
Abstract
Background: ATP-binding cassette transporter 1 (ABCB1) plays a critical role in the development and progression of cardiovascular disease. Emerging evidence suggests that common functional polymorphisms in the ABCB1 gene might have an impact on an individual's susceptibility to coronary heart disease (CHD), but individually published results are inconclusive. This meta-analysis aimed to derive a more precise estimation of the relationship between ABCB1 C3435T polymorphism and CHD risk. Method: An extensive literary search for relevant studies was conducted in PubMed, Embase, Web of Science, Cochrane Library, CISCOM, CINAHL, Google Scholar, China BioMedicine (CBM), and China National Knowledge Infrastructure (CNKI) databases from their inception through August 1st, 2013. Meta-analysis was performed using the STATA 12.0 software. The crude odds ratio (OR) with 95% confidence interval (CI) were calculated. Results: Seven clinical studies were included with a total of 13,074 CHD patients, including 378 variant angina pectoris (VAP) patients, 2290 myocardial infarction (MI) patients, and 10,406 acute coronary syndrome (ACS) patients. Our meta-analysis results indicated that ABCB1 C3435T polymorphism may be associated with an increased risk of CHD, especially for MI and ACS among Caucasian populations. However, no statistically significant association was found between ABCB1 C3435T polymorphism and VAP risk, especially among Asian populations. Meta-regression analyses showed that clinical subtype and ethnicity may be the main sources of heterogeneity. No publication bias was detected in this meta-analysis. Conclusion: The current meta-analysis suggests that ABCB1 C3435T polymorphism may contribute to the risk of CHD, especially for MI and ACS, among Caucasian populations. Thus, detection of ABCB1 C3435T polymorphism may be a promising biomarker for the early detection of CHD.
Introduction
C
Human ATP-binding cassette transporter 1 (ABCB1, also called MDR1) is a phylogenetically highly conserved super family of transport proteins that participates in the systemic response to inflammation (Jones and George, 2004). ABCB1 is a highly sensitive marker of inflammation, and elevated serum levels of ABCB1 have been concerned with the future risk of CHD (Meissner et al., 2004). Human ABCB1 gene is located on chromosome 7q21 in humans and encodes 1280 amino acids, containing 12 transmembrane sequences (Aszalos, 2007). Genetic variations in the ABCB1 gene may alter the expression, structure, and function of P-glycoprotein (ABCB1) and thereby affect individual susceptibility to CHD (Ding and Kullo, 2009; Lieb and Vasan, 2013). Therefore, it was hypothesized that common polymorphisms in the ABCB1 gene could be functional and were associated with the development of myocardial infarction (MI). Several single nucleotide polymorphisms (SNPs) in the ABCB1 gene have been identified as candidates for CHD susceptibility; among them, C3435T (rs1045642 C>T) is the most common variant that has been widely investigated (Chowbay et al., 2005; Bournissen et al., 2009; Haerian et al., 2010). Recently, many studies have indicated that ABCB1 C3435T polymorphism might play a critical role in increasing CHD risk (Simon et al., 2009; Wallentin et al., 2010; Shalia et al., 2013). However, there is also some evidence that ABCB1 C3435T polymorphism had no effect on susceptibility to CHD (Poduri et al., 2009; Spiewak et al., 2009). In view of the conflicting results from previous studies, we performed a meta-analysis of all available data to evaluate the associations between ABCB1 C3435T polymorphism and CHD risk.
Materials and Methods
Literature search strategy
A comprehensive search for relevant studies published before August 1, 2013 was conducted on the PubMed, Embase, Web of Science, Cochrane Library, CISCOM, CINAHL, Google Scolar, China BioMedicine (CBM), and China National Knowledge Infrastructure (CNKI) databases. We used the following keywords and MeSH terms: (“genetic polymorphism” or “single nucleotide polymorphism” or “polymorphism” or “SNP” or “mutation” or “variation” or “variant”) and (“coronary heart disease” or “CHD” or “myocardial infarction” or “myocardial infarct” or “MI” or “AMI” or “variant angina pectoris” or “VAP” or “acute coronary syndrome” or “ACS”) and (“ATP-binding cassette transporter 1” or “ABCB1” or “ATP-binding cassette” or “CERP”). There were no language restrictions. The references used in eligible articles or textbooks were also reviewed to find other potential studies.
