
Abstract
Aims: Tumor necrosis factor alpha (TNF-α) is a proinflammatory cytokine and important mediator of severity for periportal fibrosis (PPF). We hypothesized that the (-G380A) polymorphism in the TNF-α gene is associated with regression of PPF after treatment for schistosomiasis mansoni. Methods: This is a retrospective cohort study, involving 124 Brazilian patients infected with Schistosoma mansoni, who were followed for 2 years after treatment to estimate the likelihood of PPF regression. Sociodemographic and clinical factors were also identified, with emphasis on specific treatment. Results: No statistical difference was observed between sociodemographic and clinical factors among the exposed groups. Genotypes (-308) GA/AA were positively associated with the degree of PFF regression (relative risk [RR] = 0.52; ρ = 0.025), as well as in the image pattern of PPF (RR = 0.56; ρ = 0.048), when compared with the genotype (-308) GG. There was no statistical difference in TNF-α serum levels between the exposed groups. Conclusions: These results suggest that the (-G308A) polymorphism of the TNF-α gene may be one of the factors that prevents the regression of the degree and pattern of PPF in the Brazilian population, and thus it may potentially be a predictive factor of PPF intensity in schistosomiasis.
Introduction
S
The pathology resulting from infection is predominantly caused by the host's immune response to parasite eggs, which are deposited in the liver triggering a chronic granulomatous inflammation, with consequent periportal fibrosis (PPF) and obstruction of the blood flow of the intrahepatic portal vein (PV) branches (Magalhães et al., 2004; Pordeus et al., 2008). This process can lead to the development of portal hypertension, with consequent splenomegaly and appearance of varicose veins in the esophagus. Upper gastrointestinal bleeding caused by rupture of the esophageal varices occurs in 12-15% of the patients and it is the cause of death in around 20% of these cases (Andrade, 2009).
The development and severity of PPF depends mainly on several immunogenetic factors, but may also be influenced by environmental aspects. Among these factors the most cited are gender, age, parasite burden, alcoholism, and frequency and duration of exposure (Silva et al., 2013). By contrast, specific treatment for schistosomiasis may allow partial or complete reversal of PPF, and immune mechanisms may be involved in this process (Andrade, 2005; Guevara et al., 2007).
In addition, the study showed that the hepatic granulomas and the resulting PPF depended on the action of cytokines, and that the tumor necrosis factor alpha (TNF-α) played a central role (De Jesus et al., 2002; Henri et al., 2002). This cytokine is an important mediator of PPF severity. TNF-α plays a key role in the formation of granulomas through schistosomiasis infection and high levels of cytokines were significantly associated with the presence of hepatosplenomegaly and increased risk of developing severe PPF (De Jesus et al., 2002; Henri et al., 2002; Booth et al., 2004).
The TNF-α gene is located in the human leukocyte antigens class III on chromosome 6 p 21.3 (Bouzgarrou et al., 2010). Polymorphism at position -308 of the promoter region of the TNF-α gene—which involves the replacement of the guanine (G) nitrogenous base by adenine (A), the creation of two alleles (-308G and -308A) and three genotypes (GG, GA, and AA)—has been associated with an increase in the expression of TNF-α (Jrad et al., 2007; Bouzgarrou et al., 2010; Qin et al., 2010; Radwan et al., 2012).
The -308A allele is associated with increased levels of the TNF-α constituent in comparison with allele-308G (Dai et al., 2006; Jeng et al., 2007). This association is a possible explanation for the progression of hepatic fibrosis (Wilson et al., 1997). A relationship of causality between polymorphic variations that influence the expression of TNF-α and its effect on the severity of PPF in schistosomiasis needs to be better clarified (Dessein et al., 2009).
