
Abstract
Background: Interleukin-6 (IL-6) plays a critical role in the development and progression of cardiovascular disease. Emerging evidence suggests that two common polymorphisms (−174 G/C and −572 G/C) in the IL-6 gene might have an impact on an individual's susceptibility to myocardial infarction (MI), but individually published results are inconclusive. This meta-analysis aimed to derive a more precise estimation of the relationship between IL-6 −174 G/C and −572 G/C polymorphisms and MI risk. Method: An extensive literary search for relevant studies was conducted in PubMed, Embase, Web of Science, Cochrane Library, CISCOM, CINAHL, Google Scholar, China BioMedicine (CBM), and China National Knowledge Infrastructure (CNKI) databases from their inception through August 1st, 2013. A meta-analysis was then performed using the STATA 12.0 software. The crude odds ratios (OR) with 95% confidence intervals (CI) were calculated. Results: Eleven case-control studies were included with a total of 10,252 subjects, including 5429 MI patients and 4823 healthy controls. Our meta-analysis results indicated that IL-6 −174 G/C polymorphism may increase the risk of MI (C allele vs. G allele: OR=1.07, 95% CI: 1.01-1.14, p=0.018; GC+CC vs. GG: OR=1.14, 95% CI: 1.04-1.24, p=0.003; respectively). However, our results showed no significant association between IL-6 −572 G/C polymorphism and MI risk (C allele vs. G allele: OR=0.88, 95% CI: 0.75-1.03, p=0.098; GC+CC vs. GG: OR=0.87, 95% CI: 0.70-1.07, p=0.173; respectively). No publication bias was detected in this meta-analysis. Conclusion: The current meta-analysis suggests that IL-6 −174 G/C polymorphism may contribute to MI susceptibility. Thus, detection of IL-6 −174 G/C polymorphisms may be a promising biomarker for the early detection of MI. However, IL-6 −572 G/C polymorphism may not associate with the risk of MI.
Introduction
M
Interleukin-6 (IL-6) receptor, a member of the cytokine receptor family, which functions in the regulation of the immune response, hematopoiesis, and inflammation, plays an important role in thrombosis formulation by activating the coagulation process (Sims and Smith, 2010; Hansson and Hermansson, 2011; Turpie and Esmon, 2011). The human IL-6 gene is located on human chromosome7p21, contains five exons and four introns, and spans ∼5 kb (Brocker et al., 2010). IL-6 can produce myocyte hypertrophy, myocardial dysfunction, and on the other hand, it may block cardiac myocyte apoptosis (Anker and von Haehling, 2004). Generally, the IL-6 gene is implicated in MI susceptibility by stimulating the synthesis of a tissue factor from monocytes and endothelial cells, which triggers activation of the coagulation cascade toward thrombus formation (Iacoviello et al., 2005). Therefore, it is hypothesized that IL-6 gene polymorphisms might modulate the inflammation-triggered pathway of thrombus formation and the risk of MI (Pierre-Paul and Gahtan, 2003).
Recently, several single-nucleotide polymorphisms (SNPs) in the IL-6 gene have been identified as candidates for MI susceptibility. Among them, −174 G/C and −572 G/C are the most common variants that have been widely investigated (Georges et al., 2001). Most of previous studies support the mechanism in which IL-6 −174 G/C and −572 G/C polymorphisms promote the development of MI (Fu et al., 2006; Vakili et al., 2011). However, there are also some studies suggesting that there exists no association between the IL-6 −174 G/C and −572 G/C polymorphisms and their effects on susceptibility to MI (Nauck et al., 2002; Kelberman et al., 2004). Therefore, we performed a meta-analysis of all eligible case-control studies to reveal a more precise relationship between IL-6 −174 G/C and −572 G/C polymorphisms and MI risk.