Inclusion and exclusion criteria
Studies included in our meta-analysis have to meet the following criteria: (1) clinical case-control or cohort studies focused on the association between ABCB1 C3435T polymorphism and CHD risk; (2) all patients should meet the diagnostic criteria for CHD; (3) the minimum number of cases in included studies should be greater than 30; (4) published data about the allele and genotype frequencies of SNPs must be sufficient. Studies were excluded if they did not meet all of these inclusion criteria. If more than one study by the same author using the same case series was published, either the study with the largest sample size or the most recent publication was included.
Data extraction
Data from the published studies were extracted independently by two authors into a standardized form. For each study, the following characteristics and numbers were collected: the first author, year of publication, country, language, ethnicity of subjects, study design, number of subjects, detecting sample, genotype method, and allele and genotype frequencies. In cases of conflicting evaluations, disagreements among inconsistent data from the eligible studies were resolved through discussions and careful reexamination of the full text by the authors.
Quality assessment
The quality of the included studies was assessed independently by two authors based on the Newcastle-Ottawa Scale (NOS) (Stang, 2010). The NOS criteria use a “star” rating system to judge the methodological quality, which was based on three perspectives of the study: selection, comparability, and exposure. Scores ranged from 0 stars (worst) to 9 stars (best); a score equal to or greater than 7 indicates a generally good methodological quality. Disagreements on NOS scores of the included studies were resolved through a comprehensive reassessment by the authors.
Statistical analysis
The crude odds ratio (OR) with 95% confidence interval (CI) were calculated under five genetic models: the allele model (T allele vs. C allele), the dominant model (CT+TT vs. CC), the recessive model (TT vs. CC+CT), the homozygous model (TT vs. CC), and the heterozygous model (TT vs. CT). Genotype frequencies of controls were tested for Hardy-Weinberg equilibrium (HWE) using the χ2 test for each study included in the meta-analysis. The statistical significance of the pooled OR was examined using the Z test. Power calculations were done by PS Power and Sample Size Calculations (Dupont and Plummer, 1990). Between-study heterogeneity was estimated using Cochran's Q-statistic, whereas a ph<0.05 was set to identify heterogeneity in the associations (Jackson et al., 2012). We also quantified the effects of heterogeneity by using the I2 test (ranges from 0% to 100%), which represents the proportion of inter-study variability that can be contributed to heterogeneity rather than to chance (Peters et al., 2006). When a significant Q-test with p<0.05 or I2>50% indicated existence of heterogeneity among studies, the random effects model (DerSimonian Laird method) was conducted for the meta-analysis; otherwise, the fixed effects model (Mantel-Haenszel method) was used. To explore potential sources of heterogeneity, subgroup analysis was performed by clinical subtype, ethnicity, and genotype method. Sensitivity analysis was performed by omitting each study in turn to assess the quality and consistency of the results. Begger's funnel plots and Egger's linear regression test were used to evaluate the publication bias (Zintzaras and Ioannidis, 2005). Two-sided p<0.05 was considered to be statistically significant. All calculations were performed using the STATA version 12.0 software (STATA Corporation, College Station, TX).
