
Abstract
Aim: Polymorphisms of xeroderma pigmentosum complementation group C (XPC) are thought to have significant effects on prostate cancer (PCa) risk. The aim of our study was to evaluate the impact of XPC gene polymorphisms on PCa risk by using a meta-analysis. Methods: Data were collected from the following electronic databases: PubMed, EMBASE, Elsevier Science Direct, Cochrane Library, and CNKI, with the last report up to April 30, 2013. Odds ratios with 95% confidence intervals were used to assess the strength of the association. Results: A total of five separate case-control studies (1966 cases and 1970 controls) were included in this meta-analysis. Meta-analysis was performed for the rs2228001 and PAT+/−polymorphisms. We did not detect a significant association between rs2228001 polymorphism and PCa (p>0.05). Similar results were found in stratification analyses by ethnicity and tumor stage. We detected a significant association of PAT+/−polymorphism with PCa (p<0.05). In stratification analysis, we did not detect a significant association of PAT+/−polymorphism with risk of bone metastasis in PCa patients (p>0.05). Conclusion: These analyses suggest that XPC gene PAT+/−polymorphism, but not rs2228001, likely contributes to susceptibility to PCa.
Introduction
A decline in DNA repair may lead to carcinogenesis (Malins et al., 2001). Nucleotide excision repair (NER) is a major DNA repair pathway that can eliminate a wide variety of DNA lesions, including UV-induced photolesions and chemical carcinogen-induced bulky DNA adducts (Wood et al., 2001). Studies have indicated that individuals with decreased NER capacity are at increased risk of carcinogenesis (van Steeg, 2001), and variations in NER genes may contribute to decreased NER capacity (Pastorelli et al., 2002). Thus, variations in NER genes may modulate susceptibility to cancer. The xeroderma pigmentosum complementation group C (XPC) is a component of the NER pathway and had been reported to be involved in the early damage recognition and initiation of NER (Thoma and Vasquez et al., 2003). The XPC gene is located on chromosome 3p25, and many polymorphisms have been identified in the gene (Khan et al., 2002). Recently, a number of molecular epidemiologic studies have been performed to evaluate the role of XPC gene polymorphisms in the risk of developing PCa (Hirata et al., 2007; Agalliu et al., 2010; Liu et al., 2012; Mandal et al., 2012; Mittal and Mandal, 2012), but the results are inconclusive. Single studies may have been underpowered to detect modest effects of XPC gene polymorphisms on PCa risk.
Meta-analysis is a means of increasing the effective sample size under investigation through the pooling of data from individual association studies, thus enhancing the statistical power of the analysis for the estimation of genetic effects (Egger et al., 1997). Therefore, we performed this meta-analysis to investigate whether XPC gene polymorphisms are associated with PCa.
Materials and Methods
Search strategy and identification of relevant studies
We conducted searches on PubMed, Excerpta Medica Database (EMBASE), Elsevier Science Direct, Cochrane Library, and China National Knowledge Infrastructure (CNKI) databases, last search updated on April 30, 2013, with the keywords “xeroderma pigmentosum complementation group C,” “XPC,” “prostate,” and “prostatic.” No language restrictions were applied. References of retrieved articles and review articles were also screened. When there were multiple articles from the same population, only the largest study was included. If an article reported results on different ethnicities or subpopulations, each ethnicity or subpopulation was treated as a separate study. Studies included in the meta-analysis had to meet all the following criteria: (1) evaluated the association between XPC gene polymorphisms and PCa; (2) used an unrelated case-control design; and (3) had available genotype frequency. The exclusion criteria were as follows: (1) did not have control; (2) did not have available genotype frequency; and (3) overlapping or republished studies.
Data extraction
For each publication, the data extraction was carried out by two investigators independently to ensure the accuracy of the data. In case of disagreement on any item of the data, the problem would be fully discussed to reach a consensus. The following information was recorded from each publication: the first author's name, year of publication, racial ancestry, source of publication, polymorphisms, tumor stage, bone metastasis, the number of cases and controls, and the available genotype and allele frequency information from XPC gene polymorphisms. If the original genotype frequency data were unavailable in relevant articles, a request for additional data was sent to the corresponding author.