Materials and Methods
Literature search strategy
A comprehensive search for relevant studies published before August 1st, 2013 was conducted on PubMed, Embase, Web of Science, Cochrane Library, CISCOM, CINAHL, Google Scholar, China BioMedicine (CBM), and China National Knowledge Infrastructure (CNKI) databases without language restrictions. We used the following keywords and MeSH terms: (“genetic polymorphism” or “polymorphism” or “SNP” or “single nucleotide polymorphism” or “gene mutation” or “genetic variants”) and (“myocardial infarction” or “myocardial infarct” or “MI” or “AMI”) and (“interleukin-6” or “IL-6” or “IL6” or “IFN beta 2” or “B cell differentiation factor 2”). The references used in eligible articles or textbooks were also reviewed to find other potential studies.
Inclusion and exclusion criteria
Studies included in our meta-analysis have to meet the following criteria: (1) clinical case-control studies focused on the association between IL-6 −174 G/C and −572 G/C polymorphisms and MI risk; (2) all patients should meet the diagnostic criteria for MI; (3) the minimum number of cases in included studies should be greater than 30; (4) the genotype distribution of the controls should conform to the Hardy-Weinberg equilibrium (HWE); and (5) published data about the allele and genotype frequencies of SNPs must be sufficient. Studies were excluded if they did not meet all of these inclusion criteria. If more than one study by the same author using the same case series was published, either the study with the largest sample size or the most recent publication was included.
Data extraction
Data from the published studies were extracted independently by two authors into a standardized form. For each study, the following characteristics and numbers were collected: the first author, year of publication, country, language, ethnicity of subjects, study design, number of subjects, source of cases and controls, detecting sample, genotype method, allele and genotype frequencies, and evidence of HWE in controls. In cases of conflicting evaluations, disagreements among inconsistent data from the eligible studies were resolved through discussions and careful reexaminations of the full text by the authors.
Quality assessment
The quality of the included studies was assessed independently by two authors based on the Newcastle-Ottawa Scale (NOS) (Stang, 2010). The NOS criteria use a star rating system to judge the methodological quality, which was based on three perspectives of the study: selection, comparability, and exposure. Scores ranged from 0 stars (worst) to 9 stars (best); a score equal to or greater than 7 indicates a generally good methodological quality. Disagreements on NOS scores of the included studies were resolved through a comprehensive reassessment by the authors.
Statistical analysis
The crude odds ratios (OR) with 95% confidence intervals (CI) were calculated under five genetic models: the allele model (mutant [M] allele vs. wild [W] allele), the dominant model (WM+MM vs. WW), the recessive model (MM vs. WW+WM), the homozygous model (MM vs. WW), and the heterozygous model (MM vs. WM). Genotype frequencies of controls were tested for HWE using the χ2 test for each study included in the meta-analysis. The statistical significance of the pooled OR was examined using the Z test. Power calculations were done by PS Power and Sample Size Calculations (Dupont and Plummer, 1990). The Cochran's Q-statistic and I2 test were used to evaluate potential heterogeneity between studies (Peters et al., 2006; Jackson et al., 2012). If the Q-test showed a p<0.05 or I2 test exhibits >50%, indicating significant heterogeneity, the random-effects model was conducted; otherwise, the fixed-effects model was used. We also performed subgroup and meta-regression analyses to explore potential sources of heterogeneity (Ioannidis et al., 2008). Sensitivity analysis was performed by omitting each study in turn to evaluate the influence of single studies on the overall estimate. Begger's funnel plots and Egger's linear regression test were conducted to investigate publication bias (Zintzaras and Ioannidis, 2005). All calculations were performed using the STATA version 12.0 software (STATA Corporation, College Station, TX).