Results
Characteristics of the included studies
A total of 90 articles relevant to the searched keywords were initially identified. Of these articles, 69 were excluded after a review of their titles and abstracts; then, full texts and data integrity were reviewed, and another 14 articles were excluded. Seven clinical studies met our inclusion criteria for this meta-analysis (Poduri et al., 2009; Simon et al., 2009; Spiewak et al., 2009; Wallentin et al., 2010; Cayla et al., 2011; Ayaz et al., 2013; Shalia et al., 2013). Publication years of the eligible studies ranged from 2009 to 2013. The flowchart of the study selection process is shown in Figure 1. The distribution of the number of topic-related studies in the electronic database during the last decade was shown in Figure 2. A total of 13,074 CHD patients were involved in this meta-analysis, including 378 variant angina pectoris (VAP) patients, 2290 MI patients and 10,406 ACS patients. About 506 healthy controls of four case-control studies (Poduri et al., 2009; Cayla et al., 2011; Ayaz et al., 2013; Shalia et al., 2013) were used as the standardized control group. All the power for the sample size of included studies were higher than 0.70. Overall, five studies were conducted in Caucasian populations and two studies in Asian populations. The classical polymerase chain reaction-restriction fragment length polymorphism (PCR-RELP) method was performed in four studies; the other three studies used a TaqMan assay. Genotype frequencies of controls were in HWE (p=0.172). NOS scores of all included studies were higher than 6 (moderate-high quality). Characteristics and methodological quality of the included studies are summarized in Table 1.

Flowchart shows study selection procedure. Seven clincial studies were included in this meta-analysis.

The distribution of the number of topic-related literature in the electronic database during the last decade.
M, male; F, female; SNP, single nucleotide polymorphism; VAP, variant angina pectoris; MI, myocardial infarction; ACS, acute coronary syndrome; PCR-RFLP, polymerase chain reaction-restriction fragment length polymorphism; NOS, the Newcastle-Ottawa Scale.
Quantitative data synthesis
A summary of the meta-analysis findings on the associations between ABCB1 C3435T polymorphism and susceptibility to CHD is provided in Table 2. No heterogeneity was observed under any genetic models, so a fixed effects model was conducted to pool these results. The meta-analysis results revealed that ABCB1 C3435T polymorphism may increase the risk of CHD (T allele vs. C allele: OR=1.40, 95% CI: 1.31-1.49, p<0.001; CT+TT vs. CC: OR=1.60, 95% CI: 1.46-1.76, p<0.001; TT vs. CC+CT: OR=1.48, 95% CI: 1.33-1.65, p<0.001; TT vs. CC: OR=1.89, 95% CI: 1.67-2.14, p<0.001; TT vs. CT: OR=1.27, 95% CI: 1.13-1.42, p<0.001; respectively).
OR, odds ratios; 95% CI, 95% confidence interval; ABCB1, ATP-binding cassette transporter 1; CAD, coronary artery disease.
Subgroup analysis by clinical subtype indicated that there were significant associations between ABCB1 C3435T polymorphism and increased risk of MI and ACS (all p<0.05), but no significant association with VAP risk (Fig. 3). Further subgroup analysis by ethnicity suggested that there were significant associations between ABCB1 C3435T polymorphism and increased risk of CHD among Caucasian populations, but no significant association was found among Asian populations (Fig. 4). In the stratification analysis by genotype method, significant associations of ABCB1 C3435T polymorphism with increased risk of CHD were found in both the PCR-RFLP and TaqMan subgroups (Fig. 5).
