSNRI, SNRI, TCA without antipsychotics (n=60)
Subjects with 5-HTR2A intron 2 A/A genotype displayed a higher side effect rate than G-allele carriers. Accordingly, the hospitalization tended to be longer for patients with A/A genotype (Table 9).
Fisher exact test.
Mann-Whitney U-test.
1. Patients with SSRI (n=40) and 5-HTR2A intron 2 A/A genotype suffered from significantly more side effects compared to G-allele carriers (Table 9). No significant associations with single DOTES clusters were observed. However, patients with A/A genotype tended to suffer more frequently from anorexia, weight change, and headache (cluster e, p=0.066).
2. Subjects with selective serotonin norepinephrine reuptake inhibitor (SSNRI), selective norepinephrine reuptake inhibitor (SNRI) or TCA (n=20) displayed more moderate or marked side effects when carrying the A/A genotype, but the results were not significant (A/A: 40%, G-allele: 14.3%, p=0.272, n=19).
The negative effect of the 5-HTR2A intron 2 polymorphism was only seen in those patients receiving antidepressants acting as serotonin reuptake inhibitors, but not in subjects treated with mirtazapine (n=25, p=1.0).
No effect of this SNP on CGI or PD-S score rating was observed (p=0.609, p=0.271).
Discussion
5-HTT Polymorphisms
The 5-HTT VNTR polymorphism has been the subject of several studies concerning its impact on clinical outcome of antidepressant therapy; however, with inconsistent results.
Two studies revealed an advantage for Asian patients carrying two 12 repeat variants in response to SSRI therapy (Kim et al., 2000; Min et al., 2009). However, Mrazek et al. (2009) reported lower remission rates for citalopram patients of Caucasian ethnicity with 12/12 genotype. Other research groups did not find associations between these genetic variants and response or side effects in patients treated with sertraline or venlafaxine (Dogan et al., 2008; Lee et al., 2010). These contradictory findings might result from the different evaluated ethnicities which are possibly associated with additional variations within the 5-HTT VNTR sequence (Lovejoy et al., 2003).
In concordance with preliminary analyses in a subsample of the investigated set (n=44) (Popp et al., 2006, 2010), patients of our naturalistic study showed a treatment benefit for Caucasian patients with 9/10 or 10/10 genotype because of fewer side effects with 5-HTT-blocking antidepressants. The effects were accompanied by longer hospitalization times for patients with two 5-HTT VNTR 12 alleles supporting the findings of Mrazek et al. We found an influence of the polymorphism on side effects in both 5-HTT blocking medication groups; however, the effect was more pronounced in patients with SSRI. Patients with 5-HTT VNTR 12/12 genotype suffered from side effects up to four times more frequently than other genotypes when they received 5-HTT blocking antidepressants. For those patients, therapeutic success might be improved by choosing antidepressant drugs with other therapeutic targets than 5-HTT.
A meta-analysis of 5-HTTLPR association with antidepressant outcome considered 19 studies performed in Caucasians and included 2785 subjects with SSRI treatment (Porcelli et al., 2012). The authors confirmed the effect of 5-HTTLPR on SSRI remission and response with evidence of better outcome in patients with L allele compared to SS genotype.
For rs25531, only a few studies concerning antidepressant response are available. The LA variant was reported to be associated with a more pronounced treatment response to fluoxetine (Kraft et al., 2005) and various antidepressants (Baffa et al., 2010) in patients with depression and with generalized social anxiety disorder (Stein et al., 2006). No difference in response rate was found in 135 outpatients with escitalopram therapy (Maron et al., 2009). However, an increased risk of SSRI related side effects was found for S allele carriers in that population. Associations between 5-HTTLPR S allele and more side effects on treatment with SSRI are currently described in five additional studies with different sample sizes (n=27-1655) (Mundo et al., 2001; Perlis et al., 2003; Murphy et al., 2004; Hu et al., 2007; Smits et al., 2007). However, only in two of them have the combined effects of 5-HTTLPR and rs25531 been analyzed (Hu et al., 2007; Maron et al., 2009). Three smaller studies with sample sizes between 35 and 72 subjects did not detect associations between 5-HTTLPR genotype and adverse effects in patients treated with SSRI (Takahashi et al., 2002; Ng et al., 2006; Tanaka et al., 2008).
In a pilot study with a smaller subsample of our study population treated with HTT-blocking antidepressants (n=44), the 5-HTT LL genotype was significantly associated with fewer side effects compared to other genotypes (Popp et al., 2006). The investigation of a higher total number of patients (n=170) displayed again the least side effect rate for patients with 5-HTT LL genotype. The associations were weaker in our total population, but the impact of this polymorphism on the occurrence of side effects remained significant in a sample, including more patients compared with former analyses. However, less detailed genotyping which only included the determination of 5-HTTLPR alleles had been performed in that pilot study in contrast to this investigation. When considering rs25531 we found a significant correlation with side effects, response and remission. This was, however, only seen in patients receiving SSRIs and is in line with the results of Hu et al. (2007) in 1655 outpatients with major depressive disorder (STAR*D Level1). They reported subjects with S or LG alleles to experience more citalopram induced side effects. As reported by Maron et al. the group did not find associations between response and the genetic variants. While Hu et al. and Maron et al. investigated outpatients, we analyzed associations between 5-HTTLPR/rs25531 and antidepressant outcome in psychiatric inpatients. As the correlation of the variants to gastrointestinal side effects was more pronounced compared to CGI-S score change, possibly, a more regular medication in hospital compared to ambulant therapy could explain the observed association to response variation. Additionally, we investigated the effect of the polymorphisms on treatment with various SSRI in contrast to the other teams. Kraft et al. (2005) reported better response for 96 fluoxetine patients with LA variant. As our study population included patients with fluoxetine treatment, this might be another reason for a detected association with response and remission.