Results
Characteristics of the included studies
A total of 617 articles relevant to the searched keywords were initially identified. Of these articles, 452 were excluded after a review of their titles and abstracts; then, full texts and data integrity were reviewed, and another 154 articles were excluded. Eleven clinical case-control studies met our inclusion criteria for this meta-analysis (Georges et al., 2001; Nauck et al., 2002; Kelberman et al., 2004; Licastro et al., 2004; Lieb et al., 2004; Chiappelli et al., 2005; Fu et al., 2006; Park et al., 2007; Bennermo et al., 2011; Coker et al., 2011; Vakili et al., 2011). Publication years of the eligible studies ranged from 2001 to 2011. The flow chart of the study selection process is shown in Figure 1. The distribution of a number of topic-related literatures in the electronic database during the last decade is shown in Figure 2. A total of 10,252 subjects were involved in this meta-analysis, including 5429 MI patients and 4823 healthy controls. All the power for the sample size of included studies were higher than 0.70. Overall, eight studies were conducted in Caucasian populations and three studies in Asian populations, but no American data were found. Eight studies used population-based (community populations) controls, while the other three used hospital-based controls. The classical polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) method was performed in eight studies; two studies used TaqMan assay and the other one used allele-specific PCR. All the included studies were in HWE (all p>0.05). NOS scores of all included studies were higher than 6 (moderate high quality). Characteristics and methodological quality of the included studies are summarized in Table 1. A summary of the meta-analysis findings on the associations between IL-6 −174 G/C and −572 G/C polymorphisms and susceptibility to MI is provided in Table 2.
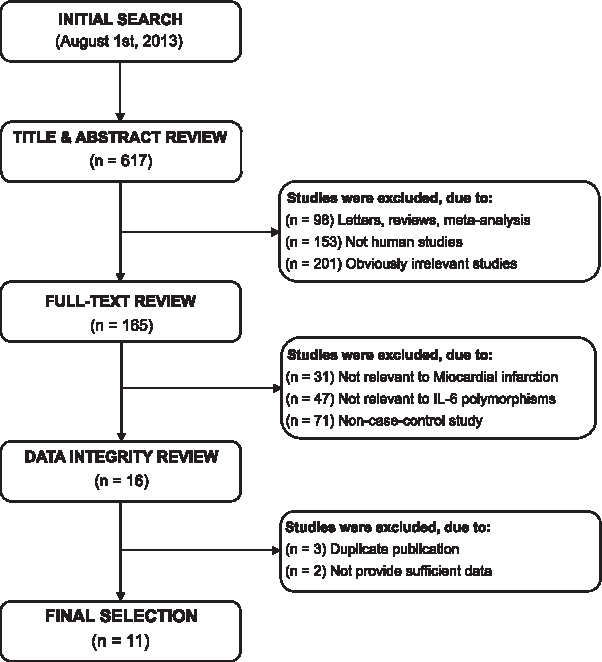
Flowchart shows study selection procedure. Eleven case-control studies were included in this meta-analysis.
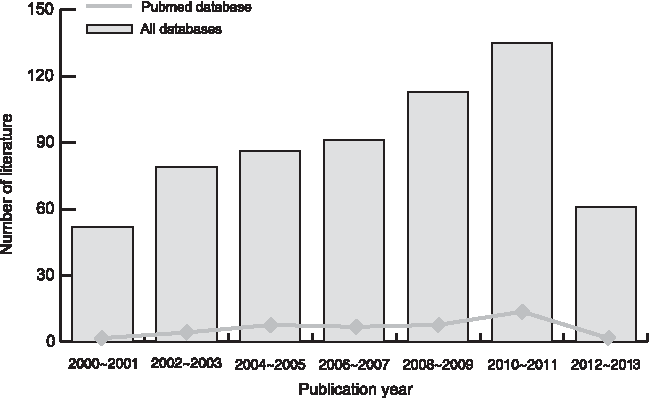
The distribution of a number of topic-related articles in the electronic database during the last decade.
M, male; F, female; PB, population based; HB, hospital based; SNP, single-nucleotide polymorphism; HWE, Hardy-Weinberg equilibrium; NOS, Newcastle-Ottawa Scale; PCR-RFLP, polymerase chain reaction-restriction fragment length polymorphism; AS-PCR, allele-specific PCR.
OR, odds ratios; 95% CI, 95% confidence intervals.
