
Abstract
Type 2 diabetes (T2DM) is a noncommunicable disease affecting huge populations in India and abroad. Single-nucleotide polymorphisms (SNPs) in CD36, a macrophage scavenger receptor, have been implicated in the pathogenesis of T2DM and its complications. Eleven SNPs in the CD36 gene and their association with 100 each of control subjects and T2DM patients were investigated in the present study. The haplotype analysis of a few significant SNPs was carried out in individuals from families with diabetic history to evaluate its utility in disease prediction. Polymerase chain reaction-restriction fragment length polymorphism was used for genotyping. Ten families with a family history of diabetes were identified and blood samples were collected from as many family members as possible. Genotyping of three SNPs, namely rs1761667 (G>A) in exon 1 A, rs3211938 (T>G) in exon 10, and rs3212018 (16 bp del) in exon 14, was performed in all samples. Our results suggested that individuals having a GATTC1 haplotype might be at risk of developing T2DM (p<0.001) and, therefore, might be susceptible to related complications. Moreover, the presence of A, G, and G alleles of SNPs rs1761667 (G>A), rs3211938 (T>G), and rs1984112 (T>G) tends to have increased BMI, respectively. Such studies may be helpful for disease prediction in individuals at risk of T2DM. The predictive potential of CD36 variants can be explored with more families in the study population to use this as a genetic marker.
Introduction
T
The CD36 gene is located in chromosome 7 at locus q11.2 with 17 exons and 16 introns, which cover approximately 36 Kb region of DNA (Silverstein et al., 1992). CD36 is a plasma membrane glycoprotein constituted by a single 88-kDa polypeptide chain of 472 amino acid residues (Greenwalt et al., 1992; Gautam and Banerjee, 2010). CD36 is widely distributed in a variety of cell types especially on macrophages, monocytes, platelets, adipocytes, etc. CD36 plays a major role in adhesion of ligand, uptake of fatty acids, and signal transduction. In obesity and hyperlipidemia, these ligands affect inflammatory and insulin signaling pathways in a pathophysiological response using CD36 (Kennedy et al., 2011). In macrophages, the uptake of fatty acids especially the oxidized form of low-density lipoprotein (Ox-LDL) leads to foam cell formation, plaque formation, and ultimately atherosclerosis. Since lipid metabolism is closely associated with diabetes and, in turn, atherosclerosis, the study of the CD36 locus was undertaken. Several studies on gene variants were undertaken (Banerjee et al., 2010; Gautam et al., 2011, 2013a, 2013b; Rać et al., 2012), which led to our investigation of selected CD36 single nucleotide polymorphisms (SNPs) and haplotypic association with T2DM in a North Indian population.
Materials and Methods
Study design and participants
The case-control study was approved by the Institutional Ethics Committee (King George's Medical University, Lucknow, India), and informed consent was obtained from all participants. Medical records of all patients were reviewed to ascertain diabetes-associated complications. The study subjects selected according to the inclusion and exclusion criteria (Gautam et al., 2013a) were >40 years of age.
Technical information
SNP selection and genetic analysis
Genomic DNA was extracted from blood samples of T2DM patients and controls (n=100 each), using the salting-out method with slight modifications and checked on 1% agarose gels (Miller et al., 1988; Gautam et al., 2011). The quality and quantity of DNA were estimated using a biophotometer (Eppendorf).
Eleven SNPs, namely rs1984112, A>G in exon 1A; rs1761667, −31118G>A in 5′ promoter region of exon 1A; −178A>C in promoter region; rs1527479, C>T in intron IB; 478C>T in exon 4; AC dinucleotide del in exon 5; rs3211938, 1264T>G in exon 10; Ins 1159A at 317 codon in exon 11 (CI962235); rs1527483, 25444C>T in intron 11; rs3212018, 16 bp del in exon 14; and rs1049673 G>C in exon 15, were identified in the CD36 gene after surveying literature and SNPdb (Table 1). The sample size for each SNP was determined using QUANTO software (v.1.2.1) after genotyping 100 control individuals and minor allele frequencies (MAFs) were calculated. SNPs with MAF≥0.01 were included in the haplotype analysis. SNPs were genotyped using polymerase chain reaction and restriction fragment length polymorphism (PCR-RFLP) (Banerjee et al., 2010).
