
Abstract
Aims: Parathyroid hormone (PTH) levels are useful as a prognostic factor of chronic heart failure (HF) and can predict hospitalization for HF. It is unknown whether serum PTH levels in hospitalized patients with HF can predict discharge and if admission, discharge, or change from admission to discharge PTH measure is the most important predictor of readmission and/or death.Methods: A total of 125 consecutive hospitalized patients with HF were enrolled into this study. The receiver operating characteristic (ROC) curves indicated the predicted values of PTH for readmission due to HF and the optimal cutoff points of PTH levels for discharge. The binary logistic regression model indicated an association between PTH levels and readmission due to HF.Results: The PTH level on admission was positively correlated with the New York Heart Association class and N-terminal pro-B-type natriuretic peptide level. The ROC curves showed that the PTH level at discharge (PTHdis) was of predictive value for readmission within 1 year due to HF. A PTHdis level <45.2 pg/mL was the best cutoff point for discharge, with a sensitivity of 72.1%, specificity of 61.5%, and area under the ROC curve of 0.693 (95% confidence interval [CI] 0.598-0.788). The results of logistic regression analysis showed that PTHdis had an odds ratio of 1.035 for readmission due to HF (95% CI 1.005-1.067).Conclusion: Serum PTH levels in hospitalized patients with HF were shown to be an independent predictor of discharge and PTHdis was the best predictor of readmission and/or death within 1 year due to HF.
Introduction
T
In recent years, it has been proven that parathyroid hormone (PTH) also plays an important role in cardiovascular diseases, including hypertension, left ventricular hypertrophy, arteriosclerosis, and valvular calcification, among others (Cha et al., 2010; Klarić et al., 2011; Bosworth et al., 2013; Demir et al., 2013), and it is particularly associated with HF (Sugimoto et al., 2013). In addition, PTH is well correlated with either HF with normal ejection fraction (EF) or with progressive HF (Altay et al., 2012, 2013). Some studies reported that PTH levels could predict hospitalization for HF in outpatients (Sugimoto et al., 2009). However, till date, there are limited data on the correlation between PTH levels and HF in the Chinese Han population, especially on the role of PTH in predicting discharge.
Therefore, the objective of this study was to evaluate the predicted value of serum PTH level in the illness conditions of Chinese Han patients with HF and whether it can be used to predict the timing of discharge, readmission, and/or death within 1 year due to HF.
Materials and Methods
Patients
The clinical data of 915 patients with chronic HF hospitalized between March 2011 and February 2014 were retrospectively analyzed, and chronic HF was diagnosed according to the ESC guidelines for the diagnosis and treatment of acute and chronic HF 2008 (Dickstein et al., 2008). The underlying causes of HF included coronary heart disease, hypertension, cardiomyopathy, and valvular heart disease. Patients with serum creatinine level ≥265 μM or transaminase level >3 times the upper limit of the normal value and with known medical history of skeletal system diseases, respiratory diseases, cancer, and rheumatic diseases were excluded. The patients with primary parathyroid diseases diagnosed with high-frequency color Doppler ultrasound were also rejected. Therefore, 125 cases were included in this study.
Research methods
General information analysis: On admission, blood pressure (BP) and weight were assessed, and 12-lead electrocardiography was performed in all hospitalized patients. The levels of serum creatinine, electrolytes, total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), triglycerides (TG), fasting blood glucose (FBG), and C-reactive protein (CRP) were measured using an automatic biochemical analyzer (Olympus).
Evaluation of cardiac function: The cardiac function of all hospitalized patients was evaluated according to the New York Heart Association (NYHA) functional classification. All patients presented clinical symptoms and were classified as NYHA classes II, III, and IV.
Measurement of serum PTH levels: Immediately after admission and within 48 h before discharge, a 3-mL venous blood sample was collected and stored at −20°C. Serum PTH levels were assessed using a chemiluminescent method (PTH ELISA kit; Dian Diagnostics Co, Ltd). The normal range established for this assay was 14-72 pg/mL.
Measurement of plasma N-terminal pro-B-type natriuretic peptide levels: Immediately after admission and within 48 h before discharge, plasma N-terminal pro-B-type natriuretic peptide (NT-proBNP) levels were assessed using a quantitative immunofluorescence method (NT-proBNP assay kit; Getein Biotechnology Co, Ltd.).