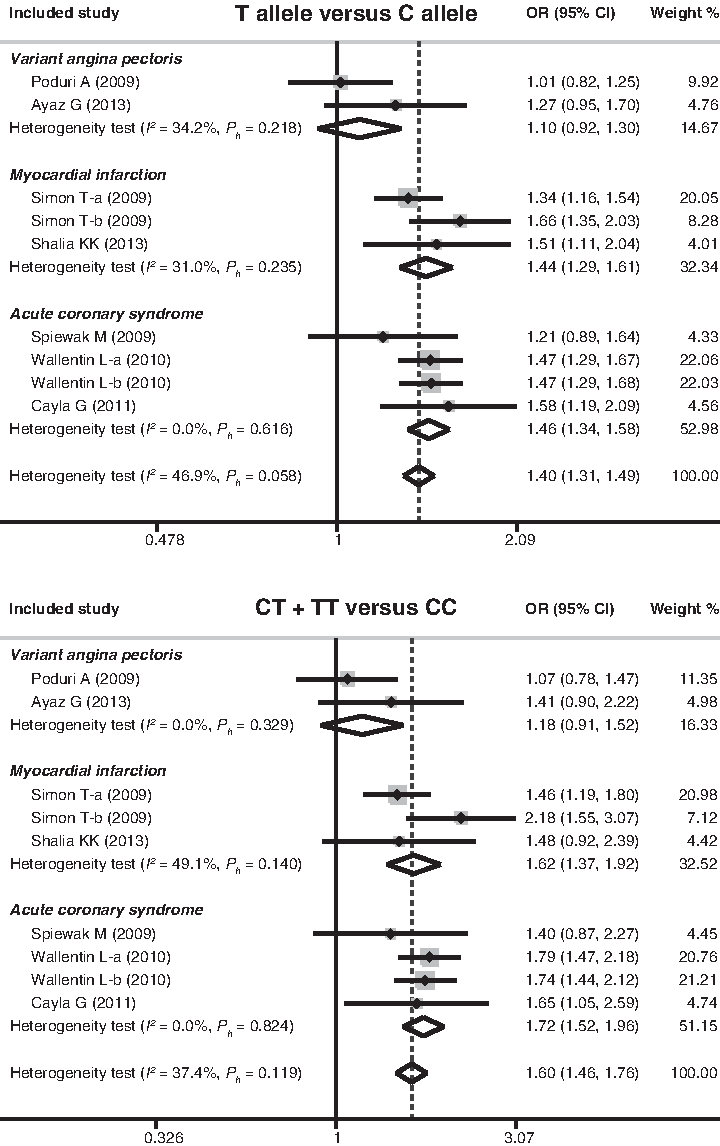
Subgroup analysis by clinical subtype for the association between ATP-binding cassette transporter 1 (ABCB1) C3435T polymorphism and susceptibility to ischemic heart disease under the allele and dominant models.

Subgroup analysis by ethnicity for the association between ABCB1 C3435T polymorphism and susceptibility to ischemic heart disease under the allele and dominant models.
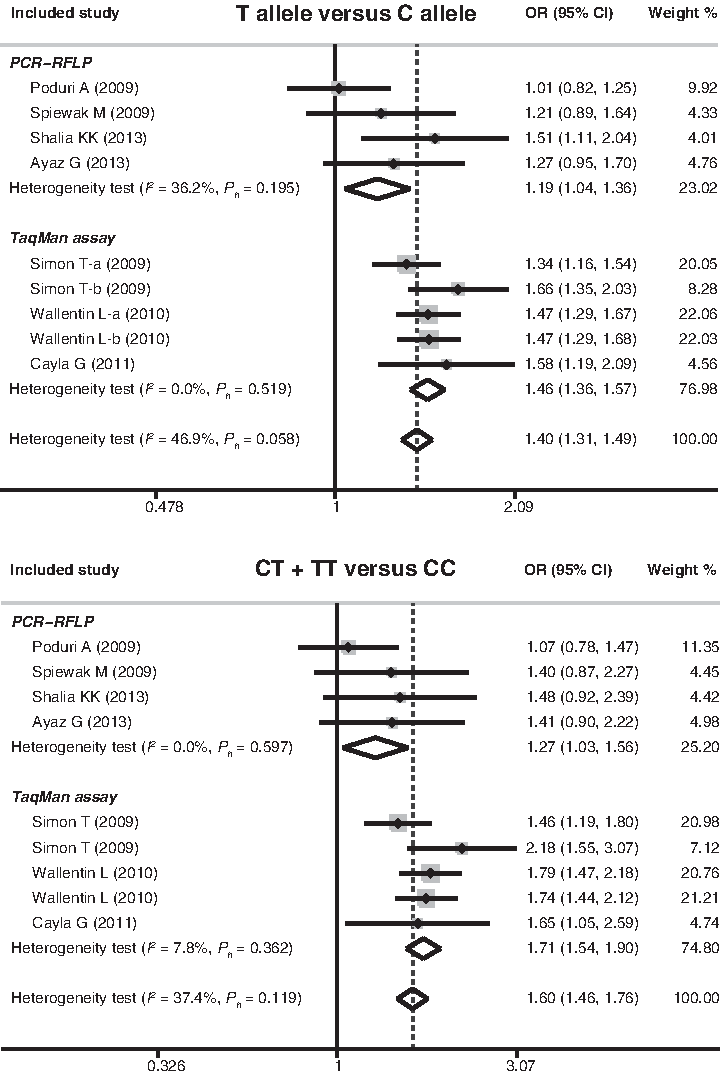
Subgroup analysis by genotype method for the association between ABCB1 C3435T polymorphism and susceptibility to ischemic heart disease under the allele and dominant models.