A study carried out in a Sudanese population evaluated the influence of polymorphism (-G308A) TNF-α in the severity of schistosomotic PPF, showing no evidence of major effects on the PPF (Moukoko et al., 2003). In addition, there has been no report to date of cohorts evaluating concurrent influence of polymorphism (-G308A) TNF-α on PPF regression. This study investigates the association between polymorphism (-G308A) TNF-α and PPF regression in patients with S. mansoni, after specific treatment, in endemic populations in the state of Pernambuco, Northeast of Brazil.
Material and Methods
Subjects
This is a retrospective cohort study retrieved from a previous study of 193 patients infected with S. mansoni and subjected to specific treatment for schistosomiasis, which determined polymorphism (-G308A) TNF-α and serum concentrations.
In this cohort study 124 patients were listed as being infected with S. mansoni. They were recruited in 2012 and 2013, and were followed up retrospectively for 2 years after specific treatment for schistosomiasis mansoni (SM) to estimate the probability of PPF regression. Sociodemographic and clinical factors were also identified, with emphasis on specific treatment for SM.
These patients were divided into two groups: group 1 (exposed), including 71 patients with genotypes (-308) GA or AA; and group 2 (not exposed), which included 53 patients with genotype (-308) GG. These patients were over 18 years of age and were treated in the Gastroenterology Clinic of the Hospital das Clínicas at the Federal University of Pernambuco (HC-UFPE), Recife, Brazil. All patients of this study came from endemic areas for schistosomiasis, in the state of Pernambuco, Northeast of Brazil.
This study only included patients who had undergone abdominal ultrasound, including a PPF evaluation, following the protocols of Niamey (Richter et al., 2001) and Cairo (WHO, 1993)—before treatment of schistosomiasis and also 2 years after treatment.
The outcome of interest was the regression of the ultrasound assessment of identified cases with PPF in the upper abdomen. The main exhibition was polymorphism (-G308A) TNF-α in the context of the study hypothesis, as a factor associated with PPF severity. The information about these genotypes and the serum levels of TNF-α were obtained for the years 2012 and 2013.
To determine the genotypes GG, GA, and AA, biological samples from all patients were previously subjected to polymerase chain technique for polymorphism analysis by restriction fragment (PCR-RFLP), followed by digestion through restriction of enzyme NcoI to detect the Single nucleotide polymorphism (SNP) in the promoter region of the TNF-α gene (rs1800629). This consisted of the replacement of the nitrogenous base guanine (G) by adenine (A), at position -308 (Cabrera et al., 1995), to define the exhibition groups mentioned above. Serum levels of TNF-α were measured using Enzyme Linked Immunosorbent Assay-the commercial ELISA kit (Biosource, Invitrogen Corporation, Carlsbad, CA), according to the manufacturer's instructions. The results were expressed as pg/mL, based on standard curves (sensitivity < 1.7 pg/mL).
Other explanatory variables were sex, age, contact with contaminated water, and clinical factors (caliber esophageal varices in first endoscopy, presence of gastric varices, red spots, and degree and pattern of PPF). Diameter of the spleen, PV, and splenic vein (SV) were compared before and 2 years after specific treatment for SM.
Information about these clinical variables was abstracted from medical records using a specific form, after the declaration of informed consent by the patient.
Ultrasound evaluation
The diagnoses of the clinical forms of the disease were determined by the patient's medical history and through physical examination, in addition to an evaluation by ultrasound of the upper abdomen through a single operator at the Endoscopy Unit of HC-UFPE, using a Siemens Acuson X150® equipment, with a convex transducer of 3.5 mHz—to confirm the diagnosis and exclude other liver diseases. The parameters used to define the pattern of PPF were based on the classification of Niamey (Richter et al., 2001): A, absence of fibrosis; B, dubious fibrosis; C, light; D, moderate; E, advanced; and F, very advanced. The classification of Cairo standardizes three degrees for PPF according to the average obtained from measurements of external-external diameter of three peripheral branches of the PV after the second branch: grade I > 3 the 5 mm; grade II > 5 the 7 mm; and grade III >7 mm (WHO, 1993). The parameters adopted as normal and abnormal measures for the diameters of PV, SV, and spleen size (longitudinal axis) in this study were the following: PV-normal ≤ 12 mm, abnormal > 12 mm; SV-normal ≤ 9 mm, abnormal >9 mm; spleen size longitudinal-normal ≤12 cm and abnormal > 12 cm (WHO, 1993; Richter et al., 2001).
