
Abstract
Objectives: The aim of this study is to compare preoperative and postoperative conditions of GMP-140 concentration, the aggregation and activation of platelets in congenital heart disease patients undergoing transcatheter closure of atrial septal defects (ASDs) or ventricular septal defects (VSDs), and the appropriate dose of aspirin of patients after transcatheter closure. Materials and Methods: Thirty-two consecutive patients with ASD (n=16) and VSD (n=16), as shown on transthoracic echocardiography and right heart catheter examination, were treated with a percutaneous catheter occlusion. The patients comprised 13 males and 19 females with a mean age of 25.6±9.15. Patients were randomly assigned into two groups within half an hour after ASD or VSD occlusion. Group A cases were treated with 3 mg/kg/day enteric-coated aspirin tablets for 6 months, while patients in group B received 5 mg/kg/day enteric-coated aspirin tablets for 6 months. Results: The rates of platelet aggregation (PAG) in the immediate postoperative ASD/VSD occlusion were significantly higher than those in the preoperative ASD/VSD occlusion (adenosine diphosphate [ADP]-induced PAG: 64.98%±7.65% vs. 86.33%±6.54%, p<0.05; arachidonic acid [AA]-induced PAG: 62.92%±9.11% vs. 86.96%±6.90%, p<0.05, respectively). After treatment with aspirin, the GMP-140 levels presented a clearly defined downward trend in the immediate postoperative period (3 mg/kg/day aspirin: 18.30±3.42 vs. 13.37±1.80, p<0.05; 5 mg/kg/day aspirin: 18.30±3.42 vs. 13.41±1.60, p<0.05), but no obvious difference was observed considering the GMP-140 levels in the 4 days after occlusion (all p>0.05). Conclusion: Our study showed that the GMP-140 serum level and PAG were increased after ASD and VSD occlusion, and patients may have a trend of decreased GMP-140 serum levels after the ASD or VSD occlusion surgeries after the treatment with aspirin. Daily oral administration of 3 and 5 mg/kg/day aspirin can induce a significant decrease in PAG of patients after VSD/ASD occlusion.
Introduction
C
In recent years, there is growing consensus driven by both clinical and experimental evidence that aspirin has been accepted as one of the most commonly prescribed antiplatelet agents in patients, especially in those with CHD, undergoing percutaneous implantation of potentially thrombogenic intracavitary devices (Wiegand et al., 2010; Zhu et al., 2013; Moszura et al., 2014). To the best of our knowledge, transcatheter closure of ASDs or VSDs should be performed under full anticoagulation, and once the device is in place, treatment with aspirin is routinely prescribed for several months (Rodes-Cabau et al., 2005). It is well known that aspirin exerts its antithrombotic effect to inhibit platelet aggregation (PAG) and reduce platelet activity, which is largely attributed to its irreversible inactivation of cyclooxygenase, leading to impaired platelet function (Cholette et al., 2010). It is important to note that most patients demonstrate an adequate response to 3-5 mg/kg/day of aspirin for 6 months, which is at present the dose generally recommended for the prophylaxis of thromboembolic events after interventional closure of ASD (Heistein et al., 2008). Nevertheless, a significant improvement has not been consistently found in response to doubling the dose of aspirin in those with a poor antiplatelet response, which lends additional evidence to demonstrate that increasing the aspirin dosage may not markedly affect its antiplatelet effects (Wiegand et al., 2010).
On the contrary, there is even accumulating evidence that increasing the aspirin dosage may cause adverse reactions of the gastrointestinal tract in patients (Huang et al., 2011; Sostres and Lanas, 2011). Based on this, the relationship between aspirin dose and treatment effect remains controversial, and therefore, the goal of the present study was to investigate whether an increase of aspirin dose in CHD patients post-transcatheter closure of ASDs or VSDs may be of any effect, and possibly, to find the optimal aspirin dose among those patients.