Our results militate in favor of integrating rs25531 in association analyses concerning 5-HTT gene variations and treatment outcome. They are in concordance with the majority of previously published results and support the role of the LA variant in a naturalistic setting; thus, supporting their potential clinical relevance.
In our study, therapy with mirtazapine acting via pathways other than serotonin reuptake inhibition was not affected by 5-HTTLPR and rs25531. Patients homozygous for unfavourable S or LG alleles might, therefore, profit from switches to antidepressants other than SSRI.
5-HTR2A intron 2 SNP
In a recent study with 1953 depressive patients, who were treated with the SSRI citalopram, a highly significant and reproducible association between treatment outcome and a marker in intron 2 of 5-HTR2A (rs7997012) was found. Participants that were A/A homozygous had an 18% reduction in absolute risk of having no response to treatment, compared with those homozygous for the other allele (McMahon et al., 2006). Peters et al. (2009) support this observation. They found an association between this SNP and better response in patients with citalopram therapy. However, on treatment with various antidepressants a more pronounced response for the G allele was reported (Horstmann et al., 2008). No influence of the SNP on response was found in 760 patients of the GENDEP project treated with escitalopram or nortriptyline (Uher et al., 2009).
In our SSRI subpopulation (n=40), no effect of rs7997012 on treatment response was observed. The very small size and different diagnoses in this study do not allow any final conclusion, neither with regard to treatment response nor side effects.
However, patients in our SSRI subpopulation with A/A genotype suffered from significantly more side effects. Of note, in this context, is that olanzapine-treated patients (without additional antidepressants) also suffered from more side effects when they carried an A/A genotype (n=50, p=0.002 for AA vs. GG and p=0.018 for AA vs. GA) (Laika et al., 2009). The underlying mechanism is possibly linked to the 5-HTR2A antagonistic effect of atypical antipsychotics attenuating negative symptoms of schizophrenia which is why atypicals are also used to treat severe depressive episodes and bipolar disorder (Tollefson et al., 1998; Gao et al., 2011).
Nothing is known about the polymorphisms' impact on 5-HTR2A activity. It has, however, been reported to influence 5-HTT binding potential and therefore, central serotonergic transmission (Laje et al., 2010). This might explain at least partially the observed frequency differences of side effects between rs7997012 genotypes in both examined medication groups despite unequal therapeutic targets.
Study limitations
There are a number of limitations to our study. First of all, the sample size for some of the examined subgroups was partly too small to be conclusive.
Response was assessed by CGI scale and not with the more detailed Hamilton Depression Scale or Montgomery-Åsberg Depression Rating Scale. However, in our study population, additionally, a self-assessment using PD scale was carried out by patients.
The study was not a randomized placebo-controlled design and patients were not evaluated for longer than 4 weeks what might prevent the detection of some associations and could be a reason for small effect sizes.
Despite a controlled medication intake of all patients, the inclusion of noncompliant subjects cannot be categorically excluded. It, however, can be assumed that the noncompliance rate of our population is substantially lower as compared to outpatient samples.
Inclusion criteria were very broad, patients had different diagnoses, partially concomitant personality disorders and the influence of comedication cannot be fully evaluated.
Conclusions
To our knowledge, this is the first naturalistic study showing an effect of the described polymorphisms in psychiatric inpatients treated with common therapy regimens, including various psychoactive and other comedication. In contrast, no associations were found between any of the examined polymorphisms and response or side effects in patients treated with mirtazapine, which acts via other pathways. This indirectly supports the notion that the studied polymorphisms may be of clinical relevance in patients treated with substances acting via the serotonergic pathway.
Pretreatment identification of these genotypes may help to shorten the length and cost of hospitalization and lead to improved patient care. Prospective studies are needed to provide more evidence for pretherapeutic genotyping.
Footnotes
Author Disclosure Statement
In the last three years Stefan Leucht has received honoraria for lectures from AstraZeneca, Bristol-Myers Squibb, ICON, Eli Lilly, Janssen, Johnson & Johnson, Roche, Sanofi-Aventis, Lundbeck and Pfizer; for consulting/advisory boards from Roche, Eli Lilly, Medavante, Bristol-Myers Squibb, Alkermes, Janssen, Johnson & Johnson and Lundbeck. Eli Lilly has provided medication for a study with SL as primary investigator.
For Julia Staeker, Barbara Laika, and Werner Steimer, no competing financial interests exist.