Ethical aspects
This retrospective cohort study was part of a study that was approved by the Ethics Committee of the Center for Health Sciences at the Federal University of Pernambuco and informed consents were obtained from all patients before blood sampling (CAAE 03161512.6.0000.5208).
Statistical analysis
The follow-up period considered started from the moment in which the specific treatment was first recorded until 2 years after the treatment. Relative risk (RR) and 95% confidence interval (CI) were used by bivariate analysis to verify the association between genotype polymorphism frequencies of (-G308A) TNF-α and the regression of the degree and standard of PPF of the exposed groups—considering the regression of the degree and pattern of fibrosis as dependent variables, and the variables selected as independent. The association was considered significant when p < 0.05. For these analyses Epi-Info software version 3.5.5 (CDC, Atlanta, GA) was used. To compare the variation of TNF-α levels between the groups, we used the Kruskal-Wallis test.
Results
In a previous study, the polymorphism (-G308A) in the promoter region of the TNF-α gene and serum concentrations were determined from 193 patients. Of these, 12 were excluded because they presented Pattern A (non PPF) on the first abdominal ultrasound, and another 57 of them did not go through the 2 year follow-up after the first specific treatment for SM. Therefore, the final analysis included only 124 patients (Fig. 1).
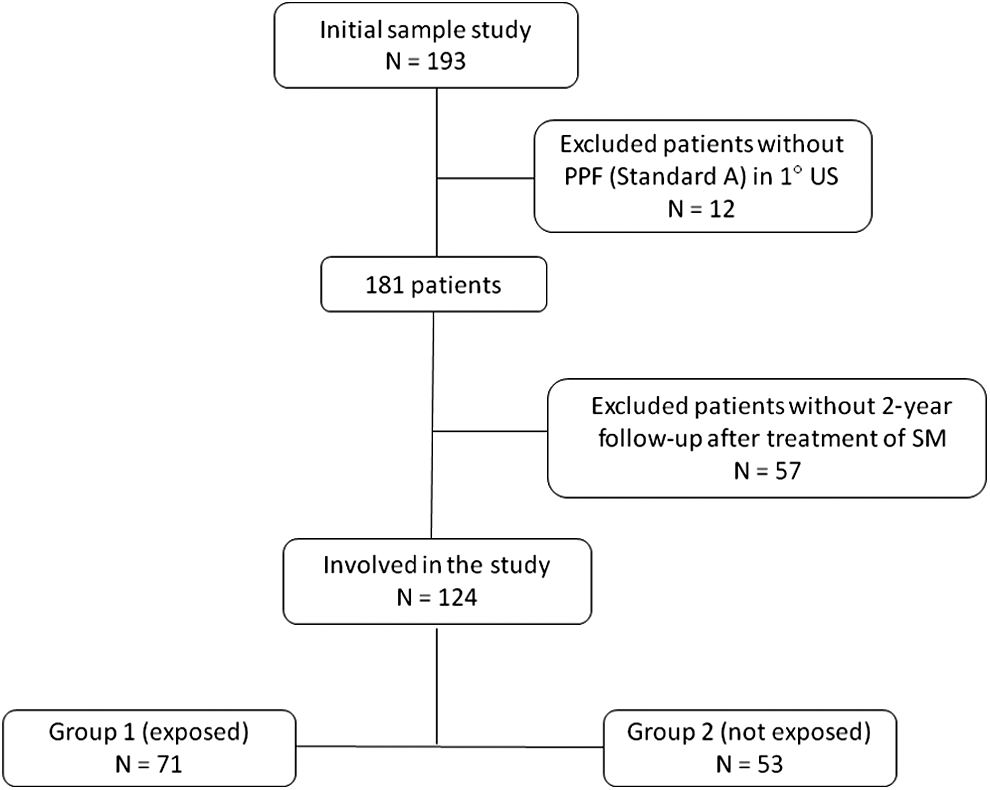
Diagram of patient eligibility.