Methods for quantitative synthesis
The strength of the association between XPC gene polymorphisms and PCa was measured by odds ratios (ORs) corresponding to 95% confidence intervals (CIs). Allele frequencies at XPC gene polymorphisms from the respective study were determined by the allele counting method. Hardy-Weinberg equilibrium (HWE) was tested by the chi-square test for goodness of fit. We examined the association between the allele, as well as genotype and PCa. The pooled OR was calculated for heterozygote comparison, homozygote comparison, dominant model, recessive model, and allele comparison, respectively. In addition, we performed stratified analyses by tumor stage (Gleason score: Gleason <7 and Gleason ≥7; pT: ≤T2 and >T2), bone metastasis (negative bone metastasis and positive bone metastasis), and ethnicity (Asians) when the data were available. For each analysis, we assessed the between-study heterogeneity across the comparisons using the chi-square test-based Q-statistic (Cochran, 1954), and a p-value of <0.10 was considered the presence of heterogeneity. We also used the statistic of I2 to efficiently test for the heterogeneity, with <25%, 25%-50%, and >50% to represent low, moderate, and high degree of heterogeneity, respectively (Higgins and Thompson, 2002). A random effect model (p<0.10) or a fixed effect model (p≥0.10) was used to pool the results (Mantel and Haenszel, 1959; DerSimonian and Laird, 1986). The pooled OR was determined by the Mantel-Haenszel method in the fixed effect model and by the DerSimonian and Laird method in the random effect model.
Evaluation of publication bias
Publication bias was investigated with the funnel plot, in which the standard error of ln(OR) of each study was plotted against its OR. An asymmetric plot suggests a possible publication bias. Funnel plot asymmetry was further assessed by the method of Egger's linear regression test (Egger et al., 1997). The significance of the intercept was determined by the t-test and a p-value of <0.05 was considered significant.
Analyses were conducted using Review Manager 4.2 software (Cochrane Collaboration) and Stata 10.0 software (Stata Corporation). A p-value less than 0.05 was considered statistically significant, and all the p-values were two sided.
Results
Study inclusion
