
Abstract
Objective: To investigate the relationship between matrix metalloproteinase 9 (MMP-9) gene polymorphism and the efficacy of glucocorticoid therapy in idiopathic pulmonary fibrosis (IPF) patients. Methods: We conducted a case-control study. Between January 2013 and September 2014, 115 patients at the Nine Department of Respiratory Medicine, Nanjing Chest Hospital, diagnosed with IPF were enrolled to be the IPF group and 100 healthy subjects were enrolled to be the control group. Prednisone was used to treat IPF patients. Polymerase chain reaction-restriction fragment length polymorphism was used to identify MMP-9 1562C> T polymorphism. The Sandwich enzyme-linked immunosorbent assay was used to measure the serum level of MMP-9 and tissue inhibitor of metalloproteinases 1 (TIMP-1) in the IPF patients before and after the glucocorticoid treatment. Results: The frequencies of the TT genotype and the T allele of MMP-9 1562C> T gene were found significantly higher in the IPF group compared with the control group (both p < 0.05). Serum levels of MMP-9 and TIMP-1 in IPF patients in each of the three genotype groups before glucocorticoid treatment were significantly higher than those in the control group (all p < 0.05). After the glucocorticoid treatment, MMP-9 and TIMP-1 levels decreased significantly compared with the levels before the glucocorticoid treatment in the IPF patients in each genotype group (all p < 0.05), but were still higher than those in the control group (all p < 0.05). The proportion of “remarkable effect” in the IPF patients of the CC genotype group was significantly higher than that in the other two genotype groups, while the rate of adverse reactions of the CC group was significantly lower than the other two groups (all p < 0.05). Conclusion: MMP-9 gene 1562C> T polymorphism may affect the efficacy of the glucocorticoid therapy for IPF and may be a predictor of IPF treatment outcome.
Introduction
I
As a chronic, progressive lung disease, IPF is caused by the histopathologic and/or radiological patterns of usual interstitial pneumonia (Idiopathic Pulmonary Fibrosis Clinical Research et al., 2014). IPF might be caused by the aberrant activation of alveolar epithelial cells, excessive accumulation of inflammation cells, proliferation of fibroblasts, and exaggerated deposition of extracellular matrix and finally leads to the destruction of lung parenchyma (Idiopathic Pulmonary Fibrosis Clinical Research et al., 2014).
A number of medications have been developed to treat IPF, including antioxidants (N-Acetylcysteine), inhibitor of tyrosine kinases (BIBF 1120, also known as nintedanib), ambrisentan, and anticoagulants (Richeldi et al., 2011; Raghu et al., 2013; Idiopathic Pulmonary Fibrosis Clinical Research et al., 2014; Richeldi et al., 2014). The glucocorticoid therapy was recommended by recent studies. The glucocorticoid therapy has been used to treat many respiratory diseases and has been suggested by international guidelines and systematic reviews in the management of acute exacerbations of chronic obstructive pulmonary disease (30-40 mg of oral prednisolone for 10-14 days) (Leuppi et al., 2013). In addition, inhaled glucocorticoids have also been widely prescribed to control asthma (Tantisira et al., 2011).
Matrix metalloproteinases (MMPs), also known as matrixins, belong to a large family of peptidases that consists of 23 members. MMPs were found to be associated with tissue remodeling, cell behavior, survival, and death (Checa et al., 2008). A recent study demonstrated that a number of MMPs, such as MMP-1, MMP-2, MMP-3, MMP-7, MMP-8, MMP-9, MMP-12, and MMP-13, are upregulated in the abnormal remodeling that characterizes IPF (Checa et al., 2008).
MMP-9 is expressed in a variety of cells, including alveolar epithelial cells and neutrophils and fibroblasts in fibroblastic foci, which could be part of the fibrogenic positive feedback loop (Pardo and Selman, 2012). Thus, MMP-9 gene polymorphisms regulating the expression of MMP-9 might relate with the development of IPF. It was proved that the glucocorticoid therapy could inhibit the production of MMPs in many other parts of the body in addition to lungs (Cincik et al., 2013). Thus, in pediatric inflammatory bowel disease, serum MMP and tissue inhibitor of metalloproteinase 1 (TIMP-1) levels are used to measure glucocorticoid therapy response (Makitalo et al., 2012).