Materials and Methods
Ethics
The protocol was authorized by the ethics committee of Xiangya Hospital of Central South University. The study also conforms to the ethical principles for medical research involving human subjects established by the World Medical Association Declaration of Helsinki (World Medical, 2013). Written informed consent was obtained from all participants in their preferred language before the enrollment.
Subjects and grouping
From June 2005 to March 2006, 32 consecutive patients with ASD (n=16) and VSD (n=16) documented by transthoracic echocardiography and right heart catheter examination were treated with percutaneous catheter occlusion at the Department of Cardiology in Xiangya Hospital of Central South University. The patients included 13 males and 19 females with a mean age of 25.6±9.15. Patients were eligible for inclusion if they (1) had secundum ASD (diameter <40 mm) with evidence of the left-to-right shunt, and all defects had a distance of >4 mm from vital cardiac structures (atrioventricular valves, superior caval vein, upper right pulmonary vein, and coronary sinus); (2) had VSD with hemodynamically relevant left-to-right shunt along with defects of <16 mm, a ≥1.5 mm distance between the upper edge of the defect and the aortic valve, and without aortic valve regurgitation and aortic valve prolapse. Exclusion criteria were as follows: (1) performing any other interventional procedures at the same time; (2) who had suffered from atrial fibrillation, peptic ulcer disease, liver and kidney dysfunction; (3) with abnormal platelet counts and platelet function perioperatively; and (4) had a history of antiplatelet drug and aspirin intolerance before the experiment. Patients who satisfied the inclusion and exclusion criteria were randomly assigned into group A and group B within half an hour after occlusion. Patients in group A were treated with 3 mg/kg/day enteric-coated aspirin tablets for 6 months, whereas patients in group B received 5 mg/kg/day enteric-coated aspirin tablets for 6 months.
VSD/ASD occlusion
Domestic-made VSD occluder (Shanghai sharp Memory Alloy Co., Ltd., SHSMA, Shanghai, China) consists of a composite nickel and titanium occluder with a screw, a delivery sheath, and a pushing rod, and the Seercare Cera ASD occluder (Lifetech Scientific, Shenzhen, China) were used to perform percutaneous occlusion. The inserted mesh (Seercare Cera ASD occluder) was composed of a nitinol wire frame and Dacron fabric. The device implantation procedures were described previously (Xu et al., 2013).
Specimen collection
Venous blood was drawn through a 19G needle with participants in the supine position at preoperative, immediate postoperative, and 4 days after occlusion by sterile, atraumatic venipuncture, then blood samples were collected into vacutainer citrate tubes (Vacuette; Greiner-Bio-One; containing 1/9 volume sodium citrate stock solution at 0.129 mM). Five milliliter blood samples were collected for analysis of PAG. Additional 5 mL blood samples were placed into a centrifuge tube and immediately centrifuged at 3000 rpm for 15 min. The supernatant was drawn into an Eppendorf centrifuge tube (EP tube), frozen at −70°C until the experimental analysis for the detection of granule membrane protein 140 (GMP-140).
Platelet preparation and aggregations
The first 5 mL blood samples were centrifuged at 1000 rpm for 10 min at 37°C without brake. The supernatant (platelet-rich plasma [PRP]) was aspirated, collected in a plastic tube, and marked. Autologous platelet-poor plasma (PPP) was obtained by further centrifugation at 3000 rpm for 15 min at room temperature with brake. Platelet counts in the PRP were in the range of 200-400×109/L; if platelet counts >400×109/L, autologous PPP was applied to dilute the platelet counts into 350×109/L. Platelet counts in the PPP were in the range of 10-20×107/L. PAG was recorded as changes in light transmission. The recorder was adjusted to make sure that the difference in light transmission between PRP and PPP was 100%. Subsequently, the PAG agonist (30ul), either 10 μM adenosine diphosphate (ADP) or 1.0 mM arachidonic acid (AA) was added and the results of optical platelet aggregometry are presented as the amplitude of light transmittance at 5 min. All aggregation tests were performed within 2 h of blood collection. The maximal aggregation response to each agonist was considered after 5 min.