Glomerular filtration rate: Glomerular filtration rate (GFR) was calculated using the following formula: GFR (mL/min/1.73 m2) = (140 - age) × weight/0.818 × creatinine concentration (μM), and the value for women was scaled to 0.85 (Cvan et al., 2015).
Six-minute walk test (ATS, 2002): To evaluate the cardiopulmonary function, the patients were required to complete the 6-minute walk test in the ward corridor on admission. The length of the corridor was 50 m and the patient was instructed to complete 6 minutes of shuttle walk. The speed was controlled by the subjects themselves and short breaks were allowed when the patients felt tired or experienced chest pain. The walking distances were recorded by the examiners.
Doppler echocardiography: Doppler echocardiography was performed using a Doppler ultrasound apparatus (vivid E9; General Electric Corp.) within 48 h after admission, and the left atrial diameter, left ventricular end-diastolic diameter, right atrial diameter, right ventricular end-diastolic diameter, and left ventricular EF were recorded.
Therapeutic regimen: For patients with no contraindications, angiotensin-converting enzyme inhibitors and β-blockers were administrated. Angiotensin receptor antagonist was used for patients with dry cough and those who could not tolerate angiotensin-converting enzyme inhibitors. Moreover, diuretics, digitalis preparations, and aldosterone receptor antagonist were administered with discretion.
Discharge criteria: Patients were discharged when clinical remission was achieved and when stable for more than 3 days.
Study endpoints: All patients were monitored for up to 1 year after discharge in the clinic or by telephone. Readmission due to HF or death from any cause within 1 year was recorded.
Ethics statement
The Medical Ethics Committee of No. 101 Hospital of PLA approved this retrospective study under protocol No. 20140105. Each patient signed a written consent form so that their information could be stored in the hospital database and used in the analysis.
Statistical analyses
Continuous variables were expressed as means and standard deviation, and analysis of variance (ANOVA) and least significant difference (LSD) were applied to compare the differences between the groups. Categorical variables were expressed as frequency and percentage and a chi-square test was applied to compare the differences between the groups.
Correlation analysis was performed using Pearson correlation and Spearman rank correlation. Receiver operating characteristic (ROC) curves were calculated to assess the predictive value of PTH for discharge and readmission, and the optimal cutoff point of PTH for discharge was selected to be the PTH value with the maximum sum of sensitivity and specificity. A Z-test was applied to compare area under the curves (AUC) of each parameter. Age, NT-proBNP levels, PTH levels, estimated GFR, left ventricular EF, and 6-minute walking distances were further entered into a binary logistic regression analysis model to identify independent predictors of readmission due to HF. Hazard ratios were calculated with 95% confidence intervals (CIs). Kaplan-Meier survival curves were calculated to evaluate the prognostic value of PTH.
A p-value <0.05 was considered statistically significant. All statistical analyses were performed using SPSS software version 13.0.
Results
General data analysis
A total of 52 men and 73 women were enrolled in this study, with an average age of 74.98 ± 11.81 years. The median follow-up period was 169 (2-365) days. The average serum PTH level was 111.66 ± 62.00 (34.50-365.30) pg/mL on admission and 68.24 ± 50.29 (5.00-275.00) pg/mL at discharge.
The cardiac function of all patients was classified according to the NYHA functional classification, and all patients were divided into three groups. The incidence of diabetes was significantly different between the three groups (Table 1). As shown in Table 2, the higher the NYHA class was, the higher was the PTH level on admission (PTHadm) and the lower were the 6-minute walking distance, GFR, and EF levels (p < 0.05). No significant differences in age, BP, electrolytes, FBG, TC, LDL-C, HDL-C, TG, CRP, PTH level at discharge (PTHdis), and cardiac chamber size were observed between the groups (p > 0.05).
A chi-square test was performed.
NYHA, New York Heart Association.
ANOVA and LSD were performed.
