
Abstract
Aims: The present study was undertaken to determine the association between −1562C>T polymorphism in the promoter region of matrix metalloproteinase-9 (MMP-9) and coronary artery disease (CAD) risk. Methods: This meta-analysis was on the basis of 26 studies that included 12,776 cases and 6371 controls, heterogeneity of which was assessed by the Q-statistic test and the I2-statistic test. Sensitivity analysis was conducted by sequentially omitting any single study and recalculating the odds ratios (ORs) and 95% confidence intervals (CIs). Funnel plots and Egger's test were performed to test the potential publication bias. All data were analyzed by using STATA version 12.0. Results: We found that −1562C>T polymorphism did not contribute to the risk of CAD in the overall results. But the stratified analysis by ethnicity indicated that −1562C>T polymorphism might decrease susceptibility to CAD in Asians (OR, 0.94; 95% CI, 0.88-1.00; ph=0.956 for CC vs. CT+TT). Conclusions: Our meta-analysis supports the fact that −1562C>T polymorphism may have association with CAD risk in Asian populations. But further larger studies are required to confirm our findings.
Introduction
C
The potential candidate gene MMP-9, also known as gelatinase B or 92-kDa type IV collagenase, is a member of the MMP family that plays a key role in the development of atherosclerotic cardiovascular diseases (Galis et al., 1994). Since MMP-9 has broad substrate specificity and distal position in the matrix proteolytic cascade, it would cause extracellular matrix degradation and subsequent rupture of atherosclerotic plaques. This facilitates cell migration into the intima after an arterial injury (Newby et al., 1994; Pauly et al., 1994; Brown et al., 1995). There are many polymorphisms in the promoter, coding, and untranslated regions of the MMP-9 gene (Yasmin et al., 2006), of which the −1562C>T polymorphism has attracted great attention from many investigators.
Despite an increasing body of studies concerning −1562C>T polymorphism and CAD risk, their findings remain uncertain (Wang et al., 2001; Cho et al., 2002; Morgan et al., 2003; Chen et al., 2005; Haberbosch et al., 2005; Tang et al., 2005; Meng et al., 2006; Nuzzo et al., 2006; Chen et al., 2007b; Horne et al., 2007; Nanni et al., 2007; Wang et al., 2007; Koh et al., 2008; Alp et al., 2009; Wu et al., 2009; Fallah et al., 2010; Gao and Wang, 2010; Ghaderian et al., 2010; Ma, 2010; Yong, 2010; Zhang et al., 2010; Zhi et al., 2010; Han et al., 2012; Opstad et al., 2012; Spurthi et al., 2012; Wang et al., 2012). For example, Morgan et al. demonstrated that −1562C>T polymorphism influences the development and progression of CAD (Morgan et al., 2003), while Haberbosch et al. (2005) supported the notion that this polymorphism is not a risk factor. This is probably because the single studies differ in sample sizes and study designs, which could be avoided through meta-analysis. Therefore, we performed a comprehensive meta-analysis with sufficient statistical power to assess whether there was relationship between −1562C>T polymorphism and the risk of CAD.
Materials and Methods
Search strategy
We searched the databases of the PubMed, EMBASE, and CNKI for eligible studies regarding the association of −1562C>T polymorphism and CAD risk published before January 2013 with a limit to human subjects. The search was performed by using the following key phrases: “matrix metalloproteinase,” “matrix metalloproteinase-9,” or “MMP-9”; “−1562C>T” or “rs3918242”; “coronary artery disease” or “CAD”; and “coronary heart disease” or “CHD.” The additional relevant publications were identified by manually searching the review articles and the references of the retrieved studies.
Inclusion criteria
The inclusion criteria for literature selection were as follows: (1) on the basis of a case-control study, (2) investigating the association of −1562C>T polymorphism and CAD risk, (3) providing sample sizes in cases and controls, and (4) having available data to retrieve the numbers of the genotypes. But reviews, editorials, and articles with insufficient information were excluded. In terms of the studies with overlapping data, the most recent one or the one with the larger sample was selected.
Data extraction
Strictly complying with the inclusion criteria, two investigators (Fengxiang Zhang and Dapeng Sun) independently extracted the data from all eligible publications. The extracted information included the first author, year of publication, study country, origin of the subjects, genotyping methods, sample sizes in the cases and controls, and the genotype distribution. The disagreements were resolved by discussion among the authors.