Association between IL-6 −174 G/C polymorphism and MI risk
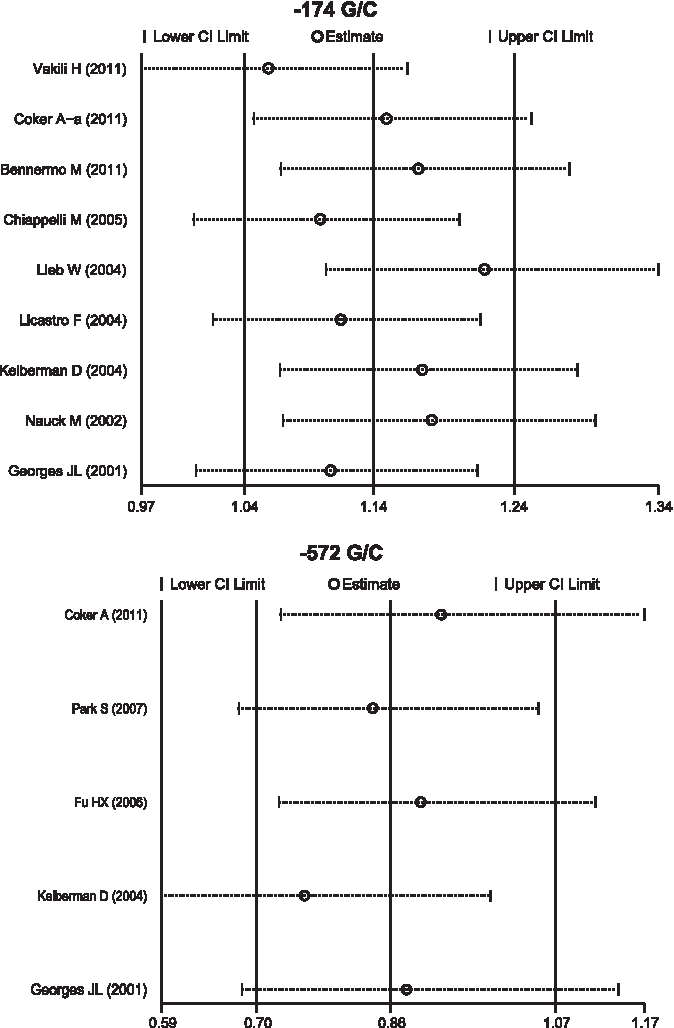
There were nine studies that referred to the association of IL-6 −174 G/C polymorphism with MI risk. The heterogeneity obviously existed, so the random-effects model was conducted to pool these results. The meta-analysis results revealed that IL-6 −174 G/C polymorphism may increase the risk of MI under the allele and dominant model (C allele vs. G allele: OR=1.07, 95% CI: 1.01-1.14, p=0.018; GC+CC vs. GG: OR=1.14, 95% CI: 1.04-1.24, p=0.003; respectively). However, no significant association was found under the recessive, homozygous, and heterozygous models (C allele vs. GG+GC allele: OR=1.04, 95% CI: 0.93-1.16, p=0.526; CC vs. GG: OR=1.09, 95% CI: 0.97-1.24, p=0.161; CC vs. GC: OR=1.01, 95% CI: 0.89-1.13, p=0.932; respectively). Subgroup analyses by source of controls and genotype methods indicated that there were significant associations between IL-6 −174 G/C polymorphism and increased risk of MI in the population-based (C allele vs. G allele: OR=1.08, 95% CI: 1.01-1.15, p=0.017; GC+CC vs. GG: OR=1.16, 95% CI: 1.05-1.27, p=0.003; respectively) and PCR-RFLP (C allele vs. G allele: OR=1.08, 95% CI: 1.01-1.15, p=0.036; GC+CC vs. GG: OR=1.14, 95% CI: 1.03-1.26, p=0.008; respectively) subgroups. Although IL-6 −174 G/C polymorphism showed no association with MI susceptibility in the hospital-based and other method subgroups Figs. 3-4), these results might have lacked sufficient reliability due to the estimation error from the effect size of a single study.

Subgroup analysis by source of controls for the association between IL-6 −174 G/C polymorphism and susceptibility to myocardial infarction under the allele and dominant models. CI, confidence intervals; OR, odds ratios.
Subgroup analysis by the genotype method for the association between IL-6 −174 G/C polymorphism and susceptibility to myocardial infarction under the allele and dominant models.
