
Abstract
The association between excision repair cross complementing group 2 (ERCC2) Asp312Asn polymorphism and lung cancer has been reported by many articles recently, but the results were controversial and inconclusive. Therefore, a meta-analysis was conducted to assess the relationship between them. Pooled odds ratios (ORs) with 95% confidence intervals (CIs) were used to assess the strength of association. A total of 22 full studies with 20,101 subjects (8719 cases and 11,382 controls) were included in our research. The meta-analysis result showed that no significant association was found between ERCC2 Asp312Asn polymorphism and lung cancer in overall analysis (AA vs. GG, OR=1.023, 95% CI=0.824-1.270, p=0.838; AG vs. GG, OR=1.003, 95% CI=0.936-1.074, p=0.942; AA+AG vs. GG, OR=1.013, 95% CI=0.949-1.082, p=0.697; AA vs. AG+GG, OR=1.033, 95% CI=0.841-1.270, p=0.755). In subset analyses of stratified ethnicity, significantly increased risk was found among Asians (AA vs. GG, OR=3.212, 95% CI=1.518-6.795, p=0.002; AA vs. AG+GG, OR=3.174, 95% CI=1.500-6.712, p=0.003), whereas the association was not found among Caucasians under any genetic models. When analyses were conducted based on the study design, it indicated that the risk of lung cancer might be significantly increased in a hospital-based study (AA vs. GG, OR=1.323, 95% CI=1.096-1.596, p=0.004; AA+AG vs. GG, OR=1.109, 95% CI=1.000-1.229, p=0.050; AA vs. AG+GG, OR=1.285, 95% CI=1.076-1.535, p=0.006). In addition, a significantly increased risk for nonsmokers was detected under the dominant model (AA+AG vs. GG, OR=1.460, 95% CI=1.095-1.948, p=0.010). In conclusion, this meta-analysis suggested ERCC2 Asp312Asn polymorphism may increase the risk of lung cancer among Asians, whereas not among Caucasians.
Introduction
L
The excision repair cross complementing group 2 (ERCC2), also named Xeroderma pigmentosum group D (XPD), located on chromosome 19q13.3, consists of 23 exons and spans about 54,000 base pairs; it is an important DNA damage repair gene, which participates in the nucleotide excision repair (NER) pathway (Weber et al., 1990). The ERCC2 gene encoded is an integral member of the basal transcription factor BTF2/TFIIH complex and plays an important role in the transcription-coupled NER pathway by opening DNA around the damage by an ATP-dependent 5′-3′ DNA helicase for NER (Schaeffer et al., 1994). The high frequencies of Asp312Asn (rs1799793) in ERCC2 mutations have been identified in a protein coding region. G to A substitution in exon 10 might result in an amino acid alteration from aspartic (Asp) to asparagine (Asn). The G→A variation might be associated with a reduced repair capacity and facilitate cancer development (Benhamou and Sarasin, 2002).
Given the well-known enzyme activity of the ERCC2 Asp312Asn, Hemminki et al. (2001) reported that Asn/Asn carriers compared to the wild-type Asp/Asp carriers were 50% less efficient in DNA repair. And it has been shown that ERCC2 Asp312Asn polymorphism was associated with cancer, such as gastric cancer, prostate cancer, and breast cancer (Jiang et al., 2010; Liao et al., 2012; Yin et al., 2013). Most studies, including a recent meta-analysis, have investigated the ERCC2 Asp312Asn polymorphism and found that the polymorphism might be associated with lung cancer (Feng et al., 2012). However, the results were inconsistent and controversial. So, an updated meta-analysis with large samples needs to be conducted to clarify the relationship between ERCC2 Asp312Asn polymorphism and lung cancer.
Materials and Methods
Searching strategy and selection criteria
We searched eligible studies from Pubmed, Embase, and Medline until April, 2013 with the following terms: “Excision repair cross complementing group 2,” “ERCC2,” “Xeroderma pigmentosum group D,” “XPD,” “Asp312Asn,” “rs1799793,” “G23592A,” “polymorphism,” and “lung cancer.” The studies included in our meta-analysis were all written in English and conducted on human subjects. For overlapping or republished studies, we only selected the one with the most recent or the largest sample size. The eligibility criteria were as follows: (1) full-text studies; (2) case-control design; (3) the study estimating the risk of lung cancer for individuals carrying ERCC2 Asp312Asn polymorphism; (4) odds ratio (OR) and the corresponding 95% confidence interval (CI) were provided in each study; and (5) providing sufficient genotype data to investigate.