Statistical analysis
The strength of the association between −1562C>T polymorphism and CAD risk was evaluated by pooled odds ratios (ORs) with corresponding 95% confidence intervals (CIs). The summary ORs were calculated for CC versus TT, CC+CT versus TT, CC versus CT+TT, allele C versus allele T, and CT versus TT, respectively. Subgroup analyses by ethnicity and source of control were also conducted to further determine the relationship of −1562C>T polymorphism and CAD susceptibility. The between-study heterogeneity of the included studies in this meta-analysis was assessed by the Q-statistic test and the I2-statistic test. p<0.1 and I2>50% indicated significant evidence of heterogeneity (Cochran, 1950; Higgins et al., 2003). If p>0.1 and I2<50%, then the fixed-effect model was applied by the Mantel-Haenszel's method (Mantel and Haenszel, 1959); otherwise, the random-effect model was adopted by the DerSimonian and Laird's method (DerSimonian and Laird, 1986). To identify the source of between-study heterogeneity, we conducted subgroup analyses and meta-regression (Thompson and Higgins, 2002). Hardy-Weinberg equilibrium (HWE) for the genotype distribution of −1562C>T polymorphism in the controls was tested to estimate the quality of the included studies (Salanti et al., 2005). Sensitivity analysis was performed by sequentially omitting any single study and recalculating the ORs and 95% CIs to examine the stability and credibility of the results. Funnel plots and Egger's test were performed to test the potential publication bias (Egger et al., 1997; Stuck et al., 1998). All data were analyzed by using STATA version 12.0 (Stata Corporation, College Station, TX). p<0.1 was deemed statistically significant.
Results
Characteristics of eligible studies
We initially extracted a total of 37 articles according to the predescribed selection criteria. Having been further examined the full tests, 11 of them were excluded, for 5 failed to provide definite numbers of the genotypes (Zhang et al., 1999; Kim et al., 2002; Blankenberg et al., 2003; Medley et al., 2004; Liu et al., 2012), 2 were updated by a subsequent study included in the current meta-analysis (Chen et al., 2007a), 2 were based on case-only design (Pollanen et al., 2001; Saedi et al., 2012), and 2 were review articles (Abilleira et al., 2006; Niu and Qi, 2012). At last, 26 studies with 12,776 cases and 6371 controls were available for the meta-analysis. The sample size of the available studies ranged from 130 to 3801. The ethnic subgroups consisted of 8663 Caucasians and 10,484 Asians. In addition, the majority of the studies eligible for this meta-analysis were based on hospital controls. The main information of the included studies is listed in Table 1.
CA, Caucasian; A, Asian; HB, hospital-based; PB, population-based; NM, not mentioned; PCR-RFLP, PCR-restriction fragment length polymorphism; TaqMan, TaqManSNP; HWE, Hardy-Weinberg equilibrium.
Meta-analysis results
The principal results of this meta-analysis are displayed in Table 2. In general, no evidence for statistically significant association was found between −1562C>T polymorphism and CAD risk under all contrast models. However, in the stratified analyses by ethnicity, we observed a protective effect under the CC versus CT+TT genetic model in Asian populations (OR, 0.94; 95% CI, 0.88-1.00; ph=0.956) (Figs. 1 and 2). Similarly, when stratifying the subgroups by source of control, we found a borderline association under the contrast model of CC versus CT+TT in hospital-based studies (OR, 0.94; 95% CI, 0.88-1.00; ph=1.000).

Forest plot of estimates of the ORs for −1562C>T polymorphism in coronary artery disease (CAD) under CC versus TT. The squares and horizontal lines correspond to odds ratios (ORs) and 95% confidence intervals (CIs) of specific study, and the area of squares reflects study weight (inverse of the variance). The diamond represents the pooled ORs and its 95% CIs.