The distribution of frequencies of the demographic and clinical variables among the exposure groups are illustrated in Table 1. In this study, the average age found among patients was 57 years (±13 years). No statistically significant difference of these factors of exposure (Table 1) was observed between the groups.
HDA, upper gastrointestinal bleeding.
Sixty-eight patients were evaluated who presented HDA.
EDA, endoscopic treatment.
Two patients from the exposed group were excluded because there was no information.
TNF-α, tumor necrosis factor alpha; TTO, treatment; n, number of individuals studied; χ2, chi-square.
Table 2 illustrates the distribution of frequencies in the two groups according to estimates of the diameters of the spleen, SV, and PV, before the specific treatment for SM and after the follow up of 2 years. The results showed no statistically significant difference between the diameters of the spleen, SV, and PV, when comparing pre and posttreatment periods.
Fifty-two patients splenectomized.
VE not displayed during examination in 8 patients and in 42 splenectomized in pre-TTO.
SV not displayed during examination in 1 patient and in 51 splenectomized in 2°years after TTO.
PV not displayed during examination (excess gases) in 8 patients in pre-TTO.
PV not displayed during examination (excess gases) in 9 patients in 2°years after TTO.
ρ-value, Chi-square; SV, splenic vein; PV, portal vein.
The association between polymorphism (-G308A) TNF-α and the regression of the degree and pattern of PPF are illustrated in Tables 3 and 4. The genotypes (-308) GA/AA showed a protective association (RR = 0.52; ρ = 0.025) for the regression of the degree of PPF and for the regression of the PPF standard (RR = 0.56; ρ = 0.048), when comparing the two groups.
One patient was excluded due to lack of information in the exposed group.
RR, relative risk; CI, confidence interval.
Two patients were excluded due to lack of information in the exposed group.
There was no significant statistical difference of average TNF-α levels between the exposure groups (Table 5).
Kruskal-Wallis test.
Discussion
This study assessed the influence of polymorphism (-G308A) TNF-α on PPF regression. This is the first article that analyzes the influence of genetic factors on PPF regression in a group of patients with SM in the state of Pernambuco, Northeast of Brazil.
Although it is well established in the literature that a number of environmental factors, including age, frequency of exposure, and parasitic load can influence the natural history of PPF (Abath et al., 2006; Arnaud et al., 2008), in this sample no statistical difference was observed among the sociodemographic and clinical factors between the exposure groups. Silva et al. (2013) evaluated 178 patients in the state of Pernambuco and stated that environmental factors, such as years of education and specific treatment, had an influence on the development of PPF. However, it is believed that the immune response, which is governed by the genetics of the host, plays a central role in the natural history of the disease.
This study involving Brazilian patients infected with S. mansoni, showed that patients with genotypes (-308) GA/AA had a protective association for regression of the degree and standard of PPF when compared with genotype (-308) GG.
The association between polymorphism (-G308A) TNF-α and hepatic fibrosis has already been extensively studied in other liver diseases (Kusumoto et al., 2006; Jeng et al., 2007; Bouzgarrou et al., 2010; Radwan et al., 2012). However, only one single study has evaluated the influence of polymorphism on the severity of PPF in schistosomiasis (Moukoko et al., 2003). Some studies found no association between this polymorphism and the severity of liver fibrosis (Moukoko et al., 2003; Kusumoto et al., 2006; Bouzgarrou et al., 2010).