Through literature search, 260 articles relevant to the searching keywords (PubMed: 10; EMBASE: 13; Elsevier Science Direct: 203; Cochrane Library: 1; CNKI: 33) were found. After careful screening, five articles examining the association between XPC gene polymorphisms and risk of PCa were found, as listed in Table 1 (Hirata et al., 2007; Agalliu et al., 2010; Liu et al., 2012; Mandal et al., 2012; Mittal and Mandal, 2012). Of the five articles, one was excluded due to it being a duplicate report (Mandal et al., 2012). Agalliu et al. (2010) provided data on two different ethnicities: Caucasian and African. Thus, each ethnicity was treated as a separate study in our meta-analysis. The study selection process is shown in Figure 1. Finally, a total of five separate studies (Hirata et al., 2007; Agalliu et al., 2010; Liu et al., 2012; Mittal and Mandal, 2012) were included in the current meta-analysis.
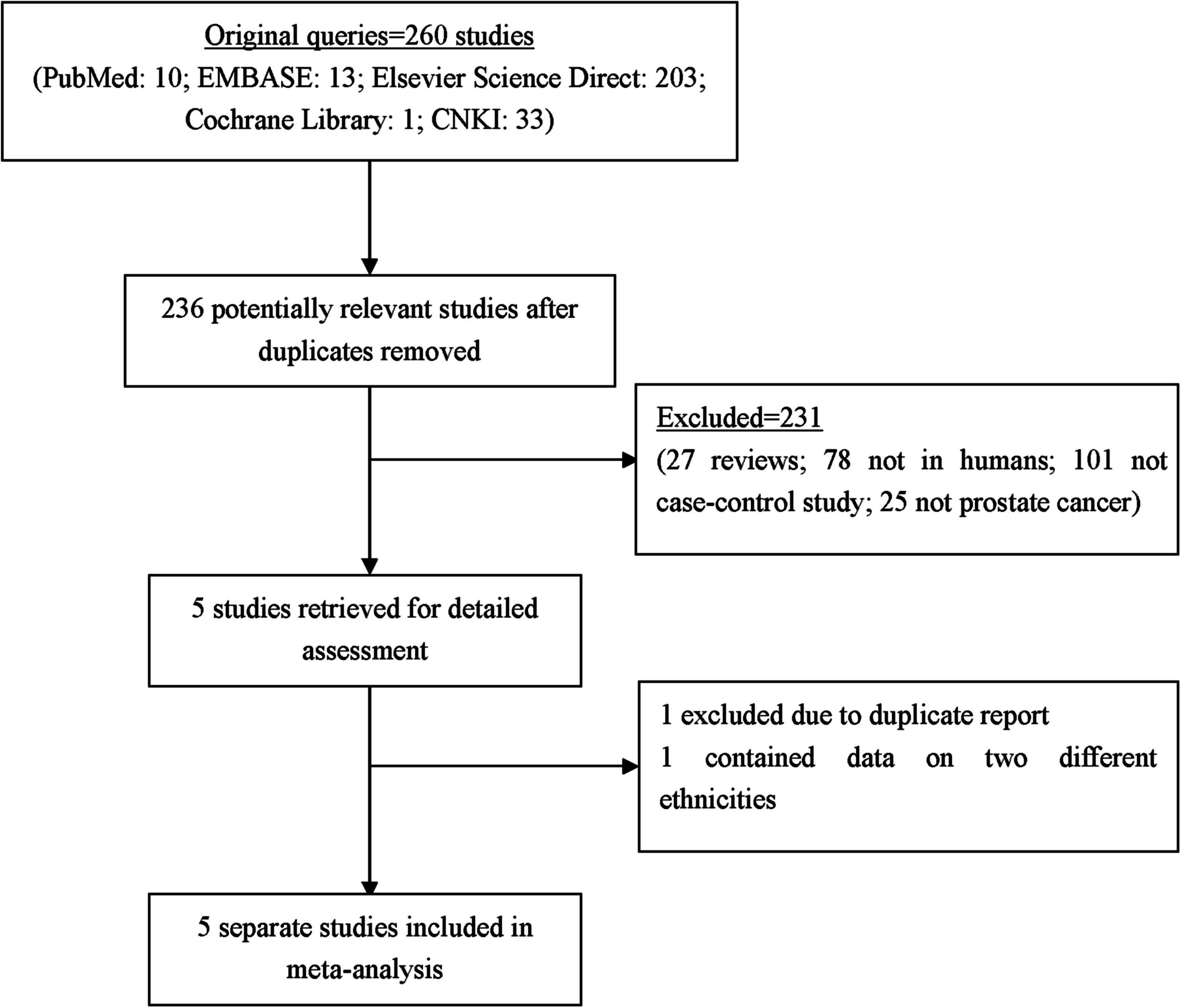
Flow diagram of the study selection process.
XPC, xeroderma pigmentosum complementation group C; HWE, Hardy-Weinberg equilibrium; C, conform.
The five separate studies assessed six polymorphisms in the XPC gene (rs2228001, PAT+/−, rs1126547, rs2733532, rs2733534, and rs8516). Two XPC gene polymorphisms [rs2228001 (Hirata et al., 2007; Agalliu et al., 2010; Liu et al., 2012; Mittal and Mandal, 2012) and PAT+/−(Liu et al., 2012; Mittal and Mandal, 2012)] were investigated in more than two studies. Meta-analysis was performed for the two polymorphisms. The distribution of the genotype in the control population was consistent with HWE in all the eligible studies (p>0.05). We performed meta-analysis in the overall population. Additionally, we performed stratified analyses by tumor stage [Gleason score: Gleason <7 and Gleason ≥7 (Hirata et al., 2007; Mittal and Mandal, 2012); pT: ≤T2 and >T2 (Hirata et al., 2007; Liu et al., 2012)], bone metastasis [negative bone metastasis and positive bone metastasis (Liu et al., 2012; Mittal and Mandal, 2012)], and ethnicity [Asians (Hirata et al., 2007; Liu et al., 2012; Mittal and Mandal, 2012)]. Whereas only the genotype frequency of the dominant model was extracted from the study by Hirata et al. (2007) when we performed stratified analyses by tumor stage.
Quantitative synthesis
The summary of meta-analysis for XPC gene polymorphisms with PCa is shown in Table 2.
R, random effect model; F, fixed effect model; OR, odds ratio; CI, confidence interval.