Characterization of platelet GMP-140
Platelets were identified with a fluorescein isothiocyanate (FITC)-conjugated anti-CD42a monoclonal antibody. Platelet GMP-140 expression was determined by a R phycoerythrin (RPE)-conjugated anti-GMP-140 monoclonal antibody (Becton Dickinson, San Jose, CA) according to a previous study (Yngen et al., 2004). In detail, the FITC- and RPE-conjugated isotypic monoclonal antibodies DAK-GO1 (Dakopatts) were used as negative controls. Agonists used were ADP (1 μM) and thrombin (0.02, 0.03, 0.04, 0.08 IU/mL). When thrombin was used, clotting was prevented by the peptide gly-pro-arg-pro. Within 3 min of collection, 5 μL citrated whole blood was added to 45 μL of HEPES-buffered saline containing antibodies and agonists and incubated at room temperature for 20 min. Samples were then diluted and fixed with 0.5% formaldehyde saline before analysis, using a Coulter EPICS XL-MCL flow cytometer (Coulter, Hialeah, FL). Platelets were discriminated from other blood cells by their light scattering characteristics and live gated in an electronic bit map. The gated cells were subsequently subjected to single color analysis of RPE-CD62P fluorescence to obtain the percentage of GMP-140-positive cells in the platelet population.
Statistical analyses
Categorical data are expressed as percentages, and continuous variables are expressed as mean±standard deviation. Categorical variables of the study and control groups were compared with the χ2 test, and continuous variables were compared with Student's t-test. Linear correlation analysis was used for correlation analysis between two variables. Differences resulting in p-values less than 0.05 were considered to be statistically significant. A commercially available statistical package (SPSS 11.5) was used for all analyses.
Results
Changes in PAG before and after ASD/VSD occlusion
Comparisons of the PAG and the plasma levels of GMP-140 were performed in patients before and after ASD/VSD occlusion (Figs. 1 and 2). The rates of PAG in the immediate postoperative ASD/VSD occlusion were significantly higher than those in the preoperative ASD/VSD occlusion (ADP-induced PAG: 64.98%±7.65% vs. 86.33%±6.54%, p<0.05; AA-induced PAG: 62.92%±9.11% vs. 86.96%±6.90%, p<0.05, respectively) (Table 1). Additionally, compared with preoperative PAG, results showed evidence of a significant decrease in the AA-induced PAG in the 4 days after ASD/VSD (62.92%±9.11% vs. 19.29%±5.73%, p<0.05); whereas no obvious difference was found in the ADP-induced PAG between the preoperative period and four postoperative days (all p>0.05) (Table 1).
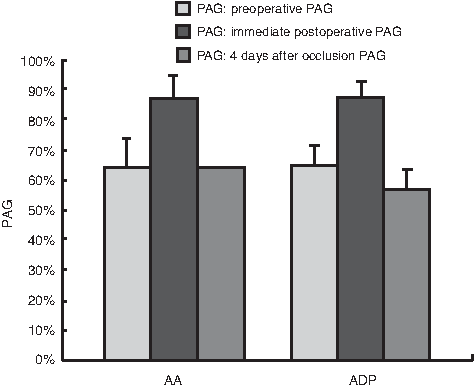
The changes of platelet aggregation (PAG) before and after transcatheter closure of ASD and VSD. ASD, atrial septal defect; VSD, ventricular septal defect.
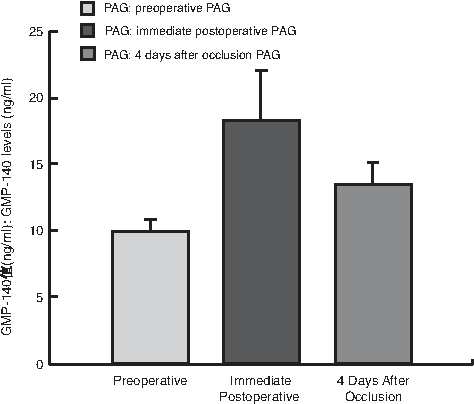
The changes of GMP-140 concentrations before and after transcatheter closure of ASD and VSD.
p>0.05 compared with the preoperative.
p<0.05 compared with the preoperative.
p<0.05 compared with the immediate postoperative.