ANOVA, analysis of variance; CRP, C-reactive protein; DBP, diastolic blood pressure; EF, left ventricular ejection fraction; FPG, fasting blood glucose; GFR, glomerular filtration rate; HDL-C, high-density lipoprotein cholesterol; LAD, left atrial diameter; LDL-C, low-density lipoprotein cholesterol; LSD, least significant difference; LVEDD, left ventricular end-diastolic diameter; PTHadm, parathyroid hormone level on admission; PTHdis, parathyroid hormone level at discharge; RAD, right atrial diameter; RVEDD, right ventricular end-diastolic diameter; SBP, systolic blood pressure; TC, total cholesterol; TG, triglycerides.
The correlations of PTH levels with NYHA class, NT-proBNP level, EF, and the 6-minute walking distance
As shown in Table 3, on admission, the PTH level was positively correlated with the NYHA class and NT-proBNP level (rs = 0.233 and r = 0.244, respectively, p < 0.01) and negatively correlated with the EF value and 6-minute walking distance (r = −0.690 and r = −0.439, respectively, p = 0.000).
Pearson correlation and Spearman rank correlation (in bold) were performed.
EF, ejection fraction; NT-proBNP, N-terminal pro-B-type natriuretic peptide; PTH, parathyroid hormone.
The predictive value of each parameter for readmission within 1 year due to HF
ROC curves were constructed to evaluate the predictive value of the following parameters for readmission within 1 year due to HF: PTHadm, PTHdis, PTH ratio (PTHadm/PTHdis), PTH difference (PTHdis − PTHadm), NT-proBNP level on admission (NT-proBNPadm), NT-proBNP level at discharge (NT-proBNPdis), and the NT-proBNP difference (NT-proBNPdis − NT-proBNPadm). Our results showed that all the parameters were of predictive value except PTHadm and NT-proBNP difference. In addition, the AUC of PTHdis had the largest predictive value (0.693) among all the PTH parameters (Table 4 and Fig. 1). The Z-analysis indicated no significant differences considering the AUC of the five parameters (p > 0.05).