MAF, minor allele frequency; SNP, single-nucleotide polymorphism.
Statistical analysis
Comparison of all clinical parameters between controls and T2DM patients was carried out by the t-test. Allelic and genotypic frequencies along with carriage rates of polymorphic alleles in patient and control groups were evaluated by Pearson's chi-square (χ2) test/Fisher's exact test. The Hardy-Weinberg equilibrium at individual locus was assessed by chi-square (χ2) statistics using SPSS software (v. 15.0). All p-values<0.05 were considered statistically significant. The odds ratio (OR) at 95% confidence interval (CI) was determined to describe the strength of association by the logistic regression model.
Haplotype analysis
Haplotype analysis was performed for all six SNPs whose MAF ≥0.01. The SNPs taken were G>A (rs1761667), C>T (rs1527483), A>G (rs1984112), C>T (rs1527479), T>G (rs3211938), and 16 bp del (rs3212018). Multivariate logistic regression analysis was carried out to analyze haplotypes. Pairwise linkage disequilibrium (LD) based on D′ statistic for the six SNPs was calculated using SHEsis software. LD blocks were defined using their default algorithm (Shi and He, 2005).
Pedigree analysis
Ten families with a family history of diabetes were identified and blood samples were collected from the available family members and DNA was extracted. The three SNPs, namely rs1761667 (G>A) in exon 1 A, rs3211938 (T>G) in exon 10, and rs3212018 (16 bp del) in exon 14, which showed significant association with T2DM in the North Indian population (Banerjee et al., 2010; Gautam et al., 2011, 2013a, 2013b), were genotyped in all individuals by PCR-RFLP. The biochemical profile of each individual was correlated with their genotypes.
Results
Prevalence of the disease was taken as 3.0% and power of the study as 80.0%. The biochemical analysis in patients (n=450) and controls (n=400) has been reported earlier (Gautam et al., 2011).
Genetic analysis
Out of eleven SNPs studied, five, namely −178A>C in promoter region; 478C>T in exon 4; AC dinucleotide del in exon 5; Ins 1159A at 317 codon in exon 11 (CI962235); and rs1049673 G>C in exon 15, were monomorphic (MAF<0.01) and therefore were not analyzed further (Table 1). Polymorphic studies of the remaining six SNPs (rs1984112, rs1761667, rs1527479, rs3211938, rs1527483, and rs3212018) in controls and patients (n=100 each) showed them to be in the Hardy-Weinberg equilibrium.
The GA heterozygous genotype of the promoter polymorphism G>A (rs1761667) in the CD36 gene was more prevalent in T2DM patients and showed an association with T2DM in the North Indian population (Banerjee et al., 2010). However, TG genotype of SNP T>G (rs3211938) had a mild significance (p=0.045) and seemed to confer susceptibility to T2DM (Gautam et al., 2013a). We also analyzed CI962235 (Ins1159A) and rs3212018 (16 bp del) SNPs, but did not observe any significant association (Gautam et al., 2013b).
Haplotype analysis
Analysis of six SNPs taken together, that is, rs1984112 (A>G), rs1761667 (G>A), rs1527479 (C>T), rs3211938 (T>G), rs1527483 (C>T), and rs3212018 (16 bp del) showed thirty-four different combinations of haplotypes. Among them, the G A T T C 1* showed the highest significant association (p<0.001) with T2DM (OR: 6.606 [2.443-17.861]). Moreover, few other haplotypic combinations also showed significant association with T2DM (p<0.05) (Table 2).
Significance of bold values is to show the haplotypes whose p-values are <0.05.
Haplotype with significant p-value and high odds ratio.