AA, arachidonic acid; ADP, adenosine diphosphate; PAG, platelet aggregation.
Changes in GMP-140 levels before and after ASD/VSD
We also observed a significant increase in GMP-140 levels before ASD/VSD occlusion in contrast with those after ASD/VSD occlusion (9.73±1.01 vs. 18.30±3.42, p<0.05) (Table 1). Results revealed that the GMP-140 levels in the four postoperative days showed a significant decrease when compared with immediate preoperative periods (9.73±1.01 vs. 13.39±1.68, p<0.05) (Table 1). Furthermore, immediate postoperative GMP-140 levels in the VSD occlusion patients were significantly higher in contrast to ASD occlusion patients (16.69±2.09 vs. 19.91±3.78, p=0.01) (Table 2).
ASD, atrial septal defect; VSD, ventricular septal defect.
Correlation between GMP-140 levels and clinical parameters
Relationships between the plasma levels of the platelet activation markers (GMP-140 levels) and clinical parameters were examined. Linear correlation analysis was performed and results in the current study suggested that the immediate postoperative GMP-140 levels in VSD/ASD occlusion patients were positively associated with the operation time (VSD: r=0.74, p<0.01; ASD: r=0.73, p<0.01, respectively) (Tables 3 and 4). However, there was no significant correlation with immediate postoperative GMP-140 levels and age, gender or the size of occluder. Furthermore, no obvious correlations were observed between the GMP-140 levels in the four postoperative days and clinical parameters mentioned above (all p>0.05) (Figs. 3-5).

The relativity between immediate postoperative GMP-140 concentrations and operating time in patients with VSD after transcatheter closure.
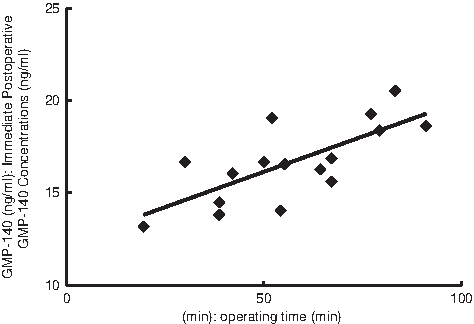
The relativity between immediate postoperative GMP-140 concentrations and operating time in patients with ASD after transcatheter closure.

Comparisons of GMP-140 concentrations in patients with VSD and ASD before and after transcatheter closure.
p<0.01 indicating that there was a significant correlation between GMP-140 concentrations and clinical parameters in patients with VSD after transcatheter closure.
p<0.01 indicating that there was a significant correlation between GMP-140 concentrations and clinical parameters in patients with ASD after transcatheter closure.