Meta-regression and sensitivity analyses
Univariate and multivariate meta-regression analyses were conducted for the associations of ABCB1 C3435T polymorphism with CHD risk. The results showed that clinical subtype and ethnicity may be the main sources of heterogeneity (as shown in Table 3). Sensitivity analysis was performed to assess the influence of each individual study on the pooled OR by omitting each individual study. The analysis results suggested that no individual studies significantly affected the pooled OR (Fig. 6), indicating a statistically robust result.

Sensitivity analysis of the association between ABCB1 C3435T polymorphism and susceptibility to ischemic heart disease under the allele and dominant models. Results were computed by omitting each study in turn. Meta-analysis random-effects estimates (exponential form) were used. The two ends of the dotted lines represent the 95% confidence interval.
SE, standard error; UL, upper limit; LL, lower limit.
Publication bias
The shapes of the funnel plots did not reveal any evidence of obvious asymmetry under the dominant model of ABCB1 C3435T polymorphism (Fig. 7). Egger's test also displayed no significant statistical evidence of publication bias under any genetic models (t=−0.53, p=0.612), suggesting that no publication bias exists.
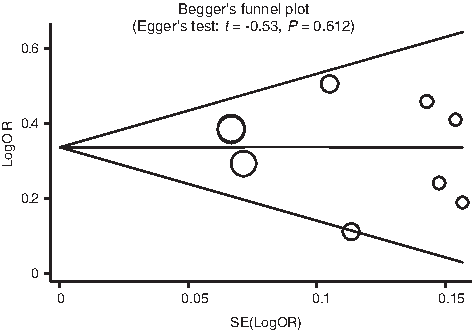
Begger's funnel plots of the association of ABCB1 C3435T polymorphism with susceptibility to ischemic heart disease. Each point represents a separate study for the indicated association. Log[OR], natural logarithm of odds ratio. Horizontal line, mean magnitude of the effect.
Discussion
ABCB1, also called the human multidrug resistance 1 gene (MDR1), is a pivotal member of the ABC group of proteins (Hoffmann and Kroemer, 2004). The superfamily of ABC possesses the ability to modulate and transport a variety of substrates such as sugars, amino acids, proteins, ions, toxins, and drugs (Wei et al., 2012). The clinical significance of ABCB1 includes not only its involvement in multidrug resistance in cancer but also its effects on the pharmacokinetic properties of various drugs (Kimura et al., 2007). It has been suggested that ABCB1 seemed to be an important candidate gene affecting the susceptibility to various diseases (Gao, 2013). Mutational analysis has indicated that the ABCB1 gene is highly polymorphic, contributing more to its significance for the study of its association with human diseases (Hoffmeyer et al., 2000). Due to the various modulating functions of ABCB1, it is plausible to hypothesize that ABCB1 gene may have association with CHD risk. There were several previous studies suggesting that some specific polymorphisms in the promoter region of the ABCB1 gene may importantly modulate the development and progression of CHD (Peters et al., 2010), while other studies had investigated no evidence of ABCB1 polymorphism showing its important role in the risk of CHD. The existence of such controversy could be resulted from several factors such as the differences in study designs, sample size, ethnicity, source of controls, genotype methods, and so on.
