
Abstract
Background: Limb girdle muscular dystrophy 2A (LGMD2A) is the most frequent LGMD variant in the European population, representing about 40% of LGMD. The c.550delA mutation in the CANP3 (calcium activated neutral protease 3) gene is the most commonly reported mutation in LGMD2A. Prevalence of this mutation in the Polish population has not been previously investigated. The aim of this study was to identify and estimate the frequency of the c.550delA mutation in Polish LGMD2A patients. Methods: Polymerase chain reaction-sequencing analysis, restriction fragment length polymorphism polymerase chain reaction method. Results: We analyzed 76 families affected with LGMD and identified 62 probands with mutations in the CANP3 gene. C.550delA was the most common mutation identified, being found in 78% of the LGMD2A families. The remaining mutations observed multiple times were as follows: c.598-612del15ntd; c.2242C>T; c.418dupC; c.1356insT, listed in terms of decreasing frequency. Two novel variants in the CANP3 gene, that is, c.700G>A Gly234Arg and c.661G>A Gly221Ser were also characterized. Overall, mutations in the LGMD2A gene were estimated to be present in 81% of patients with the LGMD phenotype who were without sarcoglycans and dysferlin deficiency on immunocytochemical analysis. The frequency of the heterozygous c.550delA mutation in the healthy Polish population was estimated at 1/124. Conclusions: The c.550delA is the most frequent CANP3 mutation in the Polish population, thus sequencing of exon 4 of this gene could identify the majority of LGMD2A patients in Poland.
Introduction
LGMD2A (limb girdle muscular dystrophy type 2A) is associated with mutations in a gene coding for calcium-activated neutral protease 3 (CANP3) (Richard et al., 1995, 1997). LGMD2A is considered the most frequent LGMD variant in certain European populations (Turkey, Czech Republic, Italy, Bulgaria, Russia, and France), where it represents ∼23-42% of LGMD cases (Chrobakova et al., 2004; Fanin et al., 2005, 2009; Balci et al., 2006; Todorova et al., 2007; Guglieri et al., 2008). LGMD2A is responsible for 40% of LGMD in India (Pradhan et al., 2010), it is less frequent in Japan, China, and the United States (Nonaka et al., 2001; Moore et al., 2006; Mahmood et al., 2013). There are more than 500 different CANP3 mutations identified in the Leiden mutation database, (www.dmd.nl/capn3_home.html) that are spread over the entire gene. In certain populations, particular CANP3 mutations were found more frequently than in others (Urtasun et al., 1998; Balci et al., 2006). In some populations, the c.550delA mutation in the CANP3 gene is more prevalent (Canki-Klain et al., 2004; Milic and Canki-Klain, 2005; Balci et al., 2006; Hanisch et al., 2007; Todorova et al., 2007; Dadali et al., 2010), including in countries neighboring Poland-Russia, the Czech Republic, and Germany (Pogoda et al., 2000; Chrobakova et al., 2004; Hanisch et al., 2007; Stehlíková et al., 2014). Haplotype analysis confirmed that c.550delA is an old mutation in the European region (Milic and Canki-Klain, 2005). Due to known c.550delA prevalence in Central Europe, we presumed that it might occur frequently in Poland. Therefore, we aimed to investigate c.550delA mutation in Polish LGMD families.
Materials and Methods
Patients
Seventy-six LGMD families were included in the study. The patients presented with progressive muscle weakness affecting muscles of pelvic and/or shoulder girdle. Neither cardiac or pulmonary involvement nor mental retardation was present. Electromyography and muscle biopsy findings revealed myopathic changes in all patients. In 30 patients, normal dysferlin and sarcoglycan expression in immunocytochemical analysis was present. Calpain 3 protein analysis was not done (this method was not available at the time).
Methods
Sequence analysis of the CANP3 gene: Polymerase chain reaction (PCR) products of the CANP3 exons and the surrounding intronic sequences obtained with the primers designed previously by Richard et al. (1995) were directly sequenced on an ABI PRISM 377 automated fluorescent DNA sequencer (Applied Biosystems).
Screening for c.550delA was done using the restriction fragment length polymorphism polymerase chain reaction method (RFLP-PCR) of exon 4 of the CANP3 gene with restriction endonuclease BsaAI (New England BioLabs).
Results
CANP3 mutations were identified in 62 families. c.550delA mutation was found in homozygous and heterozygous states. It was the most common mutation, being identified in 78% of families. In 29% of families (19), c.del550A was a homozygous mutation (Fig. 1).