Effect of various doses of aspirin on platelet activation
The effects of various doses of aspirin on platelet activation are shown in Table 5. Findings in the present study demonstrated that both the 3 mg/kg/day aspirin-treated group and the 5 mg/kg/day aspirin-treated group induced a significant decrease in ADP-induced PAG (3 mg/kg/day aspirin: 86.33%±6.54% vs. 56.06%±6.87%, p<0.05; 5 mg/kg/day aspirin: 86.33%±6.54% vs. 55.93%±6.35%, p<0.05, respectively) and AA-induced PAG (3 mg/kg/day aspirin: 86.96%±6.90% vs. 19.84%±6.07%, p<0.05; 5 mg/kg/day aspirin: 86.96%±6.90% vs. 20.53%±4.67%, p<0.05, respectively) in the immediate postoperative periods. Whereas in the four postoperative days, ADP/AA-induced PAG did not differ from that treated with aspirin (all p>0.05). After aspirin treatment, the GMP-140 levels displayed a decreased trend in the immediate postoperative (3 mg/kg/day aspirin: 18.30±3.42 vs. 13.37±1.80, p<0.05; 5 mg/kg/day aspirin: 18.30±3.42 vs. 13.41±1.60, p<0.05), but the GMP-140 levels in the 4 days after occlusion showed no obvious difference (all p>0.05). However, there was no significant difference in the PAG (ADP-induced PAG: 56.06%±6.87% vs. 55.93%±6.35%, p=0.72; AA-induced PAG: 19.84%±6.07% vs. 20.53%±4.67%, p=0.97, respectively) and GMP-140 levels (13.37±1.80 vs.13.41±1.60, p=0.95) between group A (3 mg/kg/day aspirin) and group B (5 mg/kg/day aspirin) (Table 5).
Discussion
Platelets played a prominent role in preventing blood loss in reaction to vascular injury, but they also served as a mediator in the process of pathologic thrombosis. Platelet activation is stimulated by combining with platelet secretion products and local prothrombotic factors, which can promote aggressive PAG, vasoconstriction, and activation of the coagulation system (Brass, 2010). Multiple pathways lead to platelet activation, including those stimulated by dense granules (ADP, serotonin) and alpha granules (thromboxane A2, vWF, FV, FXIII, fibrinogen) (Angiolillo et al., 2010). Platelet shape change, expression of proinflammatory cytokines such as P-selectin, and platelet procoagulant activity expression can induce PAG and become the potential reasons for pathologic thrombosis (Varga-Szabo et al., 2008). Appropriate platelet activation inhibits the extent of blood loss following injuries of blood vessels and promotes wound healing without resulting in vascular occlusion, whereas inappropriate platelet activation leads to arterial occlusion, ischemia, and soft tissue injury (Smyth et al., 2009). Thus, detection of the degree of PAG and platelet activation is very important for patients after operation on vessels of the heart. The GMP-140, also named P-selectin, is a specific marker of PAG and a member of the selectin family, presenting in the α granular membrane of the platelet (Chen and Geng, 2006). The serum level of GMP-140 is very low in normal cases, whereas once platelet activation has occurred, GMP-140 translocates to the surface of activated platelets or releases into plasma, suggesting that detection of GMP-140 serum level can reflect the degree of platelet activation and the thrombophilia (Ay et al., 2008).
In the present study, we found that the rates of PAG in the immediate postoperative ASD/VSD occlusion were significantly higher than those in the preoperative ASD/VSD occlusion and that there existed a significant increase in GMP-140 levels after ASD/VSD occlusion in contrast with those before ASD/VSD occlusion. This particular mechanism of elevated GMP-140 expression and cleavage following activation makes this molecule apparently resistant to ex vivo activation, provided that plasma is immediately separated from the cellular component (Woollard et al., 2008; Kajimoto et al., 2009). Furthermore, serum levels of GMP-140 do not seem to be influenced by different anticoagulants or varying methods of plasma preparation, indicating that the serum level of GMP-140 can be used as a reliable marker of in vivo platelet activation (van der Zee et al., 2006; Ferroni et al., 2009). To be consistent with the present study, a study conducted by Ferroni et al. (2009) found that following platelet activation, GMP-140 is expressed on the surface membrane and then shed by cleavage; thus, the determination of GMP-140 has been proposed as a useful marker of in vivo platelet activation. GMP-140 serum levels of CHD patients who suffered from ASD/VSD occlusion were decreased significantly in the four postoperative days when compared with the immediate preoperative periods. It has been reported that the implantation of occluders could lead to aggressive PAG that would last for a shorter interval and then return to a normal level due to the endothelialization of occluder devices, which begins from 7 days to 3 months after occluder implantation (Connell et al., 2007; Zeng et al., 2010).