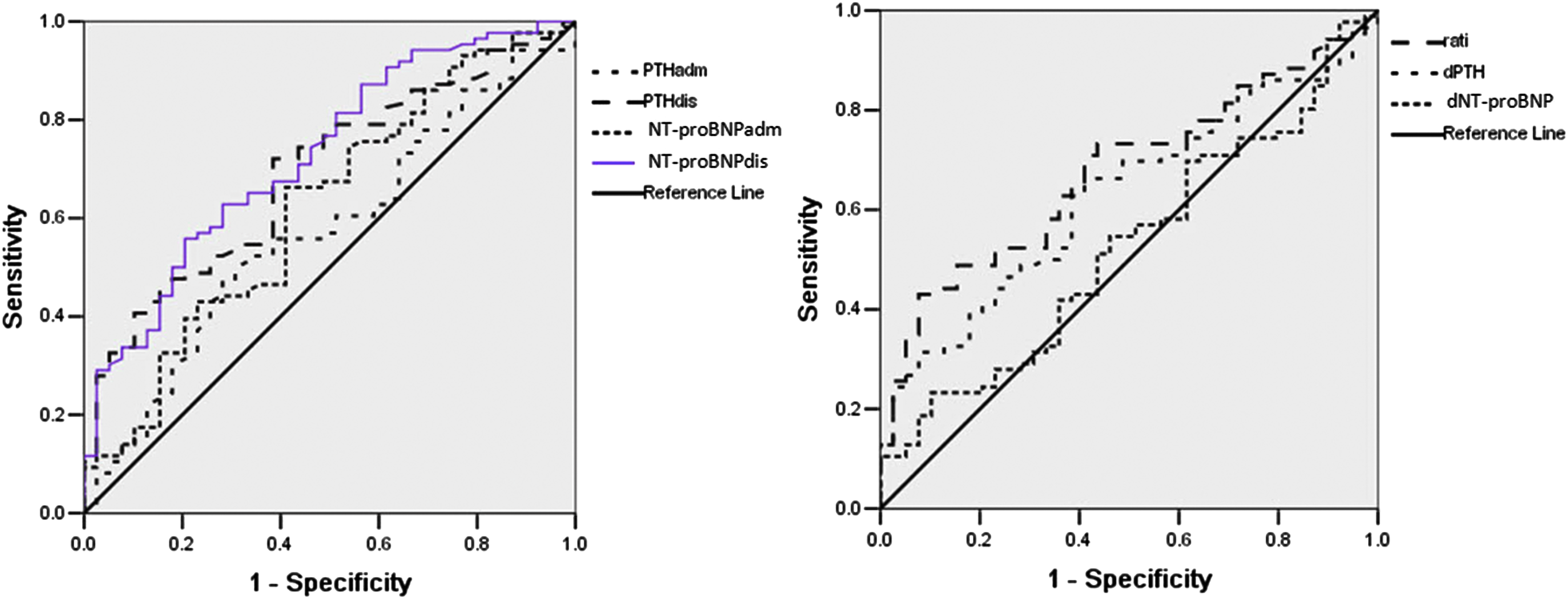
Receiver operating characteristic curves of each parameter for readmission due to heart failure within 1 year. dNT-proBNP, the NTproBNP difference (NT-proBNPdis − NT-proBNPadm); dPTH, the PTH difference (PTHdis − PTHadm); NT-proBNPadm, Nterminal pro-B-type natriuretic peptide level on admission; NT-proBNPdis, NT-proBNP level at discharge; PTHadm, parathyroid hormone level on admission; PTHdis, PTH level at discharge; ratio, the PTH ratio (PTHadm/PTHdis). Color images available online at www.liebertpub.com/gtmb
ROC curves were calculated.
AUC, area under the curve; CI, confidence interval; dNT-proBNP, the difference of NT-proBNP (NT-proBNPdis − NT-proBNPadm); dPTH, the difference of PTH (PTHdis − PTHadm); NLR, negative likelihood ratio; NPV, negative predictive value; NT-proBNPadm, NT-proBNP level on admission; NT-proBNPdis, NT-proBNP level at discharge; PLR, positive likelihood ratio; PPV, positive predictive value; PTH ratio, PTHadm/PTHdis; PTHadm, PTH level on admission; ROC, receiver operating characteristic.
In addition, age, NT-proBNP levels, PTH levels, estimated GFR, left ventricular EF, and the 6-minute walking distance were entered into a binary logistic regression analysis model to identify independent predictors of readmission due to HF. The results showed that PTHdis (odds ratio [OR] = 1.035, 95% CI 1.005-1.067) and NT-proBNPdis (OR = 1.003, 95% CI 1.001-1.005) were independent predictors of readmission due to HF, whereas EF (OR = 0.874, 95% CI 0.793-0.964) was a protective factor for readmission due to HF (Table 5).
A binary logistic regression analysis model was performed.
OR, odds ratio.