XPC rs2228001
Five separate studies, including 1966 cases and 1970 controls were eligible for the meta-analysis of XPC gene rs2228001 polymorphism. We detected significant between-study heterogeneity in the contrasts of CC versus AA+AC and CC versus AA. There was no evidence for a significant association between XPC gene rs2228001 polymorphism and PCa in the overall population (C vs. A: OR=1.05, 95%, CI=0.95-1.15, p=0.35; AC+CC vs. AA: OR=1.02, 95% CI=0.90-1.16, p=0.74; CC vs. AA+AC: OR=1.16, 95% CI=0.73-1.84, p=0.53; CC vs. AA: OR=1.14, 95% CI=0.72-1.82, p=0.57; AC vs. AA: OR=0.99, 95% CI=0.86-1.13, p=0.86). Subsequently, we performed stratified analyses by tumor stage (Gleason score: Gleason <7 and Gleason ≥7; pT: ≤T2 and >T2) and ethnicity (Asians). In the Asian population, significant between-study heterogeneity was found in the contrasts of C versus A, CC versus AA+AC, and CC versus AA. Similar results were observed in the Asian population (C vs. A: OR=1.08, 95% CI=0.80-1.45, p=0.61; AC+CC vs. AA: OR=1.06, 95% CI=0.84-1.33, p=0.63; CC vs. AA+AC: OR=1.20, 95% CI=0.46-3.11, p=0.72; CC vs. AA: OR=1.20, 95% CI=0.47-3.07, p=0.71; AC vs. AA: OR=1.00, 95% CI=0.78-1.27, p=0.97). We also did not detect a significant association between XPC gene rs2228001 polymorphism and tumor stage in PCa patients under the dominant genetic model (Gleason score: AC+CC vs. AA: OR=0.85, 95% CI=0.55-1.31, p=0.46, pheterogeneity=0.48; pT: AC+CC vs. AA: OR=1.18, 95% CI=0.77-1.80, p=0.44, pheterogeneity=0.68).
XPC PAT+/−
Two studies, including 397 cases and 471 controls were eligible for the meta-analysis of XPC gene PAT+/−polymorphism. The Q-test of heterogeneity was not significant and we conducted analyses using the fixed effect models. We detected a significant association of XPC gene PAT+/−polymorphism with PCa (+vs. −: OR=1.39, 95% CI=1.12-1.71, p=0.002;+/−and +/+ vs.−/−: OR=1.30, 95% CI=1.00-1.70, p=0.05;+/+vs.−/−and+/−: OR=2.07, 95% CI=1.33-3.23, p=0.001;+/+vs.−/−: OR=2.20, 95% CI=1.39-3.48, p=0.0008;+/−vs.−/−: OR=1.12, 95% CI=0.84-1.50, p=0.42). However, in subgroup analysis, we did not detect a significant association of XPC gene PAT+/−polymorphism with risk of bone metastasis in PCa patients (+vs.−: OR=1.34, 95% CI=0.71-2.52, p=0.37, pheterogeneity=0.04;+/−and+/+vs.−/−: OR=1.27, 95% CI=0.84-1.92, p=0.26, pheterogeneity= 0.16;+/+vs.−/−and+/−: OR=1.70, 95% CI=0.57-5.04, p=0.34, pheterogeneity=0.07;+/+vs.−/−: OR=1.79, 95% CI=0.52-6.14, p=0.36, pheterogeneity=0.05;+/−vs.−/−: OR=1.11, 95% CI=0.70-1.75, p=0.65, pheterogeneity=0.46).
Publication bias
A Funnel plot and Egger's linear regression test were performed to assess publication bias. For XPC gene rs2228001 polymorphism, the shapes of the funnel plots did not reveal any evidence of obvious asymmetry (funnel plots not shown), and these results were further supported by analysis using the Egger's linear regression test (C vs. A: t=− 0.09, p=0.936; AC+CC vs. AA: t =−0.42, p=0.703; CC vs. AA+AC: t=0.06, p=0.955; CC vs. AA: t=−0.01, p=0.995; AC vs. AA: t=−0.97, p=0.402). For the XPC gene PAT+/−polymorphism, the funnel plot and Egger's linear regression test were not applied due to the small number of studies.
Discussion
The current meta-analysis examined the association between two commonly studied XPC gene polymorphisms (rs2228001 and PAT+/−) and PCa risk. A total of 1,966 cases and 1,970 controls from five separate studies were included in the final analysis. We did not detect a significant association of XPC gene rs2228001 polymorphism with PCa. Similar results were found in stratification analyses by ethnicity and tumor stage. However, a significant association of XPC gene PAT+/−polymorphism with PCa was found. Subjects carrying the PAT+ allele exhibited a 1.39-fold increased risk associated with PCa in comparison to those with the PAT− allele. Subjects with PAT+/+genotype exhibited a 2.07-fold increased risk associated with PCa in comparison to those with PAT−/−and PAT+/−genotypes, and 2.20-fold increased risk associated with PCa in comparison to those with the PAT−/−genotype. Our results suggest that the PAT+ allele may be a low-penetrant risk factor for developing PCa. In addition, we did not find a significant association of PAT+/−polymorphism with risk of bone metastasis in PCa patients. As far as we know, this is the first comprehensive meta-analysis to investigate the association of XPC gene polymorphisms with PCa.