Moreover, we also found that the immediate postoperative GMP-140 levels in the VSD occlusion patients were significantly higher compared with ASD occlusion patients. This result may possibly be correlated with longer operative time and severe endangium injury of VSD occlusion, whereas patients treated with VSD occlusion need multiple radiography and so on (Li et al., 2008; Morgan et al., 2010). In our study, the GMP-140 serum level was increased after ASD and VSD occlusion, suggesting that patients who underwent these surgeries need antiplatelet therapy, which is the basis of oral anticoagulation and aspirin after VSD or ASD occlusion (Majunke et al., 2009). In addition, our study also indicated that the immediate postoperative GMP-140 levels in VSD/ASD occlusion patients were positively associated with the operation time. We believe that the possible causes of this result may be that we only observed the short-term outcomes of the GMP-140 level in VSD and ASD occlusion, but have no follow-up studies for the platelet activation state. It can be indicated that the length of operation time may play an important role in determining the antiplatelet therapy for patients who underwent VSD or ASD occlusion, especially in the short term after VSD/ASD occlusions.
Aspirin is one of the most widely used drugs worldwide for the prevention of thrombotic cardiovascular events; it has an antiplatelet effect by inhibiting the production of thromboxane and can prevent the formation of the platelet activating factor thromboxane A2 (Cholette et al., 2010). Because the platelet patch can become too large and block the blood flow, aspirin can be used at low doses for a long term, to prevent cardiovascular diseases, strokes, and blood clot formation in people at high risk of developing blood clots (Gasparyan et al., 2008; Mehta, 2009). Aspirin exerts its antithrombotic effect to restrain PAG by decrease of the activity of the platelet, which largely owes to its irreversible inactivation of cyclooxygenase, resulting in impaired platelet function (Yasuda et al., 2008). As mentioned in the paragraph above, CHD patients may suffer from an aggressive PAG and elevated GMP-140 serum level after the ASD or VSD occlusion surgeries, so those patients need to receive anticoagulant drugs, such as aspirin, for the prevention of vascular occlusion. In line with previous studies, our study also have found that patients may have a trend of decreased GMP-140 serum levels after ASD or VSD occlusion surgeries after the treatment of aspirin, indicating that aspirin can inhibit the rates of PAG and reduce the risk of thrombogenesis (Dunning et al., 2008). However, patients who received aspirin often suffer from some undesirable side effects, including gastrointestinal ulcers, stomach bleeding, and tinnitus, especially in higher doses. In this regard, many researchers have paid more attention to find the proper dosage of aspirin that patients were taking for maximum efficacy or safety (Serebruany et al., 2005; Gurbel et al., 2007). In the current study, we found that the dose of aspirin, both 3 and 5 mg/kg/day, has significant effects on reducing the serum level of GMP-140 and inhibiting the PAG in patients after the VSD or ASD occlusion surgery. Consistent with our observed results, a previous study has also demonstrated that lower dose of aspirin can also inhibit the PAG and support greater safety and less side effects for patients (Steinhubl et al., 2009).
In conclusion, CHD patients had a significant increase in GMP-140 levels after ASD or VSD occlusion, but the immediate postoperative GMP-140 levels in the VSD occlusion patients were significantly higher compared with ASD occlusion patients, suggesting that the phenomenon of platelet activation is more obvious after VSD occlusion than ASD occlusion. Furthermore, oral administration of aspirin can possibly inhibit platelet activation after ASD or VSD occlusion, and both daily oral administration of 3 and 5 mg/kg/day aspirin can induce a significant decrease in PAG of patients after VSD/ASD occlusion. The value of this study is not only in evaluating the serum level of GMP-140 in CHD patients who underwent ASD or VSD occlusion but also in providing a proper drug therapy with aspirin in preventing embolism thrombogenesis for patients after VSD/ASD occlusion.
Footnotes
Acknowledgments
The authors would like to acknowledge the reviewers for their helpful comments on this article.
Author Disclosure Statement
The authors have declared that no competing interests exist.