PTH level for predicting the best period of discharge
Taking the period of discharge of patients not readmitted within 1 year due to HF as the best time for discharge, the best cutoff point of PTHdis was 45.2 pg/mL, with a sensitivity of 72.1%, specificity of 61.5%, and AUC of 0.693 (95% CI 0.598-0.788).
PTH level for predicting the outcome of HF
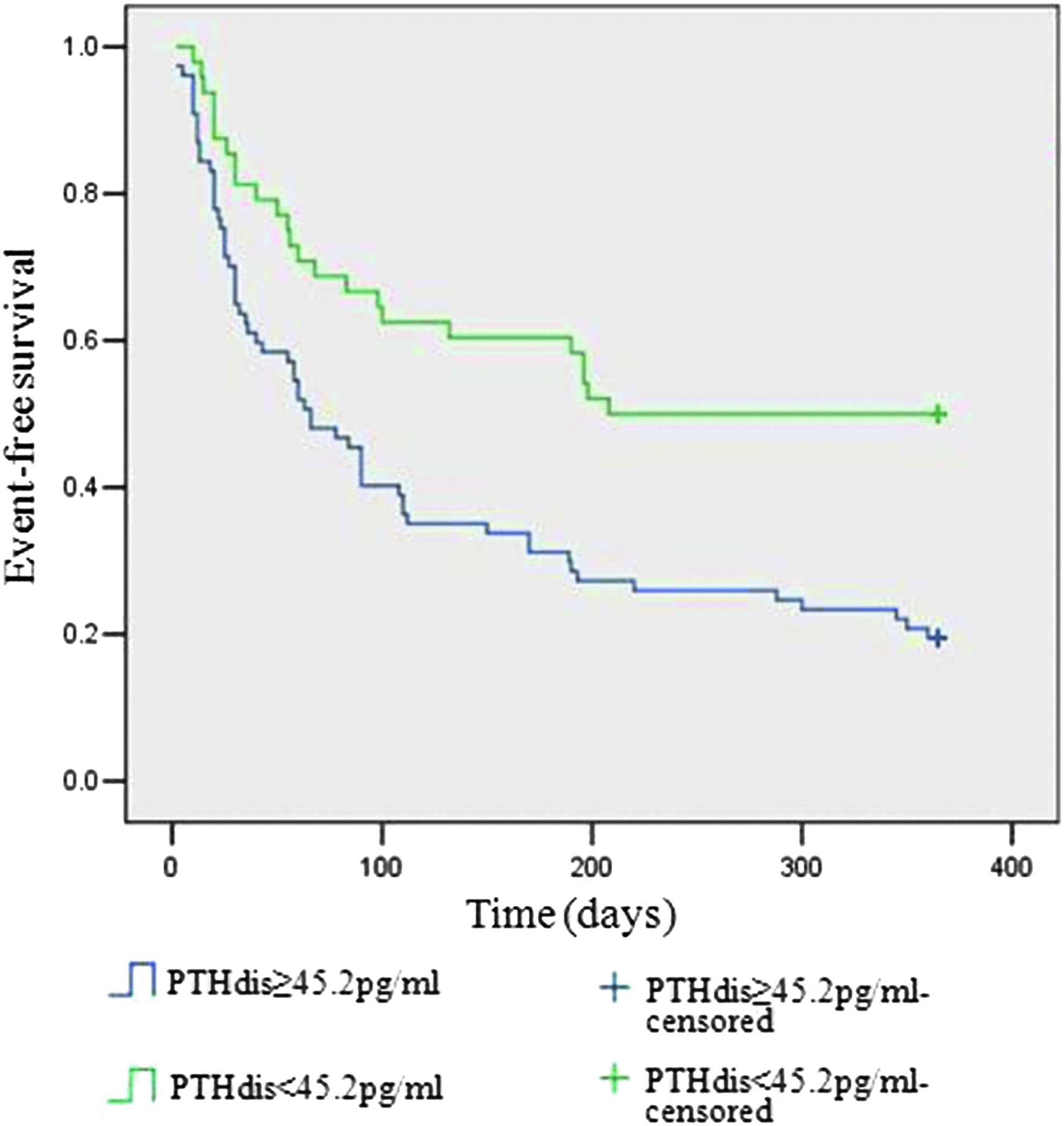
During the 1-year follow-up period, 86 patients (68.8%) were readmitted due to HF and 8 patients (6.40%) died (6 cases due to deteriorated HF, 2 cases due to malignant arrhythmia, and one case due to unknown reason). Considering the results of the ROC analysis, PTHdis, PTH difference, and PTH ratio can be used to predict readmission within 1 year due to HF. The Kaplan-Meier survival analysis indicated that the intervals from discharge to readmission or death were smaller for patients with PTHdis ≥45.2 pg/mL compared with those with PTHdis <45.2 pg/mL (Figs. 2 and 3).

Kaplan-Meier curve showing readmission for heart failure within 1 year free survival, according to PTHdis. Color images available online at www.liebertpub.com/gtmb
Kaplan-Meier curve showing readmission and (or) death for heart failure within 1 year free survival, according to PTHdis. Color images available online at www.liebertpub.com/gtmb
Discussion
PTH is an 84-amino acid linear peptide secreted by the parathyroid chief cells and is the main regulator of calcium and phosphorus metabolism in vivo. Animal experiments have shown that this hormone can alter the intracellular calcium gradient, enhance coronary blood flow, change myocardial self-discipline, and affect cardiac function (Hara et al., 1997; Andersson et al., 2004; Osto et al., 2012). Furthermore, PTH plays an important role in the development of left ventricular hypertrophy and coronary heart disease.