In our study, for the first time, we aimed to investigate the relationship between MMP-9 gene polymorphisms and the efficacy of the glucocorticoid therapy for IPF. Prednisone, member of the glucocorticoid family, was used to treat IPF patients. Polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) was used to identify MMP-9 1562C> T polymorphism, and the sandwich enzyme-linked immunosorbent assay (ELISA) was used to measure the serum levels of MMP-9 and TIMP-1 in IPF patients before and after the glucocorticoid therapy.
Materials and Methods
Study subjects
Between January 2013 and September 2014, 115 IPF patients at the Nine Department of Respiratory Medicine, Nanjing Chest Hospital, were enrolled to be the IPF group. Among them, there were 67 male and 48 female (mean age, 58.1 ± 11.4 years; mean body mass index [BMI], 21.49 ±2.02) with a mean smoking index ([Number of cigarette/day] × [years of smoking history]) of 338. Patients sensitive to hormone contraindications were excluded.
More than 50% of the patient diagnoses were confirmed by lung biopsy. Bronchoscopy lung biopsy showed slightly widened alveolar septum, inflammatory cell infiltration, and type II alveolar epithelial cell hyperplasia. Fusiform proliferated fibroblasts were observed in the lightly stained myxoid matrix. A long axis of fibroblasts parallel to the alveolar septa was also observed, indicating ongoing fibrosis rather than past damage caused by pathological changes, which was consistent with pathological changes of fibrosis. In the absence of biopsy, patients had to fulfill the criteria of the ATS/ERS international consensus, which required patients to meet the following four major criteria and at least three of the four minor criteria (Wells, 2013).
The main criteria were as follows: (1) no other known causes of interstitial lung disease; (2) restrictive ventilatory defect and/or pulmonary gas exchange barrier; (3) high-resolution computed tomography that showed reticular opacities at the bottom of the lungs; and (4) bronchoscopic lung biopsy or bronchoalveolar lavage that showed no evidence of other diseases. The minor criteria were as follows: (1) age >50 years; (2) insidious onset and respiratory diseases after activity; (3) duration ≥3 months; and (4) lung crackles appearing at the bottom of the lungs. All the enrolled IPF patients underwent regular examinations of blood, urine, liver, kidney and lung functions, blood gas analysis, and lung computed tomography pathology.
All the IPF patients received the glucocorticoid therapy and were orally administrated 0.5-1.0 mg/kg/d prednisone. After the daily administration for 4-8 weeks, serum specimens of patients before and after the treatment were collected. Another 100 healthy volunteers were treated as controls, including 55 males and 45 females (mean age, 57.2 ± 5.5 years old; mean BMI, 21.11 ± 2.05) with a smoking index of 304. No obvious clinical symptoms were observed. No heart, brain, lung, liver, and kidney disease histories were found; the results of electrocardiogram, lung function, and X-ray were all normal.
MMP-9 1562C> T gene polymorphism identification
All subjects were fasted, and 5 mL forearm blood was collected from each subject in the morning, with EDTA added for the anticoagulant. The blood sample was centrifuged at 2700 rpm/min for 10 min at room temperature, and the cell layer was collected and stored at −80°C. DNA was extracted using the blood genome DNA extraction kit (Shanghai Sangon Biotechnology Co., Ltd.).
PCR-RFLP was used to identify gene polymorphisms, and the primer sequences for MMP-9 1562C> T amplification are shown in Table 1. PCR system (20 μL): 2.0 μL forward and reverse primers, 2.0 μL DNA template, 0.5 μL 4 × dNTP, 2.0 μL 10 × Taq buffer, 0.2 μL Taq polymerase, 2 μL PCR fuel, 11.3 μL ultrapure water. The amplification reaction system was centrifuged and covered with liquid paraffin. PCR protocol: 94°C for 5 min, 30 cycles of denaturation at 94°C for 45 s, annealing at 56°C for 60 s, and extension at 72°C for 50 s. After PCR, PCR products were digested with the BbUI enzyme for 16 h at 37°C. Finally, 2% agarose gel electrophoresis was conducted to obtain the corresponding 1562C> T genotyping results.
SNP, single-nucleotide polymorphism; MMP-9, matrix metalloproteinase-9.