Data extraction
According to the above inclusion criteria, data were carefully extracted from all eligible studies independently by two investigators (X. Tan and Y.Y. Wang); disagreements were resolved by the third investigator (W.M. Chen). The following information was extracted from each study: first author's surname, year, country, ethnicity, source of controls, genotyping method, and the number of cases and controls, respectively.
Statistical analysis
The pooled OR and 95% CI were used to estimate the relationship between ERCC2 Asp312Asn polymorphism and lung cancer risk. We estimated the OR and 95% CI in the overall studies under several genetic models, including the allele contrast (A vs. G), homozygote comparison (AA vs. GG), heterozygote comparison (AG vs. GG), dominant model (AA+AG vs. GG), and recessive model (AA vs. AG+GG).
The chi-square test was used to test the Hardy-Weinberg equilibrium (HWE) in controls, and a p-value less than 0.05 was considered as significant deviation (Rohlfs and Weir, 2008). Chi-square-based Q statistic and p-value were used to assess the between-study heterogeneity. When p-value>0.1 and I2<25% indicated that no heterogeneity existed and values of about 50% indicated that heterogeneity was moderate, the fixed-effects model was performed using the Mantel-Haenszel's method. Otherwise, the random-effects model was performed by the DerSimonian and Laird method if I2>50% or p-value<0.1 (Yang et al., 2012).
The Begg's funnel plot and the Egger's linear regression test were used to test for potential publication bias; such publication bias probably exists (Peters et al., 2006) when the p-value is less than 0.05. To evaluate the effects of covariance, we performed subgroup analyses stratified by the ethnic subgroup (Asian and Caucasian) and control source (population based and hospital based). All analyses were carried out by the Stata software version 11.1 (Stata Corporation). All the p-values were two sided, less than 0.05 were considered statistically significant.
Results
Characteristics of relevant studies
Using our search strategy and inclusion criteria, 22 full studies (Butkiewicz et al., 2001; Spitz et al., 2001; Hou et al., 2002; Xing et al., 2002; Zhou et al., 2002; Liang et al., 2003; Misra et al., 2003; Popanda et al., 2004; Vogel et al., 2004; Shen et al., 2005; Hu et al., 2006; Matullo et al., 2006; Zienolddiny et al., 2006; De Ruyck et al., 2007; López-Cima et al., 2007; Yin et al., 2007; Chang et al., 2008; Raaschou-Nielsen et al., 2008; Yin et al., 2009; Qian et al., 2011; Sakoda et al., 2012; Zhou et al., 2012), including 23 individual studies with a total of 20,101 subjects (8719 cases, 11,382 controls) were included into this meta-analysis (Table 1). One study contains two ethnicity subgroups, and was divided into two individual studies (Chang et al., 2008). Therefore, in the analyses stratified by the ethnic subgroup, there were 13 studies on Caucasians, 8 studies on Asians (Table 1), and the remaining 2 studies were Latino-American and African-American, respectively. There were 15 population-based studies and 8 hospital-based studies (Table 1) in the source of control subgroup analysis. In addition, to investigate the effect of smoking on Asp312Asn polymorphism and lung cancer, only a few studies provided the smoking status and separated the raw data of genotype (Butkiewicz et al., 2001; Hou et al., 2002; Xing et al., 2002; Zhou et al., 2002; Misra et al., 2003; Yin et al., 2009; Zhou et al., 2012), which divided into the never-smokers group (Butkiewicz et al., 2001; Hou et al., 2002; Xing et al., 2002; Zhou et al., 2002; Yin et al., 2009) and the ever-smokers group (Butkiewicz et al., 2001; Hou et al., 2002; Xing et al., 2002; Zhou et al., 2002; Misra et al., 2003; Zhou et al., 2012).
For Hardy-Weinberg equilibrium in control group.
HB, hospital based; PB, population based; PCR, polymerase chain reaction; PCR-RFLP, polymerase chain reaction-restriction fragment length polymorphism; WGA, whole genome amplification.