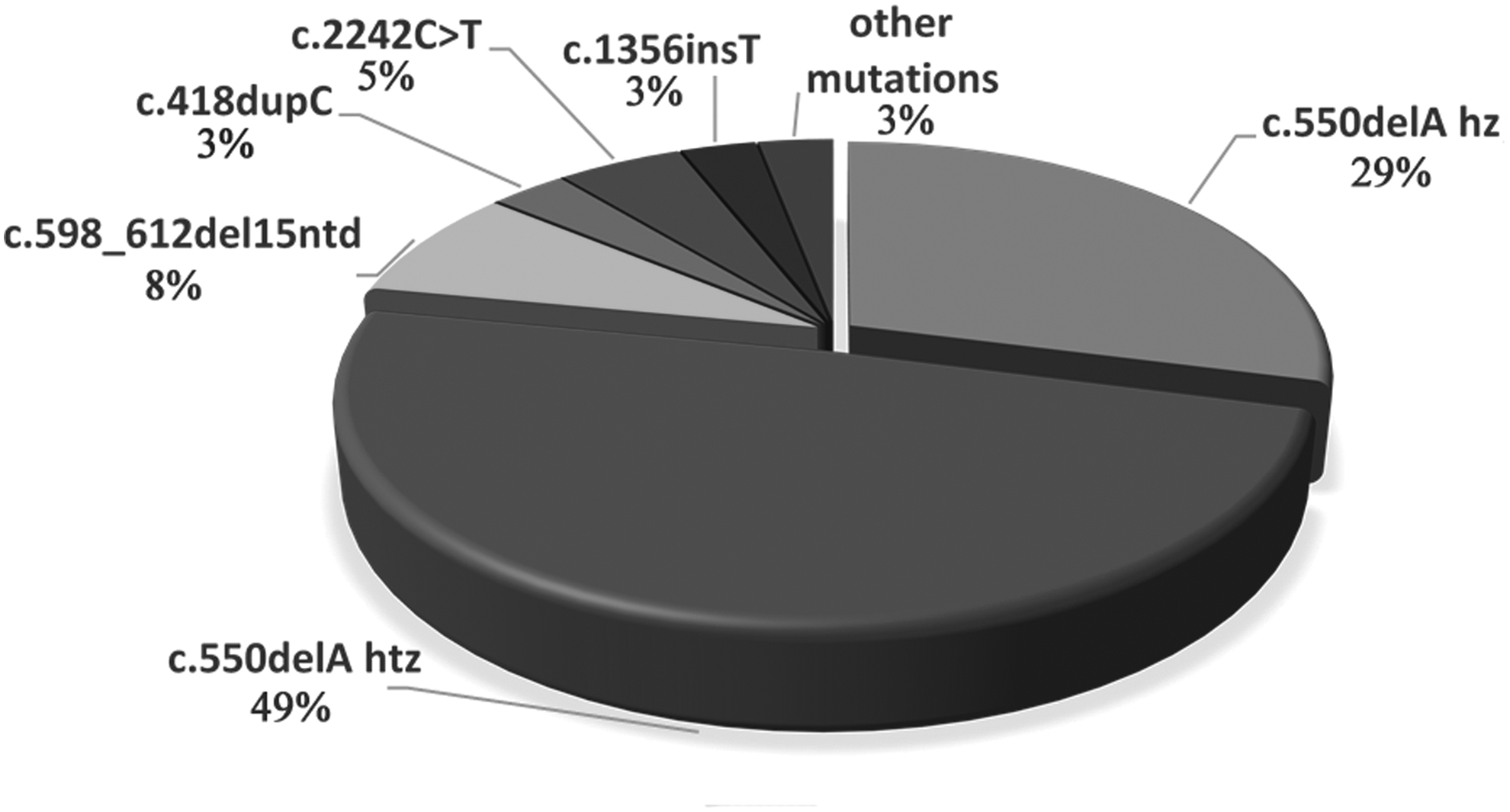
CANP3 mutation frequency in LGMD2A.
c.598-612del15ntd was the second common recurring mutation, present in five individuals on nine alleles. c.2242C>T mutation was found in three families on three alleles; c.418dupC and c.1356insT, each mutation was present in two families.
Two novel variants (c.700G>A p.Gly234Arg and c.661G>A p.Gly221Ser) in the CANP3 gene, not reported in the Leiden database, were found. The remaining mutations and the two novel variants are presented in Table 1.
(i), intron.
In the majority of cases, mutations were located in exons 3, 4, and 5. From the initial CANP3 mutation screening, we anticipated that c.550delA was relatively frequent. For rapid screening of c.550delA, RFLP-PCR of exon 4 with BsaAI endonuclease was designed. BsaAI endonuclease recognizes restriction site that is created by deletion of adenine in the position c.550 of the CANP3 gene. This assay also recognizes mutation c.598-612del15ntd (Fig. 2). Results of RFLP were consistent with the result of direct sequencing.

BsaAI RFLP of exon 4 of the CAPN3 gene in patients with c.550delA and c.598-612del15ntd mutations:
Overall, we estimated the frequency of LGMD2A in the Polish patients with LGMD phenotype at 81%. Screening for c.550delA in 248 healthy individuals revealed the carrier state in two cases, which may correspond to the estimated frequency of this mutation in the healthy Polish population at 1/124.