Association between IL-6 −572 G/C polymorphism and MI risk
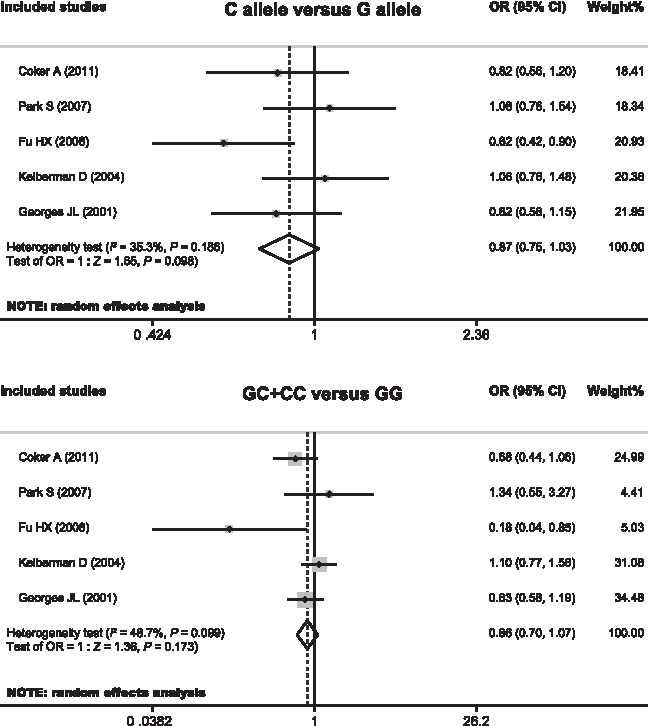
There were five studies that referred to the association between IL-6 −572 G/C polymorphism with MI risk. Since heterogeneity was significantly observed, the random-effects model was used. Meta-analysis of these studies showed no significant association between IL-6 −572 G/C polymorphism and MI risk (C allele vs. G allele: OR=0.88, 95% CI: 0.75-1.03, p=0.098; GC+CC vs. GG: OR=0.87, 95% CI: 0.70-1.07, p=0.173; CC vs. GG+GG: OR=0.85, 95% CI: 0.64-1.13, p=0.265; CC vs. GG: OR=0.81, 95% CI: 0.48-1.36, p=0.422; C vs. GG: OR=0.90, 95% CI: 0.67-1.21, p=0.477; respectively). Further subgroup analyses based on the source of controls and genotype methods also showed no association between IL-6 −572 G/C polymorphism and MI risk in each subgroup (all p>0.05) (Figs. 5-6).
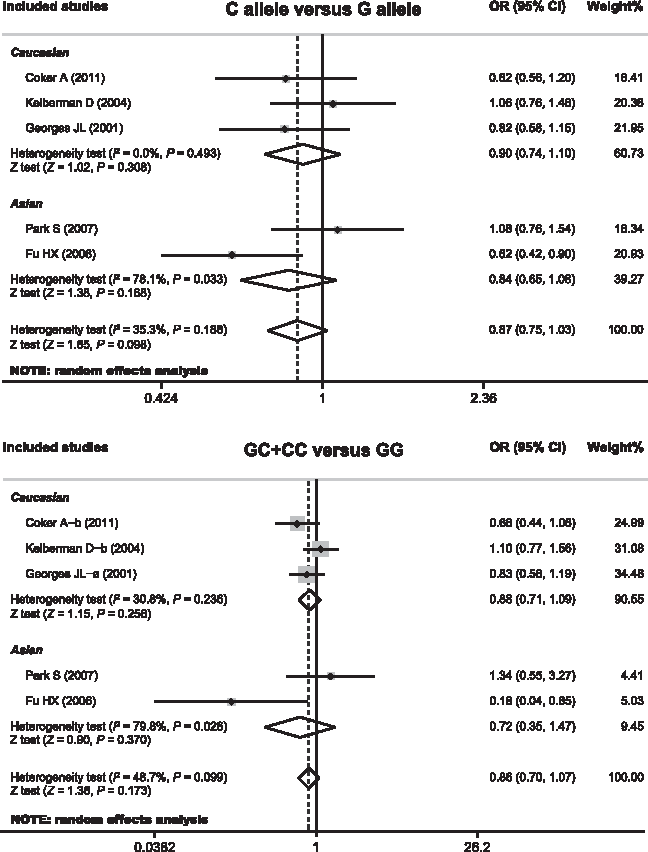
Subgroup analysis by source of controls for the association between IL-6 −572 G/C polymorphism and susceptibility to myocardial infarction under the allele and dominant models.