Serum MMP-9 and TIMP-1 protein concentrations
Double antibody sandwich ELISA was used to measure the concentrations of the serum MMP-9 and TIMP-1 protein. Commercially available ELISA kits for MMP-9 and TIMP-1 were purchased from R&D Systems Europe Ltd. and were used according to the manufacturer's instructions. Diluted avidin-peroxidase complex and tetramethylbenzidine (TMB) substrate were prebalanced at 37°C for 30 min. Standard samples (100 μL) with a protein concentration of 10,000, 5000, 2500, 1250, 625, 312, or 156 pg/mL were respectively added to the seven wells in a row.
A 100 μL sample diluent was added to another well called the zero well. Study samples (10 μL) were added to rest of the wells, each with a 90 μL diluent added (dilution ratio of 1:10). ELISA plates were sealed with lids and reacted at 37°C for 90 min. Liquids in the ELISA plates were dried with absorbent paper. 0.1 mL prepared anti-human MMP-9 antibody combined with 0.1 mL anti-human TIMP-1 antibody was added to each well to react at 37°C in the dark for 60 min. Each well was washed with 0.01 M PBS thrice and soaked for 1 min. 0.1 mL prepared avidin-peroxidase complex was added to each well and reacted at 37°C in the dark for 30 min. Each well was washed with 0.01 M PBS five times and soaked for 1 min. Ninety microliters of balanced TMB was added successively into each well and reacted at 37°C in the dark for 25-30 min.
The reaction should be terminated when visible blue gradient solutions were observed in the ELISA plates. Then, 0.1 mL TMB solution was added to terminate the reaction, and the blue solution turned into yellow solution. The microplate reader was used to measure absorbance (OD value) at 450 nm. The zero well was used as a control well. By comparing the sample absorbance values with the seven standard samples and the control, we obtained the concentration of each sample. Absorbance value was set as x-axis and concentration value was set as y-axis.
Efficacy determination
Clinical efficacy was categorized as follows: glucocorticoid therapy had a “remarkable effect” on IPF patients if the patients did not have symptoms such as cough, dyspnea after activities, cyanosis, or high-pitched lung crackles at the end of the study; glucocorticoid therapy had a “moderate effect” on IPF patients if the patients with paroxysmal did not have severe cough, did not have dyspnea at the resting state or cyanosis after moderate activity, and had no lung crackles at the end of the study; glucocorticoid therapy had “no effect” on IPF patients if the patients experienced no improvement after treatment (Wells, 2013).
Statistical methods
SPSS 20.0 was used for data analysis. The deviation from the Hardy-Weinberg genetic equilibrium was analyzed using χ2 goodness-of-fit tests, and p < 0.05 was regarded as statistically significant. Numerical data are presented as mean ±standard deviation and were tested using the t-test. Categorical data were presented as a percentage or rate and were tested using the χ2 test. Odds ratio (OR) and 95% confidence intervals (95% CI) were calculated to measure the association between IPF occurrence and various genotypes. In all the analyses of this study, p < 0.05 was considered to be statistically significant.
Results
Baseline characteristics
The baseline characteristics of the control group and the IPF group are shown in Table 2. There was no significant difference in age, gender ratio, BMI, smoking index, or smoking status between the control group and the case group (all p > 0.05).
IPF, idiopathic pulmonary fibrosis; BMI, body mass index.
Genotype analysis
MMP-9 PCR products were initially identified using agarose electrophoresis; amplified specific fragments with a size of 435 bp were successfully obtained. After being digested by the restriction enzyme BbUI, there was one fragment (435 bp) in the wild-type (C/C genotype), three fragments (435, 247, and 188 bp) in the heterozygous type (C/T genotype), and two fragments (247 and 188 bp) in the homozygous type (T/T genotype) (Fig. 1).