Moukoko et al. (2003), observed that within the Sudanese population high levels of TNF-α were associated with higher risk of PPF, but found no evidence of association between polymorphism (-G308A) TNF-α and the severity of PPF. These authors stated that this result does not exclude the possibility that this polymorphism has an effect on the development of PPF.
Bouzgarrou et al. (2010) studied 53 Tunisian patients with chronic hepatitis C and 103 randomly selected healthy blood donor controls, matched by ethnicity and geographical area. In this study, no association was found between polymorphism (-G308A) TNF-α and liver fibrosis severity. The authors concluded that these results, although based on a small cohort, are consistent with other major studies on different ethnic populations (Powell et al., 2000; Rosen et al., 2002; Bahr et al., 2003; Goyal et al., 2004; Abbas et al., 2005), which excluded the influence of this polymorphism on the severity of Hepatitis C virus-related liver fibrosis.
Kusumoto et al. (2006) evaluated 460 patients with positive HCV and 63 healthy controls, from a hyperendemic area for HCV in Japan, and also found no significant association between this polymorphism and the severity of hepatitis. These authors concluded that polymorphism (-G308A) TNF-α can be associated with hepatic fibrosis and that these results may have been influenced by ethnic variations.
On the other hand, some studies involving patients with chronic hepatitis C confirmed the association between polymorphism (-G308A) TNF-α and liver fibrosis severity (Ho et al., 2004; Richardson et al., 2005; Feld and Liang, 2006; Schwabe and Brenner, 2006).
Jeng et al. (2007) studied 108 patients with hepatocellular carcinoma (HCC) and 108 healthy controls, matched by gender and age (±5 years), and concluded that the allele -308A TNF-α was associated with more advanced liver fibrosis, which can contribute to greater risk of HCC.
Radwan et al. (2012) studied 280 Egyptian patients with HCV (152 with cirrhosis and 128 with HCC) and 160 healthy controls, and found that polymorphism (-G308A) TNF-α was associated with risk of liver cirrhosis and HCC in patients with chronic hepatitis C.
A consensus about the influence of this polymorphism on the expression of TNF-α has not yet been established in the literature. Some studies have shown that the allele-308A was associated with increased levels of the TNF-α constituent in comparison with the allele -308G, while others failed to associate the presence of the -308A allele with different levels of TNF-α production (Wilson et al., 1997; Bayley et al., 2004; Jrad et al., 2007). This data may reinforce the hypothesis of this current study, which showed that the tested genotypes (-308) GA/AA can play an important role in the prevention of PPF regression in schistosomiasis, in the Brazilian population.
In the current study, although there was no difference of TNF-α serum levels between the exposure groups, one possible explanation for these results is that individuals with the genotypes (-308) GA/AA, possibly maintain a production of TNF-α residue after the specific treatment, contributing to less reabsorption of fibrosis in this group.
The results found in this study do not exclude the possibility of influence from other cytokines and other genes on PPF intensity. Therefore, future studies with larger samples are needed to better analyze these genotypes and their respective doses of TNF-α serum, to be able to better assess whether there is a connection between polymorphism (-G308A) TNF-α and the expression of TNF-α and PPF intensity, which may influence the regression of PPF after specific treatment of schistosomiasis. To conclude, these results suggest that polymorphism (-G308A) TNF-α can be a factor that prevents the regression of the degree and pattern of PPF in the Brazilian population, and can, therefore, potentially be a predictive factor in the severity of PPF in schistosomiasis.
Footnotes
Acknowledgments
The authors are especially thankful to the patients of the Gastroenterology Clinic of the Hospital das Clinicas/Federal University of Pernambuco, who accepted to participate, contributing with samples without direct benefit from the results, and to the laboratories of Human Molecular Genetics (University of Pernambuco) and of Virology-Immunology Laboratory Keizo-Asami (LIKA) (Federal University of Pernambuco-UFPE), where the analyses were carried out. This research study was supported by the Federal University of Pernambuco (UFPE), Brazil.
Author Disclosure Statement
No competing financial interests exist.