The LD patterns according to the position of variants within the gene, which showed the strongest statistical significance of LD between two SNPs, were rs3211938 (T>G): rs1527483 (C>T) (frequency=0.725; p<0.01); however, a few other SNP combinations also showed a high significant association with T2DM [rs1527479 (C>T): rs3211938 (T>G) (frequency=0.702; p<0.01) and rs1761667 (G>A): rs3211938 (T>G) (frequency=0.728; p<0.01)] (Fig. 1).
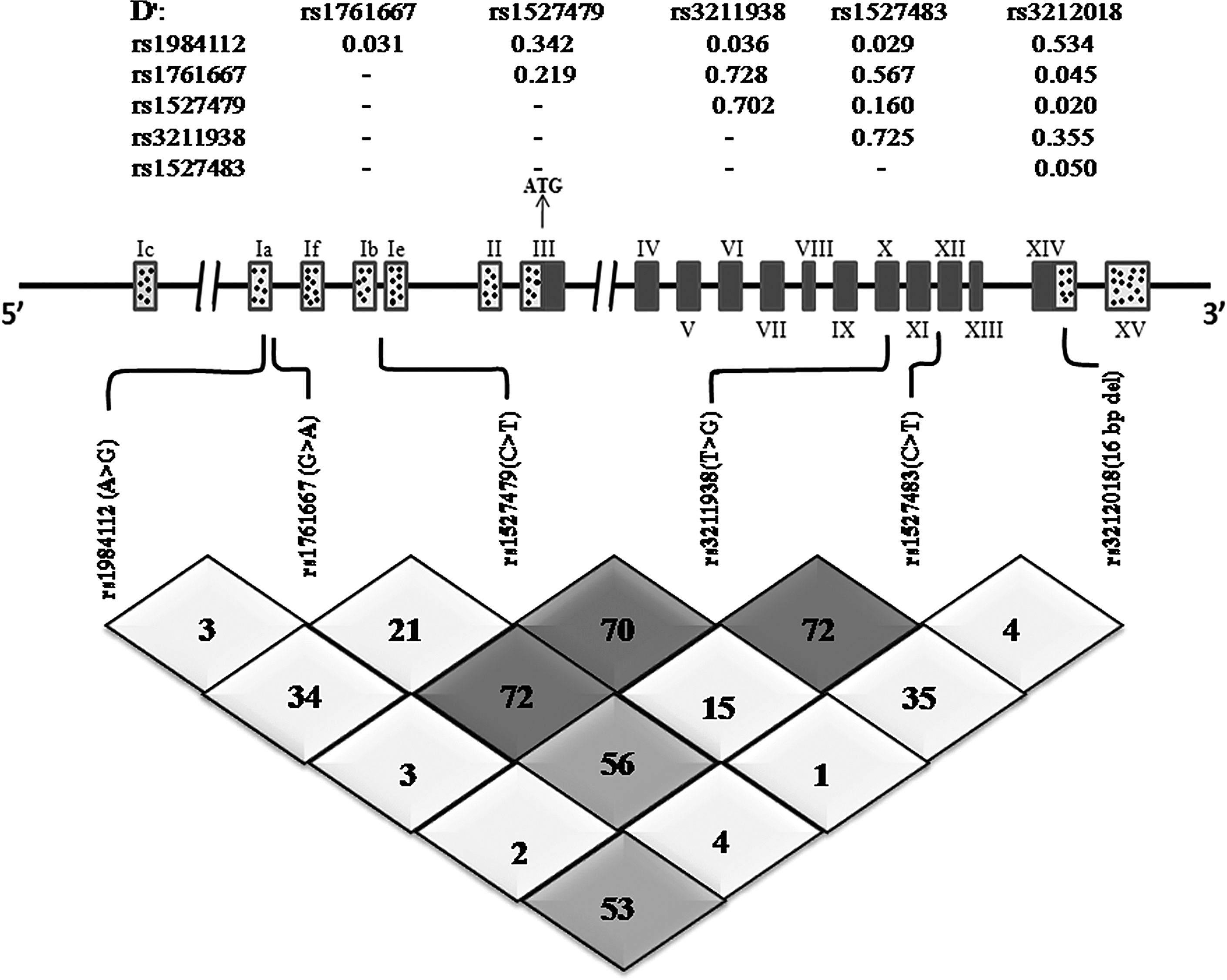
Linkage Disequilibrium (D′) of six single-nucleotide polymorphisms in the CD36 gene in a North Indian population with T2DM. Pairwise LD in subjects is represented as dark gray squares for strong LD, and light gray squares for little or no LD, linkage disequilibrium; T2DM, type 2 diabetes mellitus.