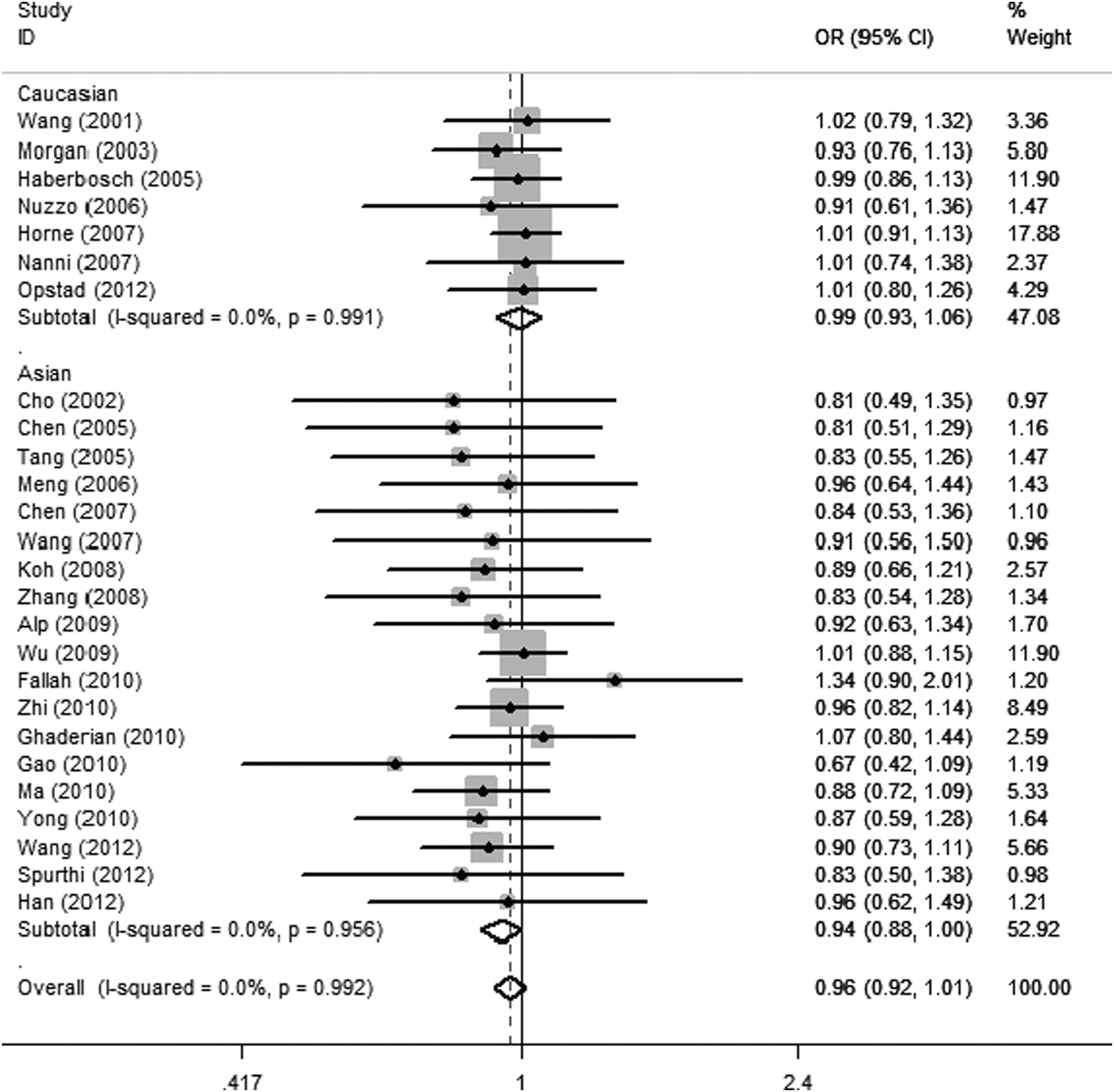
Forest plot of estimates of the ORs for −1562C>T polymorphism in CAD under CC versus CT+TT. The squares and horizontal lines correspond to ORs and 95% CIs of specific study, and the area of squares reflects study weight (inverse of the variance). The diamond represents the pooled ORs and its 95% CIs.
ph, p-value of heterogeneity test; OR, odds ratio; CI, confidence interval.
Heterogeneity analysis
There was no observed between-study heterogeneity in the included studies (p>0.1). Therefore, the fixed-effect model was applied for the pooled analyses to assess the association between −1562C>T polymorphism and CAD susceptibility.
Sensitivity analysis
Sensitivity analysis was performed via sequentially excluding each single study, one at a time and recalculating the ORs and 95% CIs to detect the credibility and stability of our results. The sensitivity analysis suggested that no single study changed the pooled ORs qualitatively (data not shown).
Publication bias
Funnel plot and Egger's test were conducted to access the publication bias of all studies. The symmetrical shape of the funnel plots indicated that there existed no evident publication bias (Fig. 3). Moreover, no obvious evidence was observed in Egger's test, suggesting that there was no significant publication bias in this meta-analysis (CC vs. CT+TT: p=0.450).