Our study is the first comprehensive meta-analysis of all eligible studies concerning the role of ABCB1 C3435T polymorphism in the etiology of CHD. In this meta-analysis, seven independent clinical studies were included with a total of 13,074 CHD patients, including 378 VAP patients, 2290 MI patients, and 10,406 ACS patients. When all the eligible studies were pooled into the meta-analysis, the results revealed that ABCB1 C3435T polymorphism was associated with an increased risk of CHD, suggesting that ABCB1 C3435T polymorphism may represent a potential biomarker for CHD. The ABCB1 C3435T polymorphism (rs1045642, also known as Ile1145Ile), a transversion mutation of C to T substitution at position 3435 in exon 26, could alter expression and function of ABCB1, thereby possibly affecting individual susceptibility to CHD (Schwab et al., 2003; Su et al., 2012).
In the stratification analysis by clinical subtype, ABCB1 C3435T polymorphism showed significant associations with increased risk of MI and ACS. Nevertheless, we observe no significant association between ABCB1 C3435T polymorphism and VAP risk. Although the exact function of ABCB1 in the development of CHD is not clear yet, a potential explanation might be that ABCB1 gene mutations could increase the ATPase activity of ABCB1 that might be associated with changes in cholesteryl ester synthesis and result in low high-density lipoprotein cholesterol (HDL-C) levels, thereby possibly explaining inter-individual differences in disease incidences of CHD (Ridker et al., 2009; Munic et al., 2010). Our results indicated that ABCB1 C3435T polymorphism might increase the risk of CHD among Caucasian populations, but not among Asian populations. Although ethnic differences in susceptibility to CHD are well known, the molecular basis is still not fully understood. One possible explanation for this difference could be that large differences in common SNPs influencing the risk of CHD are mostly due to genetic drifts and natural selection (Serre et al., 2008). Subgroup analyses results showed that differences in clinical subtype and ethnicity might be the main sources of heterogeneity. Meta-regression analyses also confirmed that clinical subtype and ethnicity could potentially explain the sources of heterogeneity. Our findings are consistent with the previous studies, suggesting that ABCB1 C3435T polymorphism may be associated with increased risk of CHD and may be useful biomarkers for predicting an individual's susceptibility to CHD.
Some limitations of this meta-analysis should be acknowledged. First, there were only nine articles included in the present meta-analysis, so the sample size was relatively small and may not provide sufficient statistical power to estimate the correlation between common polymorphisms in ABCB1 gene and susceptibility to CHD. Therefore, more studies with larger sample size are still needed to accurately provide a more representative statistical analysis. Second, as a type of a retrospective study, a meta-analysis may encounter recall or selection bias and may possibly influence the reliability of our study results (Stroup et al., 2000). Third, our lack of access to the original data from the studies limited further evaluations of the potential interactions between other factors including HDL-C levels and dyslipidemia history and susceptibility to CHD, such as gene-environment and gene-gene interactions.
In conclusion, our meta-analysis suggests that ABCB1 C3435T polymorphism may contribute to the risk of CHD, especially for MI and ACS among Caucasian populations. Thus, detection of ABCB1 C3435T polymorphism may be a promising biomarker for the early detection of CHD. However, due to the limitations mentioned above, further detailed studies are still required to confirm our findings.
Footnotes
Acknowledgments
We would like to acknowledge the reviewers for their helpful comments on this article. We would also like to thank our colleagues at the Department of Cardiology, The Fourth Affiliated Hospital of China Medical University.
Author Disclosure Statement
No competing financial interests exist.