Pedigree analysis
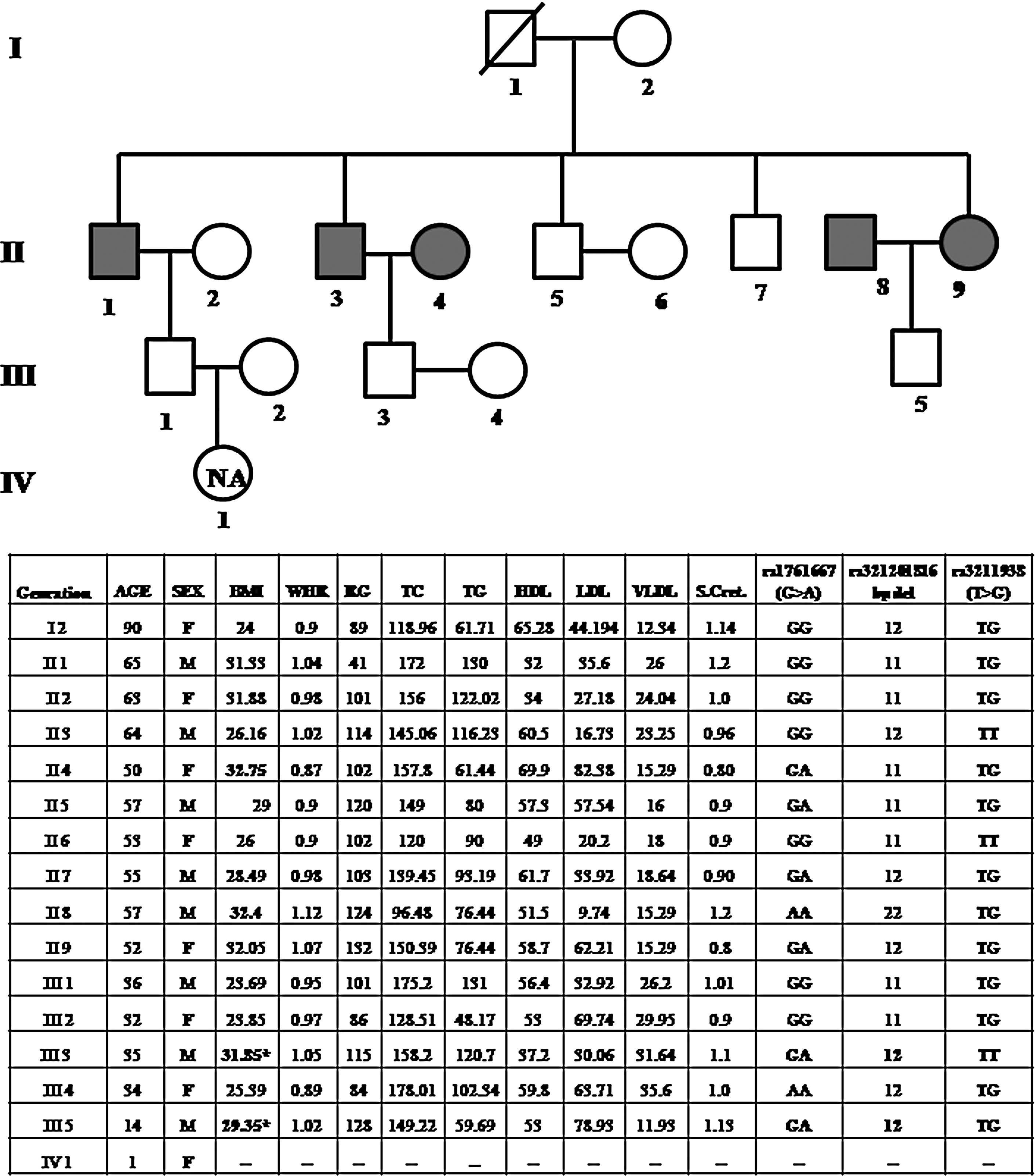
The three SNPs reported earlier showed similar results in family studies. Out of 10, one large family has been described, in which subjects II-1, II-3, II-4, II-8, and II-9 were diabetic at the time of sample collection (Fig. 2). The individuals II-1, II-3, and II-9 were related and all were between 50 and 65 years of age (Fig. 2). Their random glucose levels were 41, 114, 102, 124, and 132 mg/dL, respectively. Most of the individuals of the family were heterozygous GA and TG for the SNPs rs1761667 (G>A) and rs 3211938 (T>G), respectively. Those individuals who have the A allele of rs1761667 and the G allele of rs3211938 have a higher BMI than other members, for example, II-4, II-8, and II-9. It was also observed that some individuals who were not yet diabetic but possessed similar alleles showed a higher BMI (II-5, II-7, III-3, and III-5).
Pedigree analysis: A family with four generations
Discussion
CD36 recognizes and binds to specific Ox-LDL and initiates an intracellular signaling cascade in macrophages. Its uptake finally leads to the formation of plaques and atherosclerosis (Gautam and Banerjee, 2010). A substantial number of studies have investigated the association of CD36 with certain disorders such as abnormal serum LDLs (Goyenechea et al., 2008; Morii et al., 2009), fatty acids (Ma et al., 2004), coronary artery disease (Doris, 2002; Kuang et al., 2004; Ma et al., 2004; Yun et al., 2007), left ventricular mass (Arnett et al., 2009; Hall et al., 2011), metabolic syndrome (Leprêtre et al., 2004; Noel et al., 2010), insulin resistance (Heilbronn et al., 2007; Kashyap et al., 2009), low adiponectin levels (Leprêtre et al., 2004), and stroke (Ikram et al., 2009). Recent studies on a Chinese population showed the association of CD36 gene variants with triglycerides and high-density lipoprotein (Chien et al., 2012). Another study reported a significant