Meta-analysis results
The detailed results of our meta-analysis on the relationship between ERCC2 Asp312Asn polymorphism and lung cancer risk are shown in Table 2. When the overall studies were pooled, the random-effects model was performed if the Q-test of heterogeneity was considered significant. In the case where the Q-test of heterogeneity was not significant, a fixed-effects model was constructed. In the overall pooled analysis, the results from random-effect models indicated that mutation allele (A) of ERCC2 Asp312Asn was not associated with lung cancer (A vs. G, OR=1.017, 95% CI=0.931-1.110, p=0.712). Moreover, there was no association between them under any assumed genetic models (AA vs. GG, OR=1.023, 95% CI=0.824-1.270, p=0.838; AG vs. GG, OR=1.003, 95% CI=0.936-1.074, p=0.942; AA+AG vs. GG, OR=1.013, 95% CI=0.949-1.082, p=0.697; AA vs. AG+GG, OR=1.033, 95% CI=0.841-1.270, p=0.755) (Table 2).
The pooled p-value.
p-Value for heterogeneity test.
Random-effects model.
Fixed-effects model.
OR, odds ratio; CI, confidence interval.
In the subgroup analysis based on ethnicity (Caucasians and Asians), no significant association was found between ERCC2 Asp312Asn polymorphism and lung cancer among the Caucasians (Table 2, Fig. 1). In contrast, our meta analysis result indicated that ERCC2 Asp312Asn polymorphism might increase the risk of lung cancer under two genetic models among Asians (AA vs. GG, OR=3.212, 95% CI=1.518-6.795, p=0.002; AA vs. AG+GG, OR=3.174, 95% CI=1.500-6.712, p=0.003) (Table 2, Fig. 2). Thus, individuals carrying the variant homozygote Asn/Asn might increase the susceptibility to lung cancer among the Asians.
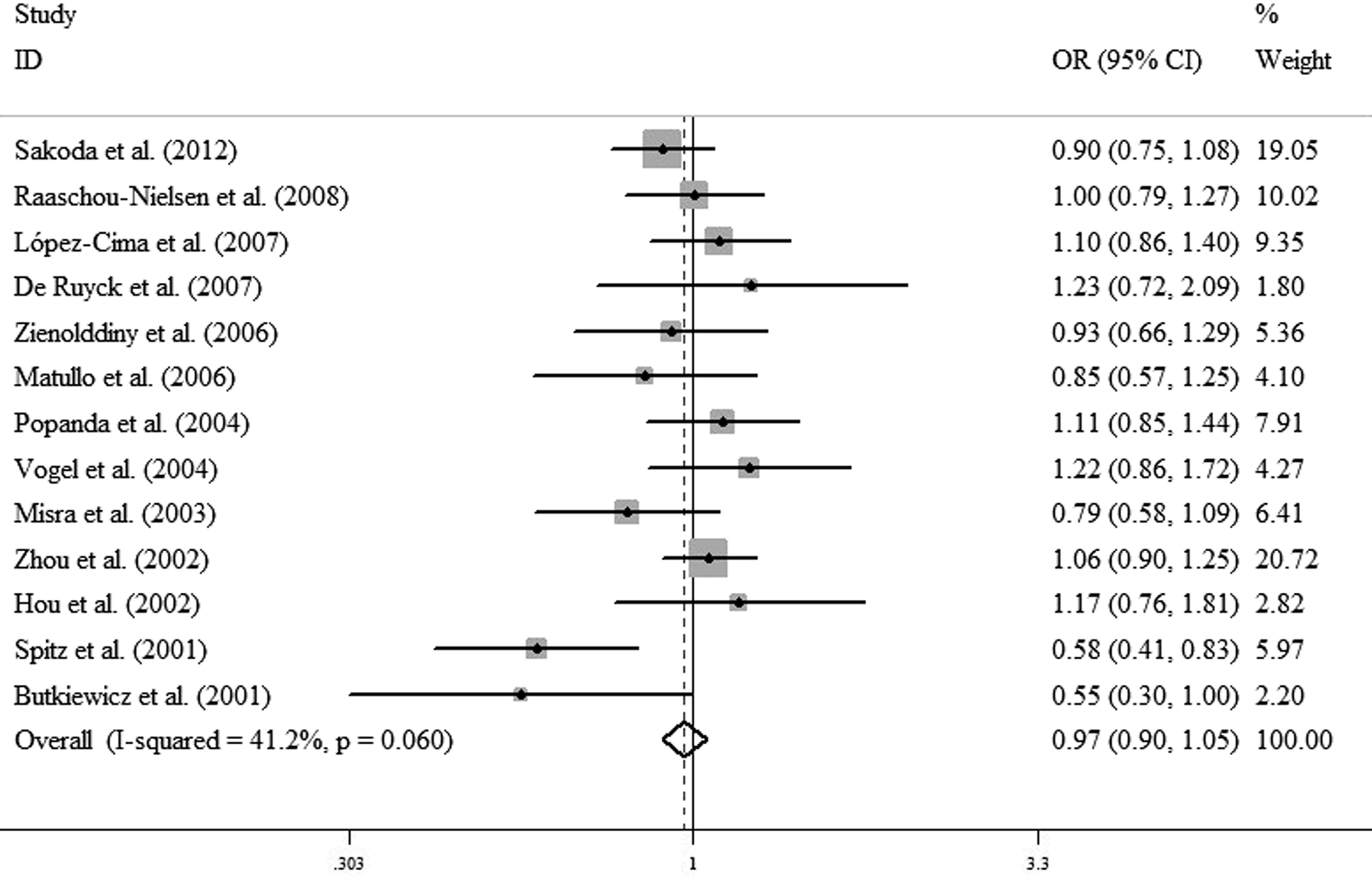
Forest plots for the excision repair cross complementing group 2 (ERCC2) Asp312Asn polymorphism and risk of lung cancer in the Caucasian group using the fixed-effect dominant model (AA+AG vs. GG).
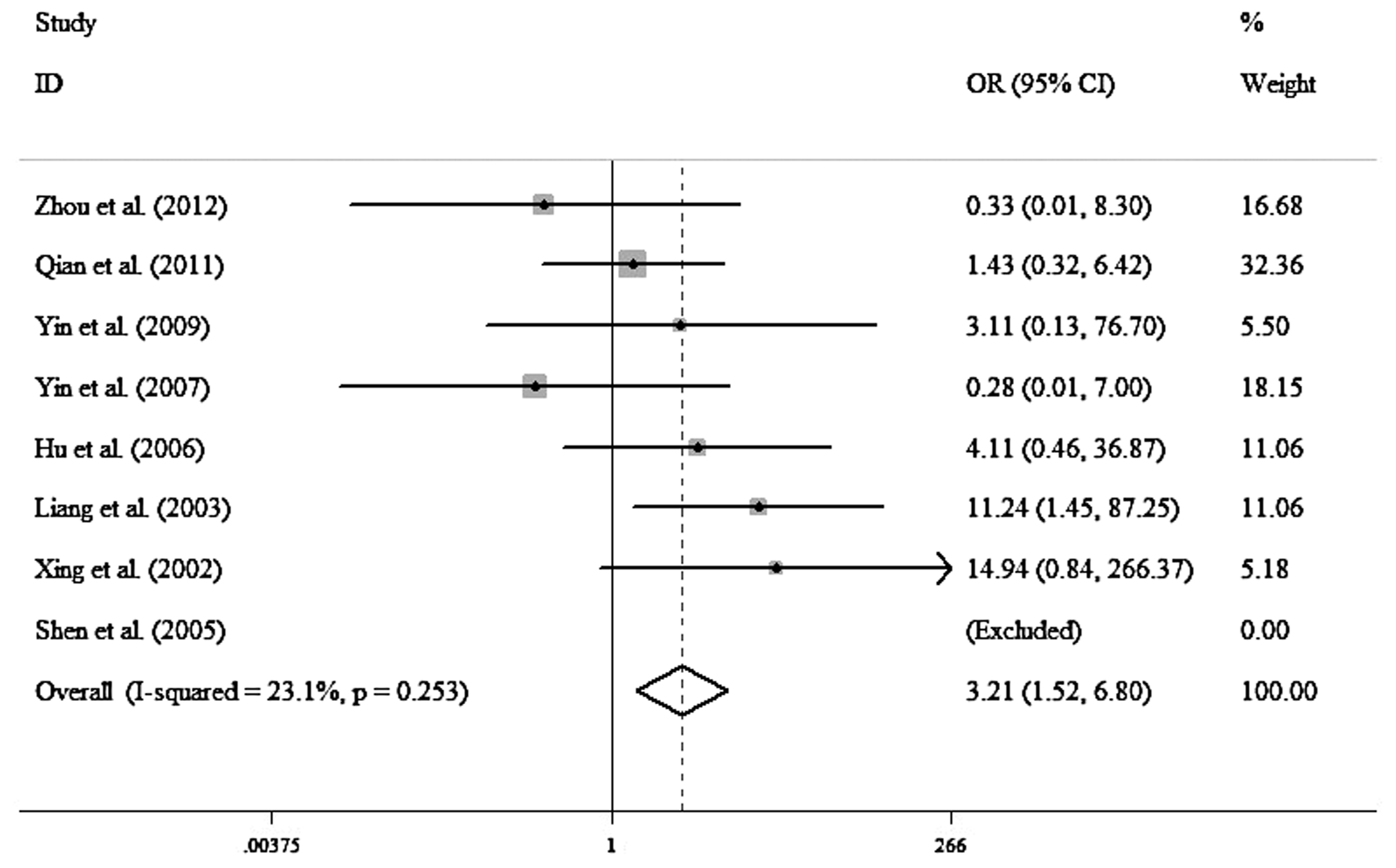
Forest plots for the ERCC2 Asp312Asn polymorphism and risk of lung cancer in the Asian group using the fixed-effect model (AA vs. GG).
When stratified by source of controls, the risk of lung cancer has been significantly elevated using hospital-based controls (AA vs. GG, OR=1.323, 95% CI=1.096-1.596, p=0.004; AA+AG vs. GG, OR=1.109, 95% CI=1.000-1.229, p=0.050; AA vs. AG+GG, OR=1.285, 95% CI=1.076-1.535, p=0.006) (Table 2, Fig. 3), whereas the increased risk was not found in a population-based group (Table 2).