In the study, we detected a significant association of XPC gene PAT+/−polymorphism with PCa, and the PAT+ allele may be a low-penetrant risk factor for developing PCa. DNA repair capacity (DRC) plays a key role in genetic susceptibility to cancer. The XPC protein binds tightly with HR23B and forms the XPC-HR23B complex, which is involved in the DNA damage recognition and repair initiation in the NER pathway (Sugasawa et al., 1998; Thoma and Vasquez et al., 2003). Based on its functions in the NER pathway, XPC plays an important role in the repair of potential carcinogenic lesions. The PAT+/−polymorphism was located in the intron 9 of XPC gene, which involves deletion of five base pairs (bp) and insertion of an 83 bp AT repeat (Khan et al., 2000). In 2002, Qiao et al. (2002) investigated the association between the repair phenotype of ultraviolet (UV)-induced damage and genotypes of the XPC gene using a host cell reactivation assay. They found that healthy subjects with the homozygous variant genotype of the PAT polymorphism (+/+) exhibited lower DRC as compared to wild-type carriers (−/−), suggesting that the PAT+/+genotype maybe an adverse genotype on DRC. In 2004, in a hospital-based case-control study of 359 newly diagnosed lung cancer patients and 375 control subjects matched on age, sex, and catchment area, Marín et al. (2004) found that the PAT+/+subjects were at significantly increased risk for lung cancer, suggesting that XPC gene PAT+/−polymorphism may contribute to the risk of developing lung cancer. Thus, we speculate that XPC gene PAT+/−polymorphism might be associated with a lower DRC, resulting in an increased susceptibility to PCa. The detailed mechanisms need further study. In addition, the association may result from linkage disequilibrium with another functional polymorphism in the gene. The PAT+/−polymorphism has been reported to be in linkage disequilibrium with a new common C/A single-nucleotide polymorphism in intron 11 (IVS11-6) that was associated with increased skipping of exon 12 (Khan et al., 2002). The XPC splicing isoform without exon 12 had reduced the DNA repair activity and may contribute to PCa susceptibility. The PAT+/−polymorphism may not be a causal polymorphism, and the increased PCa susceptibility may arise from the linkage with IVS11-6 polymorphism. We did not detect a significant association of XPC gene rs2228001 polymorphism with PCa. Several pieces of evidence have shown that this polymorphism does not alter XPC function in vitro, which supports our results (Khan et al., 2000). Some studies have shown that the PAT+/−polymorphism maybe in linkage disequilibrium with rs2228001 polymorphism (Khan et al., 2002; Blankenburg et al., 2005; Sak et al., 2005). However, these studies were mainly conducted in the Caucasian population. In the current study, the studies that contributed data to the meta-analysis of PAT+/−polymorphism were mainly conducted in the Asian population. We speculate that the PAT+/−polymorphism maybe not in linkage disequilibrium with rs2228001 polymorphism in the Asian population. Further studies examining the linkage disequilibrium between the two polymorphisms are needed in the Asian population.
Meta-analysis remains a retrospective research that is subject to the methodological deficiencies of the included studies, and some limitations should be acknowledged. First, significant between-study heterogeneity was detected in some comparisons, and may be distorting the results. Second, our results are based on unadjusted estimates and a more precise analysis stratified by age, different lifestyle-related habits, and different subtypes of PCa could be performed if individual data were available. Third, for PAT+/−polymorphism, the funnel plot and Egger's linear regression test were not applied due to the small number of studies, which may affect the validity of the conclusion. Finally, given the limited number of studies in the meta-analysis, our results should be interpreted with caution.
In summary, the present meta-analysis provides new information on the association of XPC gene polymorphisms with PCa, and suggests that PAT+/−polymorphism, but not rs2228001, may contribute to the risk of developing PCa. To reach a definite conclusion, further studies based on a larger sample size, case-control design, and stratified by ethnicity are still needed.
Footnotes
Acknowledgments
We thank all the people who rendered help for this study. This work was supported by grants for Scientific Research of BSKY from the Anhui Medical University (XJ201110).
Author Disclosure Statement
No competing financial interests exist.