Discussion
LGMDs are rare disorders with prevalence ranging from 0.07 to 0.43 per 100,000 (Narayanaswami et al., 2014). Due to genetic heterogeneity and clinical similarity of different subtypes, precise LGMD diagnosis is difficult. According to recently published guidelines, LGMD diagnosis should be based on phenotype, mode of inheritance, and specific monoclonal antibodies' test results (Narayanaswami et al., 2014). Monoclonal antibodies recognize muscle proteins that are deficient in particular LGMD variants. This approach has become a powerful tool in the initial differential diagnosis of LGMD. It was partly adopted in this study with the use of antibodies against sarcoglycans and dysferlin to exclude LGMD2B, 2C, 2D, 2E and 2F. The prevalence of particular LGMD subtypes varies, depending on geographic origin and ethnic clusters. Estimations based on molecular reports indicate that the LGMD2A frequency ranges from 10% of LGMD cases in the United States to 80% in the Basque region and Russia (Urtasun et al., 1998; Pogoda et al., 2000; Moore et al., 2006; Mahmood et al., 2013). LGMD2A represents about 33% of LGMDs in the Czech Republic (Stehlíková et al., 2014).
In this study, we showed that prevalence of Polish LGMD2A was about 80% in patients with the LGMD phenotype. The c.550delA mutation identified worldwide is the most frequent mutation in the CANP3 gene, reported more than 250 times in the Leiden database www.dmd.nl/capn3_home.html. The c.550delA mutation was identified in different European populations, also in countries neighboring Poland: Russia, the Czech Republic, and Germany (Pogoda et al., 2000; Hanisch et al., 2007; Dadali et al., 2010; Stehlíková et al., 2014). In Russia, the c.550delA mutation was reported in 70% of LGMD2A patients (Dadali et al., 2010). It was present in 59% of LGMD2A families (on 47% of CANP3 mutant alleles) in the Czech Republic (Stehlíková et al., 2014). It was also occasionally found in isolated hyperCKemia in German patients (Hanisch et al., 2007).
In other European countries, the c.550delA mutation occurred with variable frequency. In Bulgaria, this variant was present in 70% of LGMD2A families (Todorova et al., 2007). In Croatia, more than 90% of the 25 examined families had the c.550delA mutation, present on 75% CANP3 alleles (Milic and Canki-Klain, 2005). In Turkey, c.550delA was found in 43% of LGMD2A families (Balci et al., 2006). However, in the United Kingdom and Spain, c.550delA is rather infrequent (Sáenz et al., 2005; Groen et al., 2007).
In Polish patients, c.550delA mutation was identified on both alleles in one-third of the families. It was present at least on one chromosome in 79% of LGMD2A families. This frequency corresponds to high c.550delA prevalence earlier reported in countries neighboring Poland. In Russia, linkage analysis with microsatellite markers flanking the LGMD2A locus revealed complete haplotype identity in most cases. This supports the possibility of a common founder (Pogoda et al., 2000). c.550delA was found to be embedded in the same haplotype on nearly 70% chromosomes in Croatia. The authors suggested that the mutation originated in the Eastern Mediterranean, from there it had expanded across Europe (Canki-Klain et al., 2004; Milic and Canki-Klain, 2005).
Two substitutions (c.700G>A, p.Gly234Arg and c.661G>A, p.Gly221Ser) found in Polish families are novel. p.Gly234 and p.Gly221 of the calpain are highly conserved amino acids across many species. Nevertheless, the two novel missense variants could not be definitely proven to be pathogenic.
There are thorough clinical and genetic evaluations of LGMD2A (Fardeau et al., 1996a, 1996b; Richard et al., 1997; Pénisson-Besnier et al., 1998; Urtasun et al., 1998; Chou et al., 1999). The phenotypes include patients with upper girdle in Erb LGMD or lower girdle in Leyden-Mobius LGMD (Angelini et al., 2010). In the studied group, both phenotypes were present. Marked scapular involvement with severe scapular winging in 10 patients made us to include facioscapulohumeral muscular dystrophy (FSHD) in the differential diagnosis. FSHD was excluded by genetic analysis (with P13E11 probe) in three cases, in whom further molecular testing revealed homozygous CANP3 mutations.
The c.550delA frequency in the healthy Polish population (1/124) is similar to the previously reported frequency of this mutation in other populations, estimated at 1/150-1/133 (Pogoda et al., 2000; Canki-Klain et al., 2004).
The results of this study are consistent with previous reports showing high frequency of LGMD2A among other LGMDs and high frequency of c.550delA mutation in LGMD2A in several European populations. We found that c.550delA is the most prevalent mutation in Polish LGMD2A. Rapid screening for c.550delA and c.598-612del15ntd mutations with BsaAI RFLP or sequencing of CANP3 exon 4 could enable identification of molecular defect in more than 80% of LGMD2A families. Due to genetic heterogeneity of LGMDs, epidemiologic data for the most frequent LGMD subtypes in different geographic regions and identification of particular recurrent mutations are mandatory for scheduling diagnostic procedures. The results of this study would be helpful in establishing screening of the LGMD2A strategy in Poland.
Footnotes
Acknowledgment
This study was performed with the approval of the appropriate local ethics committee.
Author Disclosure Statement
No competing financial interests exist.