polymorphic association of the CD36 gene with essential hypertension and systolic blood pressure in a Chinese population (Liu et al., 2013). Our results suggested that individuals having a GA genotype might be susceptible to T2DM and may be at risk of developing related complications (Banerjee et al., 2010). A few of our other studies have also suggested the role of CD36 variants in the development of T2DM (Gautam et al., 2013a, 2013b).
These alleles may also act as a genetic marker in early age diagnosis of T2DM such as subject III-5 in our family study. At present, he is only 14 years of age and has heterozygous genotypes GA and TG of rs1761667 (G>A) and rs3211938 (T>G), respectively (Fig. 2), and an increased BMI, which might indicate a high risk of developing T2DM in the future.
Moreover, the presence of the G allele in the TG genotype of SNP T>G (rs3211938) and the G allele of SNP T>G (rs1984112) appeared to be indicators of increased BMI and, therefore, can be used as a markers for early prediction of T2DM. Another interesting finding from haplotype studies was that individuals with
The genotype results led to the conclusion that CD36 variants have a high predictive potential on determining the disease susceptibility in the North Indian population. However, further follow-up studies are essential to determine what changes occur at molecular levels for these SNPs, which may help in correct diagnosis and treatment of T2DM.
Footnotes
Acknowledgments
The authors would like to thank the Department of Biotechnology (DBT), the Department of Science & Technology (DST), the Indian Council of Medical Research, New Delhi, India, and the Centre of Excellence, Higher Education, Government of Uttar Pradesh, Lucknow, India, for funding the work. SG would like to acknowledge the Rajiv Gandhi National Fellowship, University Grants Commission, New Delhi, India.
Author Disclosure Statement
No competing financial interests exist.