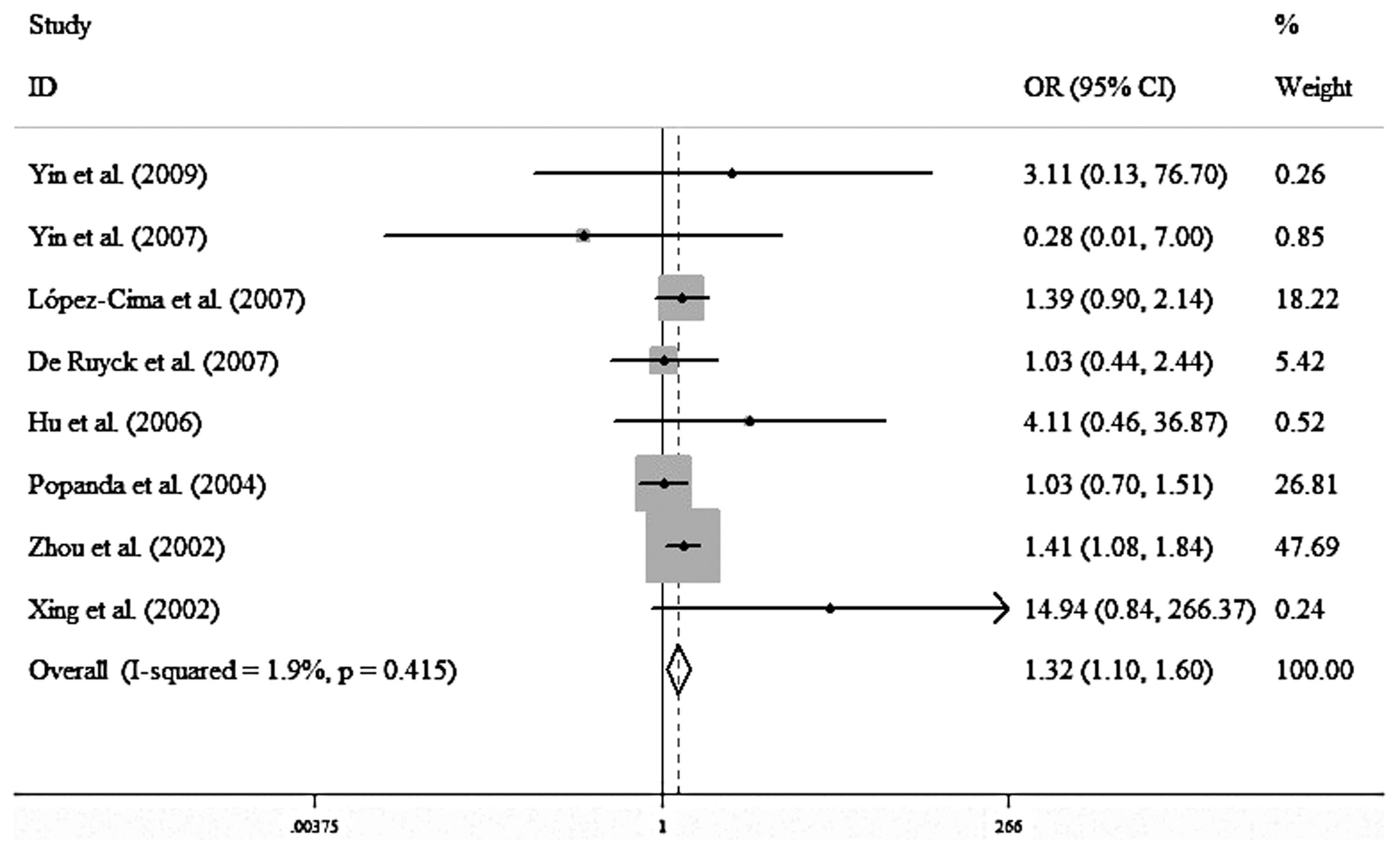
Forest plots for the ERCC2 Asp312Asn polymorphism and risk of lung cancer in the hospital-based group using the fixed-effect model (AA vs. GG).
Regarding the smoking effect on Asp312Asn polymorphism and lung cancer, it indicated that nonsmokers might have significantly increased lung cancer risk with Asp312Asn under the dominant model (AA+AG vs. GG, OR=1.460, 95% CI=1.095-1.948, p=0.010) (Fig. 4).
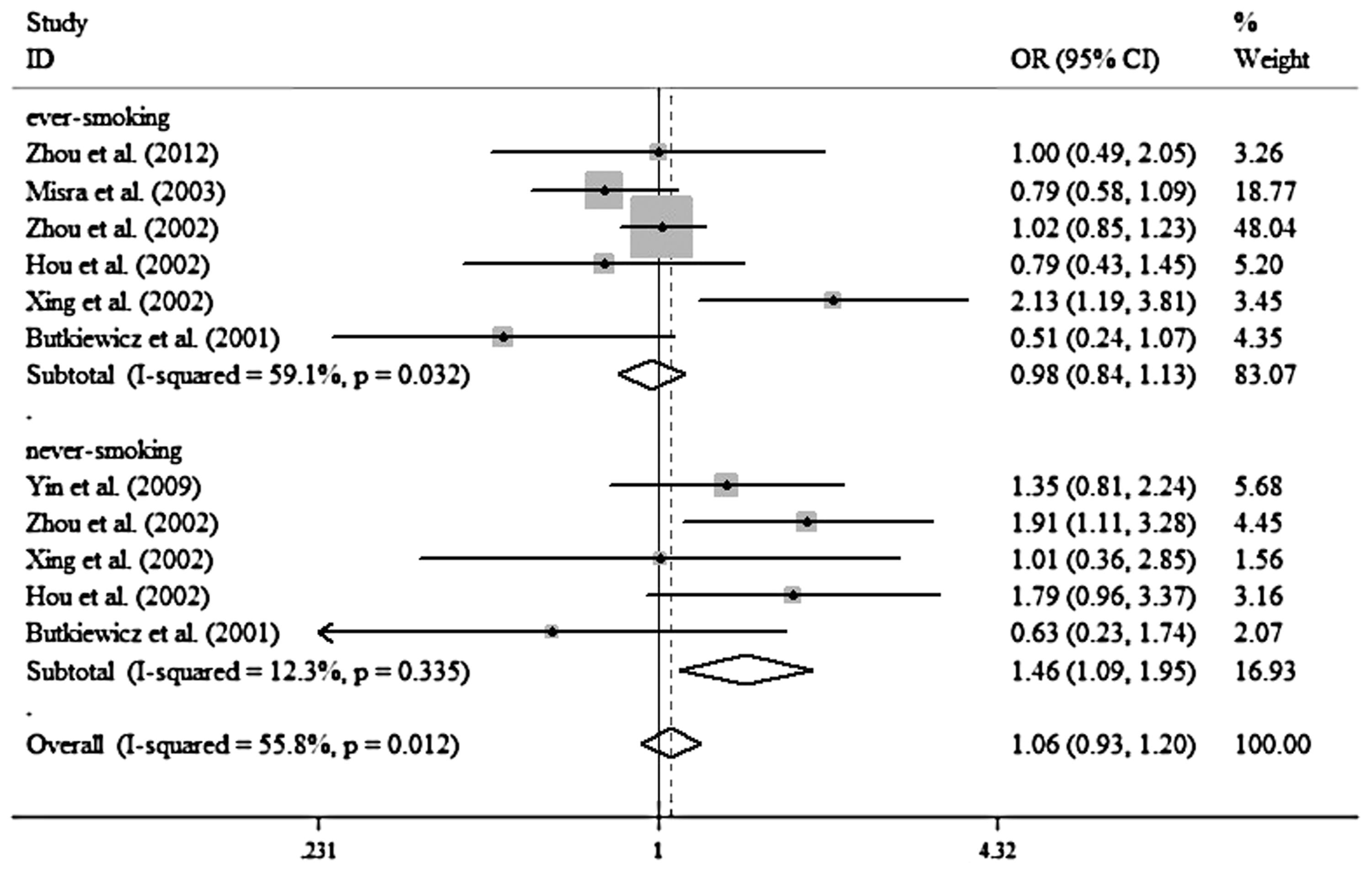
Forest plots for the ERCC2 Asp312Asn polymorphism and risk of lung cancer in the never-smoked group using the fixed-effect dominant model (AA+AG vs. GG).
Test for heterogeneity, sensitive analysis, and test for publication bias
Our results indicated that heterogeneity was present in the overall pooled analysis; when we performed stratified analysis, the heterogeneity was substantially reduced in the Asians and the hospital-based group, whereas it was not significantly decreased in the Caucasians and the population-based group. HWE was estimated for each study's controls (p>0.05). There were three studies that deviated from HWE in our meta-analysis. Therefore, sensitivity analysis was performed in our meta-analysis. When we dropped one study at each time, the results remained stable, which indicated that our meta-analysis results were robust and reliable (data not shown).