Excessive pressure loads or myocardial ischemia and hypoxia may be the underlying mechanisms for PTH release (Meyer et al., 2007), that is, increased intraventricular pressure and myocardial ischemia may lead to increased serum PTH level. During HF, increased ventricular end-diastolic pressure may lead to pulmonary congestion and decreased coronary blood flow, resulting in myocardial ischemia and hypoxia. All of these factors can be the cause of increased serum PTH levels.
In addition, hypocalcemia is one of the important factors that provoke the parathyroid glands to release PTH (Borkowski et al., 2011). During HF, the activation of renin-angiotensin-aldosterone system with a resultant elevation in circulating aldosterone is usually accompanied by marked excretory wasting of calcium in both feces and urine leading to ionized hypocalcemia. As a result, the calcium-sensing receptor of the parathyroids is provoked to release PTH (Khouzam et al., 2006; Laguardia et al., 2006). Recent studies have shown that even after considering the established risk factors and other variables, including mineral metabolism, serum PTH levels can still predict the occurrence of overall HF and nonischemic HF (Emil et al., 2009).
Therefore, PTH levels can be used in the risk stratification of HF and to guide individualized treatment (Gruson et al., 2014). However, till date, there is little information about the predictive value of PTH for assessing the optimal timing of discharge and readmission.
NT-proBNP is a 76-amino acid polypeptide synthesized by the cardiac cells and primarily expressed in the ventricle. The increase in left ventricular pressure triggers stress response mechanisms in myocardial cells and results in the synthesis and release of NT-proBNP. Therefore, BNP is a recognized indicator for the diagnosis and prognosis of HF. In addition, it can be used to predict readmission or mortality (Wu et al., 2006; Robb et al., 2011; Savarese et al., 2014) and has been included in the guidelines for the management of chronic HF.
Our results showed that PTH and NT-proBNP levels were significantly higher in patients with higher NYHA class and that these levels decreased accordingly with the improvement of cardiac function. Besides, the walking distance was shorter in patients with higher PTH levels, and there was a significant correlation between the PTH level and walking distance. The left ventricular EF is the main indicator of cardiac function. Our results showed a negative correlation between PTH and left ventricular EF. Therefore, the PTH level was well correlated with subjective and objective indicators of HF and is important in predicting the outcome of HF.
Previous studies have revealed that the PTH level is closely associated with mortality and severity of illness in patients with HF in the emergency department (Carlstedt et al., 1997). Accordingly, the present study showed the prognostic value of PTH in hospitalized patients with HF. In addition, the results of the ROC analysis indicated that the AUC of PTHdis for the prediction of readmission was 0.693, which was similar to the AUC of NT-proBNPadm and NT-proBNPdis (0.622 and 0.727, respectively), but the differences were not significant.
Similarly, the binary logistic regressive analysis model demonstrated the independent predictive value of PTHdis for readmission due to HF, corroborating that PTH is of predictive value for readmission due to HF. The best cutoff point of PTH for discharge was 45.2 pg/mL, with a sensitivity of 72.1% and specificity of 61.5%, and this value can be adopted as a discharge criterion. The Kaplan-Meier survival analysis indicated that the asymptomatic survival period of patients with PTHdis <45.2 pg/mL was significantly higher than that of patients with PTHdis ≥45.2 pg/mL, which further confirms the prognostic importance of PTH.
One of the limitations of this study was that the underlying causes of HF were not identified for the study group and that the patients with diastolic or systolic HF were not distinguished. Second, the data analyzed were simplified, PTH and NT-proBNP levels on admission and discharge were detectable, whereas the 6-minute walk test and Doppler echocardiography were not performed at discharge. Third, more objective indicators of cardiac function, such as left ventricular filling pressure, were not analyzed in this study. The primary endpoints of the study were its relative simplicity, retrospective nature, and small sample size. Therefore, this study can only indicate crude trends. Further studies should be conducted to explore the mechanisms underlying the increase in PTH levels after HF.
In short, serum PTH levels obtained in hospitalized patients with HF were shown to be an independent predictor of discharge and PTHdis best predicts readmission and/or death within 1 year due to HF.
Footnotes
Acknowledgment
G.W and G.Z. are currently receiving a grant (No. 81371657) from the National Natural Science Fund of China (NSFC).
Author Disclosure Statement
No competing financial interests exist.