Subgroup analysis by the genotype method for the association between IL-6 −572 G/C polymorphism and susceptibility to myocardial infarction under the allele and dominant models.
Meta-regression and sensitivity analyses
Univariate and multivariate meta-regression analyses were conducted for IL-6 −174 G/C and −572 G/C polymorphisms. The results showed that no one factor may explain the source of heterogeneity (as shown in Table 3). Sensitivity analysis was performed to assess the influence of each individual study on the pooled OR by omitting each individual study. The analysis results suggested that no individual studies significantly affected the pooled OR of IL-6 −174 G/C and −572 G/C polymorphisms (Fig. 7), indicating a statistically robust result.
Sensitivity analysis of the association of IL-6 −174 G/C and −572 G/C polymorphisms with susceptibility to myocardial infarction. Results were computed by omitting each study in turn. Meta-analysis random-effects estimates (exponential form) were used. The two ends of the dotted lines represent the 95% CI.
SE, standard error; UL, upper limit; LL, lower limit.
Publication bias
The shapes of the funnel plots did not reveal any evidence of obvious asymmetry under the dominant model of IL-6 −174 G/C and −572 G/C polymorphisms (Fig. 8). Egger's test also displayed no significant statistical evidence of publication bias under any genetic models (−174 G/C: t=1.84, p=0.108; −572 G/C: t=−0.91, p=0.428), suggesting that no publication bias exists.
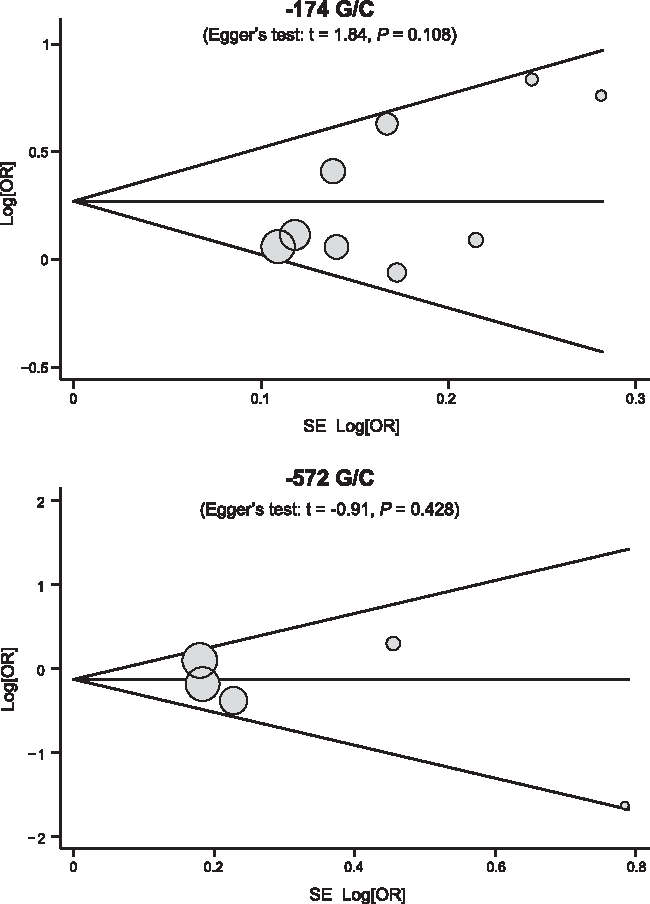
Begger's funnel plots of the association of IL-6 −174 G/C and −572 G/C with susceptibility to myocardial infarction. Each point represents a separate study for the indicated association. Log[OR], natural logarithm of OR. Horizontal line, mean magnitude of the effect.