Potential publication bias was estimated by the Begg's funnel plot and the Egger's test. Both the Begg's funnel plot and Egger's test indicated that there was no evidence of publication bias in the overall pooled studies (AA vs. GG Begg's test, p=0.596, Egger's test, p=0.773; AG vs. GG Begg's test, p=0.463, Egger's test, p=0.753; dominant model, Begg's test, p=0.833, Egger's test, p=0.868; recessive model, Begg's test, p=0.596, Egger's test, p=0.813).
Discussion
DNA alterations in a single cell or a clone of a cell may lead to the malfunction of a cell, which could result in cancer. The NER pathway was one of the most significant versatile systems to repair a wide variety of DNA lesions, including crosslinks, UV-induced photoproducts, bulky adducts, oxidative damage, and so on (Zhang et al., 2011). The ERCC2 gene played an important role in the NER pathway. Hu et al. (2006) reported that a fivefold variation in DNA repair capacity (DRC) has been detected in the general population and the decreased DRC may increase the risk of lung cancer. Spitz et al. (2001) reported that DRC had the interindividual variability, and the ability to repair BPDE-induced adducts was a significant predictor of lung cancer risk in peripheral lymphocytes. However, how ERCC2 Asp312Asn polymorphism affects lung cancer risk in the molecular mechanisms remained unclear. Butkiewicz et al. (2001) reported that the Asn allele might be a protective effect when compared with the Asp/Asp genotype using 96 lung cancer cases. However, Xing et al. (2002) indicated that at least one 312Asn variant allele had an increased risk of lung cancer. Raaschou-Nielsen et al. (2008) have demonstrated that the ERCC2 Asp312Asn polymorphism had no significant association with the risk for lung cancer. Recently, several meta-analyses investigated the association between ERCC2 Asp312Asn polymorphism and the risk of lung cancer (Benhamou and Sarasin, 2005; Manuguerra et al., 2006; Kiyohara and Yoshimasu, 2007; Wang et al., 2008; Vineis et al., 2009; Zhang et al., 2011; Feng et al., 2012). A recent meta-analysis has suggested that the ERCC2 312Asn variant allele significantly increased lung cancer risk, and the relationship held in both Caucasians and Asians (Feng et al., 2012). However, the results were still controversial and inconclusive.