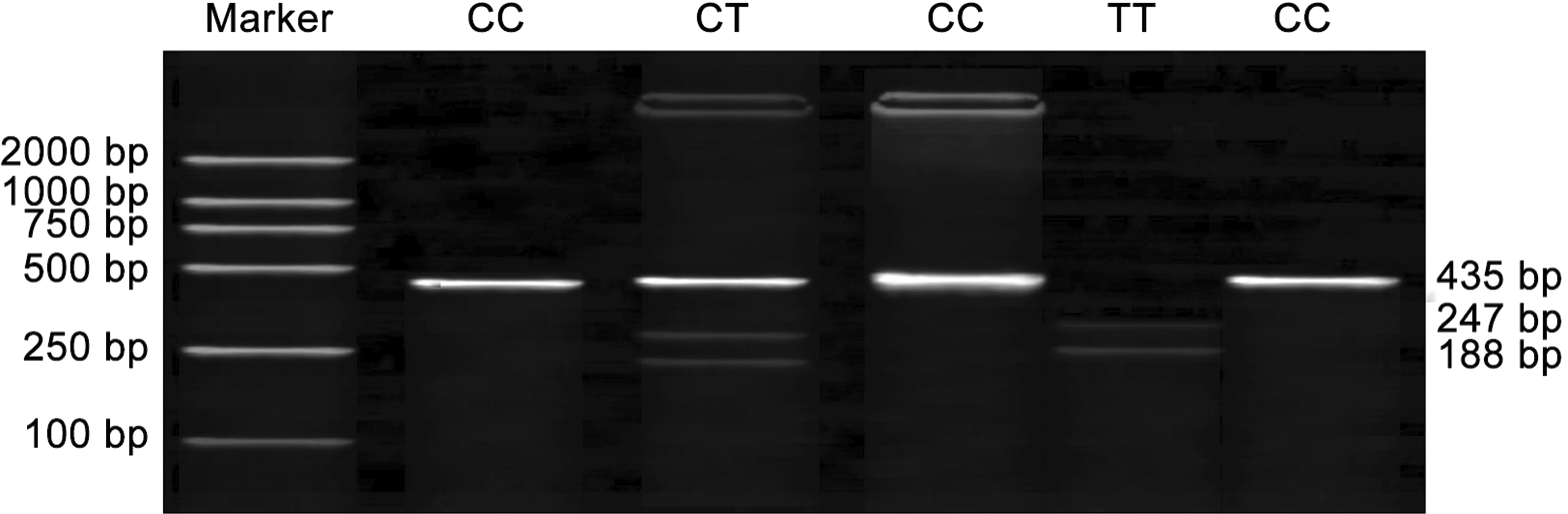
Electrophoresis of MMP-9 gene 1562C>T polymorphism (There was one fragment in the C/C genotype, three fragments in the C/T genotype, and two fragments in the T/T genotype). MMP-9, matrix metalloproteinase-9.
MMP-9 genotype and allele frequency distribution
The χ2 goodness-of-fit test indicated the Hardy-Weinberg genetic equilibrium in both the IPF group and the control group (both p > 0.05). The TT genotype and T allele frequencies of MMP-9 1562C> T gene polymorphism in the IPF group were significantly higher than those in the control group (both p < 0.05), indicating that the T allele may be a risk factor for IPF occurrence (TT vs. CC: OR = 3.571, 95% CI = 1.355-9.411; TT + CT vs. CC: OR = 1.929, 95% CI = 1.072-3.471; C vs. T: OR = 1.624, 95% CI = 1.040-2.536) (Table 3).
OR, odds ratio; CI, confidence interval.
Serum MMP-9 and TIMP-1 protein levels and MMP-9/TIMP-1 ratio
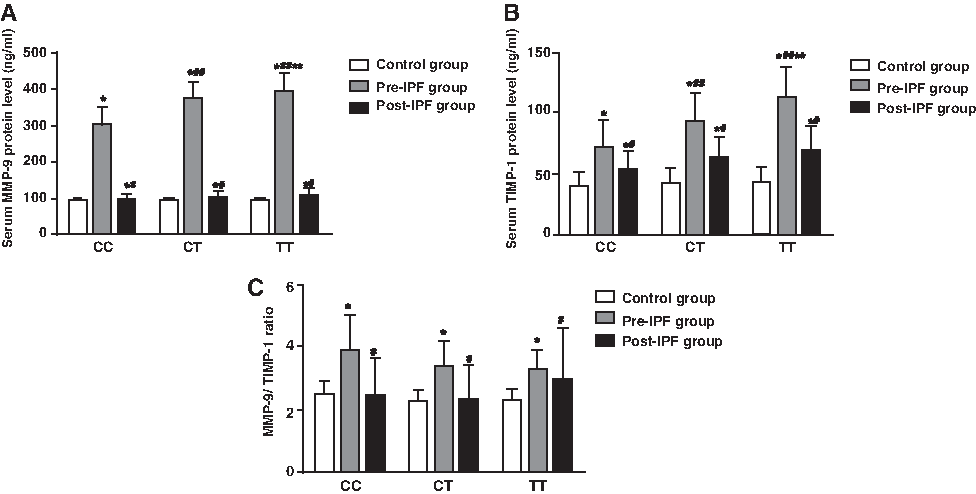
Serum MMP-9 and TIMP-1 levels of the IPF patients in each genotype group before the glucocorticoid therapy were significantly higher than those of the controls (all p < 0.05). After the treatment, MMP-9 and TIMP-1 levels in all the three genotype groups decreased significantly (all p < 0.05), but were still higher than those in the control group (all p < 0.05). Before the treatment, serum levels of MMP-9 and TIMP-1 increased in the order of CC, CT, and TT genotype, with significant difference among the three genotypes (all p < 0.05) (Table 4, 5).