Discussion
Interleukins are a group of cytokines transferring immune information and regulating the growth, differentiation, and proliferation of blood cells through a variety of receptors on target cells, and play an important role in the function of the immune system and inflammation (Banks and Kastin, 1991; Brocker et al., 2010). IL-6, a member of the human interleukin gene family, is a pleiotropic cytokine that has a broad range of humoral and cellular immune effects on inflammation, host defense, and tissue injury (Papanicolaou et al., 1998). Recently, IL-6 has been implicated in the development of atherogenesis and in the mediation of tissue damage (Licastro et al., 2004; Zee et al., 2008). MI is one of the many disorders involving tissue injury and atherosclerosis, which can provoke an acute phase response, suggesting that IL-6 is related to the infarcted area of the MI (Neri et al., 2013). Therefore, it is biologically plausible that genetic variations of the IL-6 gene may modulate MI risk (de Gaetano et al., 2011).
In this meta-analysis, 11 independent case-control studies were included with a total of 10,252 subjects, including 5429 MI patients and 4823 healthy controls. Two common polymorphisms (−174 G/C and −572 G/C) in the IL-6 gene have been evaluated. When all the eligible studies were pooled into the meta-analysis, the results revealed that IL-6 −174 G/C polymorphism was associated with an increased risk of MI, suggesting that IL-6 −174 G/C polymorphism may be a potential biomarker for early detection of MI. Although the exact function of IL-6 −174 G/C polymorphism in the development of MI among different populations is not yet clear, a possible reason could be that inherited mutations in IL-6 might be associated with changes in expression of inflammatory cytokines, and thereby could possibly explain interindividual differences in disease incidences of MI. However, our meta-analysis indicated that IL-6 −572 G/C polymorphism was not associated with increase susceptibility to MI. One possible reason could be that IL-6 −572 G/C polymorphism may not be an important determinant of MI susceptibility (Ridker et al., 2009). Since significant heterogeneity was observed, subgroup and meta-regression analyses were performed to explore the sources of heterogeneity. Further subgroup analyses showed that IL-6 −174 G/C polymorphism was associated with an increased risk of MI in the population-based and PCR-RFLP subgroups, indicating that the source of controls and genotype methods may be the potential sources of heterogeneity. However, our meta-regression analyses indicated that none of these factors explained heterogeneity among the studies. These disparate results may be due to the small sample size resulting in substantial errors from estimation. Our findings are consistent with the previous studies, suggesting that IL-6 gene polymorphisms may be associated with increased risk of MI and may be useful biomarkers for predicting an individual's susceptibility to MI.
In interpreting our results of the current meta-analysis, some limitations need to be addressed. The first major limitation is the relatively small sample size of this meta-analysis and selection bias due to the same origin (Europe and Asia), which may not have sufficient statistical power in estimating the association between IL-6 gene polymorphisms and MI risk. Therefore, more studies with larger sample sizes are still needed. On the other hand, as a type of a retrospective study that focuses on the summary of data from previously published studies, our meta-analysis may encounter recall or selection bias, thereby possibly influencing the reliability of the results (Stroup et al., 2000). Most importantly, the lack of access to all data from the original studies limits further evaluations of the potential values of IL-6 genetic polymorphisms. However, despite these statistical limitations, our study is the first comprehensive meta-analysis of all eligible studies concerning the relationship between IL-6 −174 G/C and −572 G/C polymorphisms and MI risk.
In conclusion, our meta-analysis suggests that IL-6 −174 G/C polymorphism may contribute to MI susceptibility. Thus, detection of IL-6 −174 G/C polymorphisms may be a promising biomarker for the early detection of MI. However, IL-6 −572 G/C polymorphism may not associate with the risk of MI. Due to the limitations mentioned above, further detailed studies are still required to confirm these findings.
Footnotes
Acknowledgments
The authors would like to acknowledge the reviewers for their helpful comments on this article. The authors would also like to thank their colleagues at the Department of Cardiology, The Fourth Affiliated Hospital of China Medical University.
Author Disclosure Statement
No competing financial interests exist.