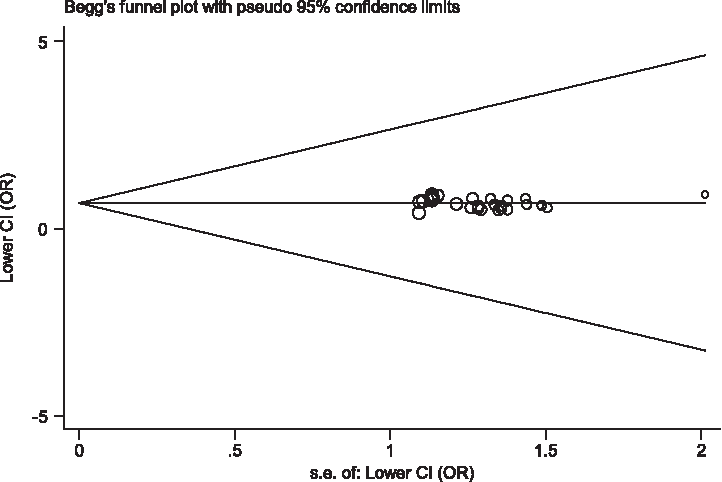
Funnel plot for publication-bias test (CC vs. CT+TT).
Discussion
The MMP-9 gene is located on chromosome 20. Overexpression and increased circulation level of this protein have been reported to be correlated with CAD in previously published studies (Brown et al., 1995; Yasmin et al., 2005). Recently, a large number of individual studies have paid much attention to the effects of the functional −1562C>T polymorphism of the MMP-9 gene on CAD susceptibility, yet the findings remain inconclusive and inconsistent. Of them, seven studies demonstrated that the functional 1562C>T polymorphism is not a risk contributor to CAD susceptibility (Wang et al., 2001; Haberbosch et al., 2005; Nuzzo et al., 2006; Alp et al., 2009; Wu et al., 2009; Han et al., 2012; Opstad et al., 2012). Conversely, as many as 24 single publications indicated a different finding (Cho et al., 2002; Morgan et al., 2003; Chen et al., 2005; Tang et al., 2005; Meng et al., 2006; Chen et al., 2007b; Horne et al., 2007; Nanni et al., 2007; Wang et al., 2007; Koh et al., 2008; Fallah et al., 2010; Gao and Wang, 2010; Ghaderian et al., 2010; Ma, 2010; Yong, 2010; Zhang et al., 2010; Zhi et al., 2010; Wang et al., 2011; Spurthi et al., 2012; Wang et al., 2012; Li et al., 2013). There are possible explanations for this discordance, such as small sample sizes, incorrect multiple hypothesis testing, and potential publication bias.
In addition, two meta-analyses were carried out in 2011 (Wang et al., 2011) and 2013 (Li et al., 2013) separately, supporting the fact that the MMP9-1562C>T polymorphism is a risk factor for CAD susceptibility. As compared with the former two meta-analyses of the association of MMP9-1562C/T polymorphism and CAD risk, our study showed that −1562C>T polymorphism did not have statistically significant association with the susceptibility to CAD. Our meta-analysis is superior to the others, due to the far larger number of participants (26 included studies with 12,776 cases and 6371 controls) compared with the study by Li et al. (2013) (12 included studies with 8281 cases and 3940 control) and with the study by Wang et al. (2011) (seven included studies with 4473 cases and 3343 controls). The substantially large sample size ensures the reliability of the results, despite no relationship indicated in the analysis.
Wang et al. (2011) have identified that −1562C>T polymorphism plays different roles in different ethnic populations; thus, subgroup analysis by ethnicity was carried out. The analysis indicated supportive evidence for correlation between the polymorphism of −1562C>T and the risk of CAD in Asian populations rather than Caucasian populations. It is likely that genetic background plays a crucial role in the susceptibility to CAD.
Moreover, the CC versus CT+TT genetic model was implicated to be potentially associated with CAD risk in the hospital-based studies. The included studies had different criteria when selecting their control subjects. Some control groups may not be representative of the general population, leading to the occurrence of selection bias.
Several limitations in this meta-analysis need to be pointed out. One limitation is that our study only investigated one single-gene polymorphism, which would have less power to completely interpret the genetic risk for CAD. Because CAD is a multifactorial disease caused by genetic and environmental factors. Another limitation refers to the potentially unobservable heterogeneity in our study. In the subgroup analyses by ethnicity and source of control, we did not find any significant heterogeneity in the distribution of the genotypes of −1562C>T polymorphism. The insignificant heterogeneity should be further confirmed by stratified analysis by other unmeasured characteristics.
To sum up, the current meta-analysis provided evidence that −1562C>T polymorphism may have modification effects on CAD susceptibility in Asians. Future studies with more genetic polymorphisms and better study designs are necessary to confirm our current findings, which might provide more insights into the pathogenesis and targeted prevention of CAD.
Footnotes
Acknowledgments
This work was supported by Natural Science Foundation of Liaoning Province (2013022010); Youth Science Foundation of Liaoning Medical University (Y2012Z011); Youth Science Foundation of The First Hospital of Liaoning Medical University (FY2012-17).
Author Disclosure Statement
No competing financial interests exist.