Compared with the control group, p < 0.05.
Compared with the pre-IPF group, p < 0.05.
Compared with patients with CC genotype in the same group, p < 0.05.
Compared with patients with CT genotype in the same group, p < 0.05.
Pre-IPF group, IPF group before therapy; Post-IPF group, IPF group after therapy.
Compared with the control group, p < 0.05.
Compared with the pre-IPF group, p < 0.05.
Compared with patients with CC genotype in the same group, p < 0.05
Compared with patients with CT genotype in the same group, p < 0.05.
TIMP-1, tissue inhibitor of metalloproteinases-1.
MMP-9/TIMP-1 ratio in the IPF patients before the treatment was significantly higher than that in the IPF patients after the treatment as well as the control group (both p < 0.05). However, there was no significant difference in MMP-9/TIMP-1 ratio between the control group and the IPF patients after the treatment (p > 0.05). In addition, there was no significant difference in MMP-9 level, TIMP-1 level, or MMP-9/TIMP-1 ratio between the control group and the IPF patients in each genotype group after the treatment (all p > 0.05) (Table 6 and Fig. 2).
Serum protein levels of MMP-9 and TIMP-1 and ratio of MMP-9/TIMP-1 in the control group, Pre-IPF group, and Post-IPF group with different genotypes
Compared with the control group, p < 0.05.
Compared with the pre-IPF group, p < 0.05.
Efficacy differences after glucocorticoid therapy
In the CC genotype group, the proportion of the IPF patients on whom the treatment had a remarkable effect with regard to cough, dyspnea, cyanosis, and lung crackles was significantly higher than the patients in the CT group and the TT group (all p < 0.05). However, there was no significant difference in the proportion of “remarkable effect” between the CT group and the TT group (all p > 0.05) (Table 7 and Fig. 3).
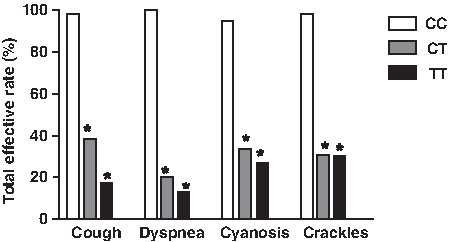
Total effective rate after glucocorticoid therapy in IPF patient with different genotypes (%). *compared with the CC genotype, p < 0.05.
Compared with the CC genotype, p < 0.05.
Drug adverse reactions after glucocorticoid therapy
IPF patients in the CT group and the TT group had a significant higher incidence of ostealgia, muscle atrophy, and depression than those in the CC group (all p < 0.05). However, no significant difference was found in the incidences of hypertension, gastrointestinal bleeding, or other adverse reactions among the three genotype groups (all p > 0.05) (Table 8 and Fig. 4).
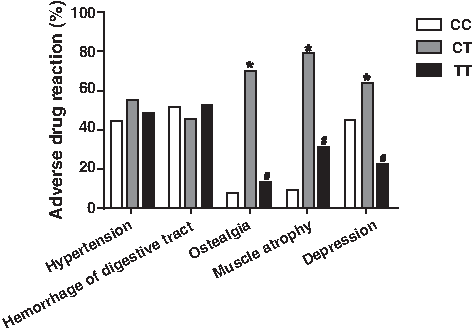
Drug adverse reaction rate after glucocorticoid therapy in IPF patient with different genotypes (%). *Compared with the CC genotype, p < 0.05; #compared with the CT genotype, p < 0.05.
Compared with the CC genotype, p < 0.05.
Compared with the CT genotype, p < 0.05.
Discussion
We are the first to study the relationship between MMP-9 1562C> T gene polymorphism and the development of IPF. Our results showed that TT genotype and T allele frequencies of MMP-9 1562C> T gene polymorphism were much higher in the IPF group than those in the control group, indicating that the T allele may be a risk factor of IPF.