To further investigate the association between ERCC2 Asp312Asn polymorphism and lung cancer, our meta-analysis included more new studies with a larger sample size. Our meta-analysis showed that there was no significant association between ERCC2 Asp312Asn polymorphism and lung cancer in the overall analysis, which was consistent with the Kiyohara and Yoshimasu (2007) report. However, our results were different from that of Feng et al. (2012) and Zhang et al. (2011). No publication bias was found using the Begg's and Egger's test, which demonstrated that the conclusion drawn from our meta-analysis was reliable.
In subgroup analyses, ERCC2 Asp312Asn polymorphism was significantly associated with susceptibility to the development of lung cancer among the Asians. However, the association was not held among the Caucasians. Feng et al. (2012) and Zhang et al. (2011) have shown the similar results among the Asians but not Caucasians. There are several potential reasons to explain this. First, the genetic polymorphisms are distributed differently among different ethnicity groups. Second, lifestyles and eating habits may also differ in different ethnicity groups. It is worth noting that people with different ancestry may also have a different smoking habit. Furthermore, the gene-environmental interaction might be another significant factor. Finally, the sample size in our present research might be relatively small, and large-scale studies would be necessary to investigate their relationship. It is noteworthy that the Asian subjects included in our meta-analysis were all Chinese, and it indicated that the significant association between ERCC2 Asp312Asn polymorphism and lung cancer was held in the Chinese population. In all, individuals carrying the variant homozygote Asn/Asn of the ERCC2 Asp312Asn might be a risk factor for lung cancer in Asians.
When in the subgroup analyses stratified based on the population and hospital, no significant association was detected between ERCC2 Asp312Asn polymorphism and lung cancer in the population-based group. It revealed that variant Asn of ERCC2 Asp312Asn increased the susceptibility to lung cancer in the hospital-based group. The source of hospital-based people might be associated with other diseases, particularly the genotypes investigated in the controls, which might lead to some biases for our result. So the results should be interpreted with caution. It has been known that smoking is the strongest risk factor for lung cancer, when subgroup analysis stratified by smoking status, nonsmokers with the variant genotype 312Asn compared with wild-type Asp/Asp might be at risk for lung cancer, whereas this finding was not detected in ever-smokers. Previous studies showed similar results for the gene-smoking interaction, which was in accord with our results (Feng et al., 2012). Different individuals with the NER capacity leading to NER gene polymorphisms may not be the main susceptibility to tobacco smoke for developing lung cancer (Raaschou-Nielsen et al., 2008).
Despite having made great efforts to collect all possible data for comprehensive analysis, some limitations in our meta-analysis should be acknowledged. First, although 20,101 subjects were included in our study, the sample sizes were relatively small in the stratified analyses. There was not enough power to investigate the true relationship. Second, our data lacked detailed adjustment, such as age, sex, smoking status, and lifestyle. In particular, the source of control was not uniformly defined, which might be a source of heterogeneity. Finally, although the Begg's and Egger's test did not indicate any publication bias in our research, all studies included in our research were written in English and excluded unpublished articles and abstracts, which might lead to publication bias. In spite of this, our research was more powerful than any single study.
In summary, our research indicates that ERCC2 Asp312Asn polymorphism may increase lung cancer risk in the Asians, especially in the Chinese. The finding does not hold in the Caucasians. Due to the incompleteness of raw data, gene-gene and gene-environmental interactions leading to lung cancer have not been thoroughly investigated. Therefore, a large-sample and well-designed case-control study is needed to investigate the relationship between ERCC2 polymorphism and lung cancer.
Footnotes
Author Disclosure Statement
All the authors of this manuscript have no conflicts of interest.