As a chronic, progressive, fibrotic lung disease, IPF is characterized by serious morbidity, premature death, and a median survival of less than 3 years (John et al., 2013). Typical IPF symptoms include progressive breathlessness and persistent cough, which is resistant to conventional antitussive therapy (Kilduff et al., 2014). IPF occurs as a result of fibrosis of the lung parenchyma. However, the development of IPF is largely unpredictable, and the underlying molecular and cellular pathogenesis remains to be elucidated (Cottin, 2014; Wuyts et al., 2014).
As a major group of proteinases, MMPs are known to regulate the extracellular matrix remodeling and are important in the process of lung fibrosis and airway remodeling (Corbel et al., 2002). Capable of degrading various connective tissues, MMPs are believed to play an important role in parenchymal damage remodeling, resulting in tissue destruction or the induction of repair process in pulmonary diseases (Henry et al., 2002; McKeown et al., 2009). Under inflammatory conditions, the fibroblast cells as well as the infiltration of neutrophils and eosinophils can induce MMP-9 transcription (Chakrabarti and Patel, 2005).
Among all the MMPs, MMP-9 is most extensively studied in human interstitial lung diseases and lung fibrosis, due to the great sensitivity of revealing gelatinolytic activity through gelatin zymograms (Pardo and Selman, 2006). Our study provided a new idea to study the role of MMP-9 in the development of IPF, and our result provided valuable genetic information for IPF etiology.
Another result of our study showed that MMP-9 level, TIMP-1 level, and MMP-9/TIMP-1 ratio in each of the three genotype groups significantly decreased after therapy. As a kind of pleiotropic extracellular protein, TIMPs are recognized as endogenous regulators of MMPs (Moore and Crocker, 2012). High serum levels of MMP-9 and TIMP-1 are both associated with lymph node metastasis, higher tumor stage, and lower relapse-free and overall survival rates of breast cancer (Wu et al., 2008). Serum MMP-9/TIMP-1 ratio is a reliable measure of gadolinium triple-dose lesions; rIFNb-1a treatment can decrease serum MMP-9, increase serum TIMP-1, and lower serum MMP-9/TIMP-1 ratio (Avolio et al., 2005). The ratio of MMP-9/TIMP-1 can be a potent biomarker for the diagnosis and prognosis of many diseases. The ratio of MMP-9/TIMP-1 increased with the exacerbation of chronic obstructive pulmonary disease (Mercer et al., 2005). MMP-9 and TIMP-1 were detected in the serum and sputum samples of asthmatics, and the molar MMP-9/TIMP-1 ratio was found to be associated with lung function (Beeh et al., 2003). MMP-9 and TIMP-1 in the serum of patients with either small-cell lung cancer or nonsmall-cell lung cancer can reflect the pathological changes occurring in the lung (Jumper et al., 2004). Our results confirmed the efficacy of the glucocorticoid therapy on IFP patients by regulating the serum levels of MMP-9 and TIMP-1, as well as the MMP-9/TIMP-1 ratio. Additionally, before the treatment, serum levels of MMP-9 and TIMP-1 increased in the order of CC, CT, and TT genotype, with significant difference among the three genotypes. Finally, our results also found that in the CC genotype group, the proportion of the IPF patients who experienced remarkable improvement in cough, dyspnea, cyanosis, and lung crackles was significantly higher than those in the CT and TT genotype groups. In contrast, IPF patients in the CT and the TT groups had a significantly higher incidence of ostealgia, muscle atrophy, and depression than those in the CC group, indicating that patients in the CC group may have a better response to the glucocorticoid therapy than the other IPF patients.
Taken together, MMP-9 gene 1562C> T polymorphism affects the efficacy of glucocorticoid therapy in IPF patients and may be a predictor of IPF treatment outcome. The difference of the genotype and allele frequencies of MMP-9 1562C> T gene polymorphism indicates that the T allele may be a risk factor of IPF occurrence. Our study also showed that CC genotype had a better response to the glucocorticoid therapy than the other IPF patients. Our results provided a valuable clinical reference for IPF diagnosis and treatment.
Footnotes
Acknowledgments
The authors would like to thank their researchers for their hard work and reviewers for their valuable advice.
Author Disclosure Statement
No competing financial interests exist.